%20for%2018,19,%205.8x4(2)%20for%2020.jpg)
|
|
|
|
|
|
|
|
Osteotomy Perpendicular to Cortex
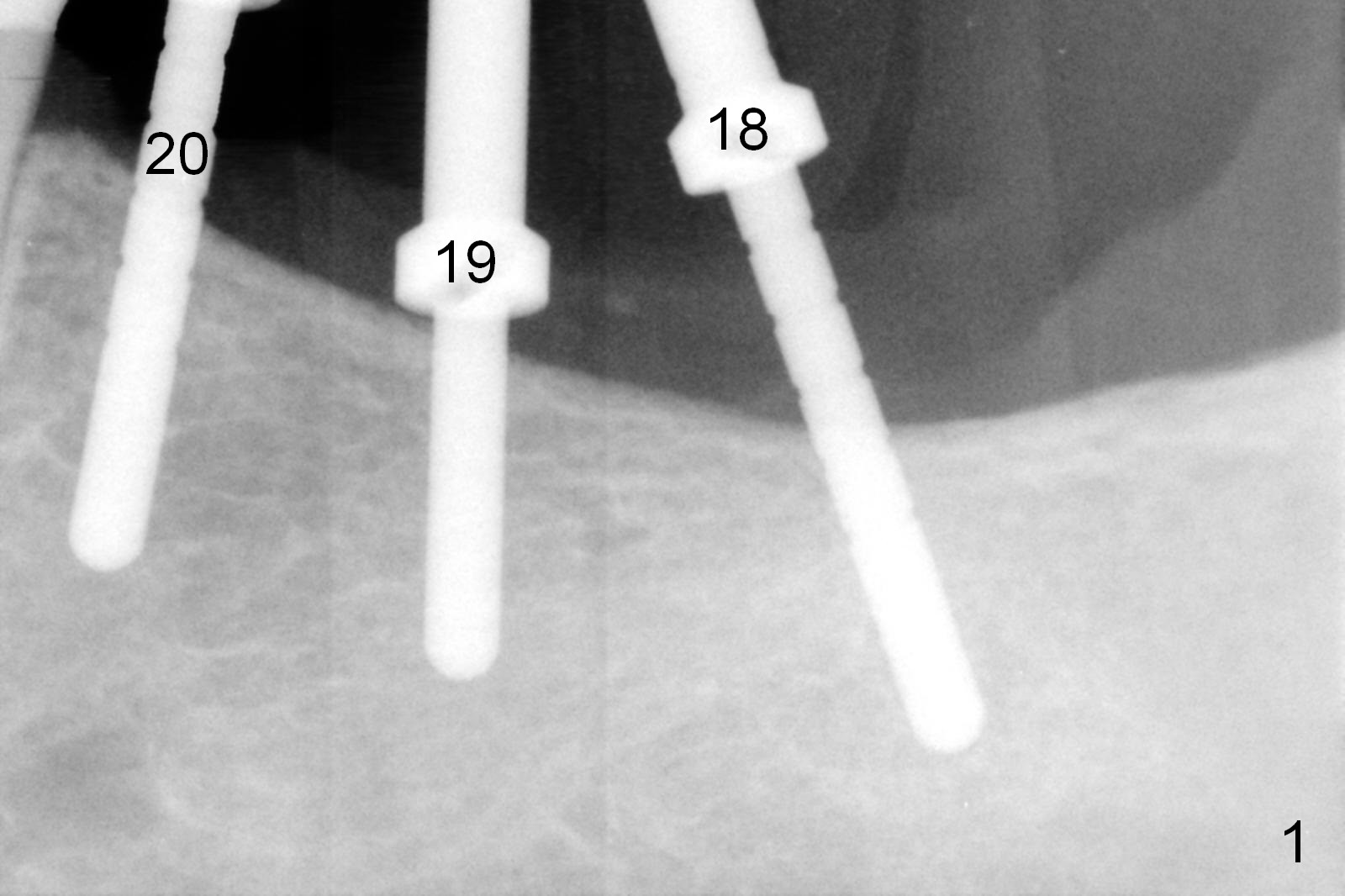
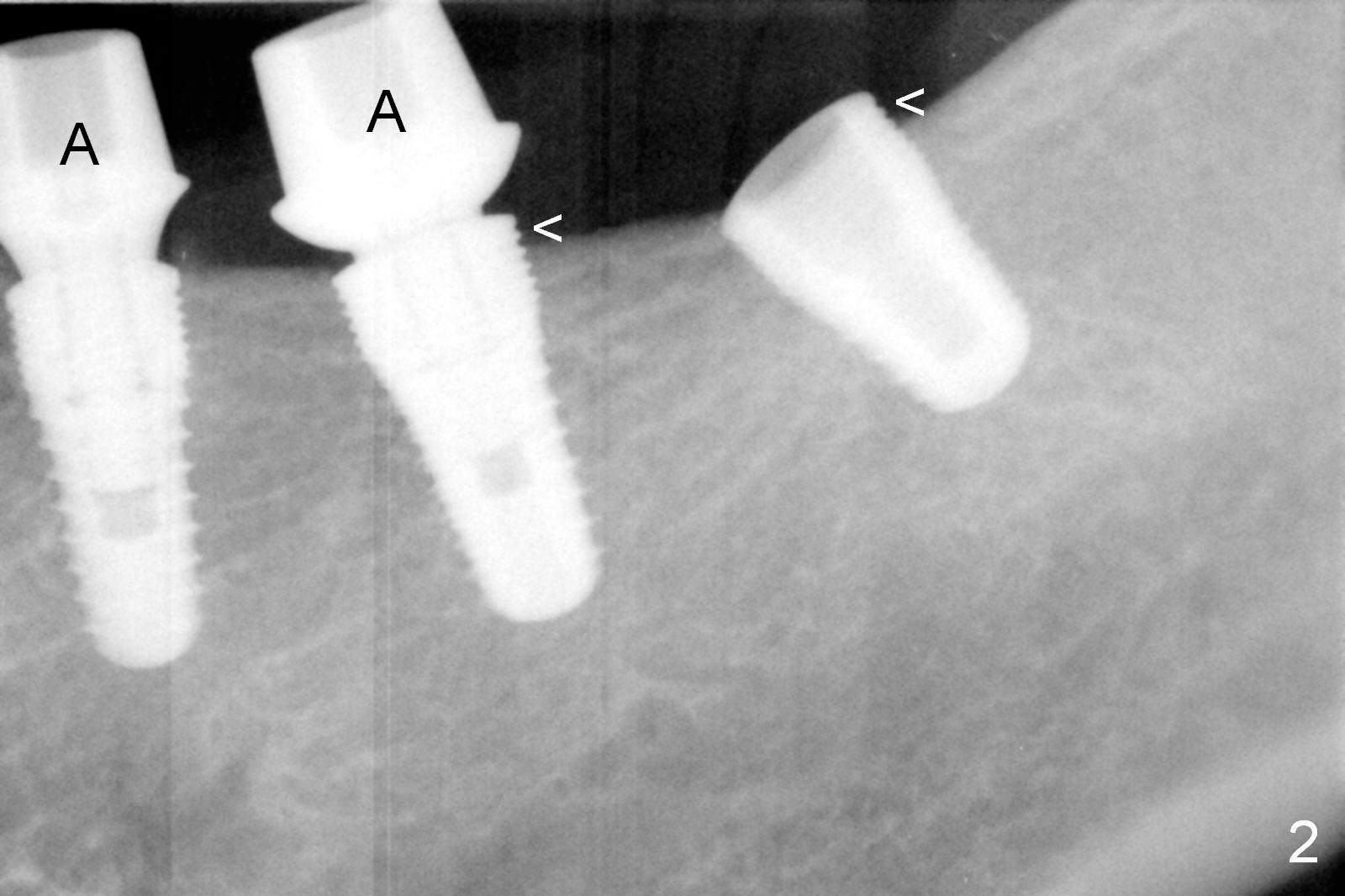
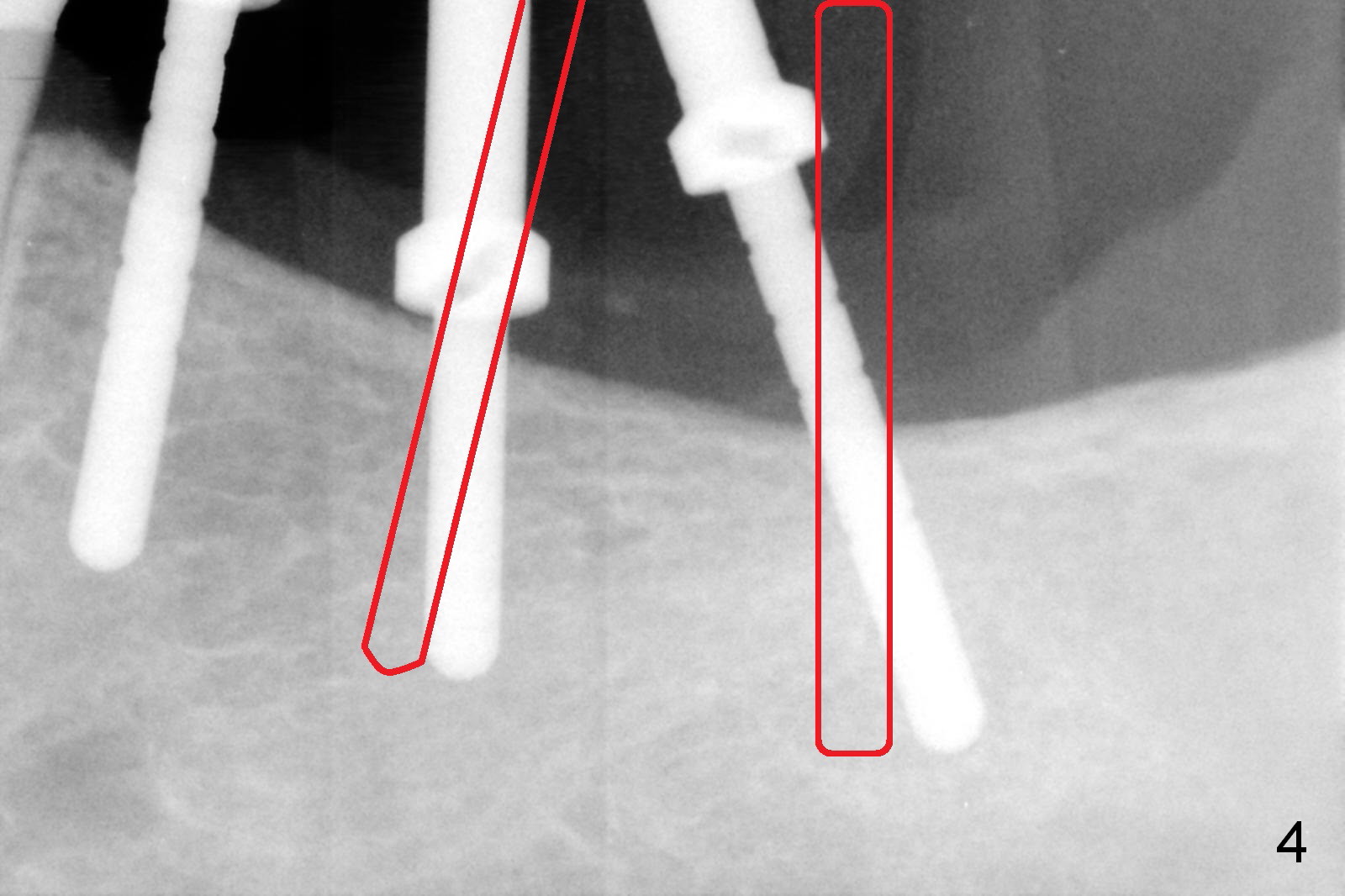
Osteotomy at the site of #18-20 is initiated using a surgical stent (Fig.1). When implants are placed (5.3x8, 5x10, 4.5x10 mm at #18-20, respectively), the distal threads are exposed excessively at #18 and 19 (Fig.2 <). In addition, the implant at #19 tilts buccally. The implants at at #18 and 19 are removed, the last drills are re-used to change the trajectory. When the implants are placed, they are levels with the cortex (Fig.3 ^). The drawback is decrease in insertion torque. More ideally, the trajectory problem should be detected at the early osteotomy stage (Fig.1) and corrected (Fig.4 red lines). In one word, the initial osteotomy should be perpendicular to the cortex.
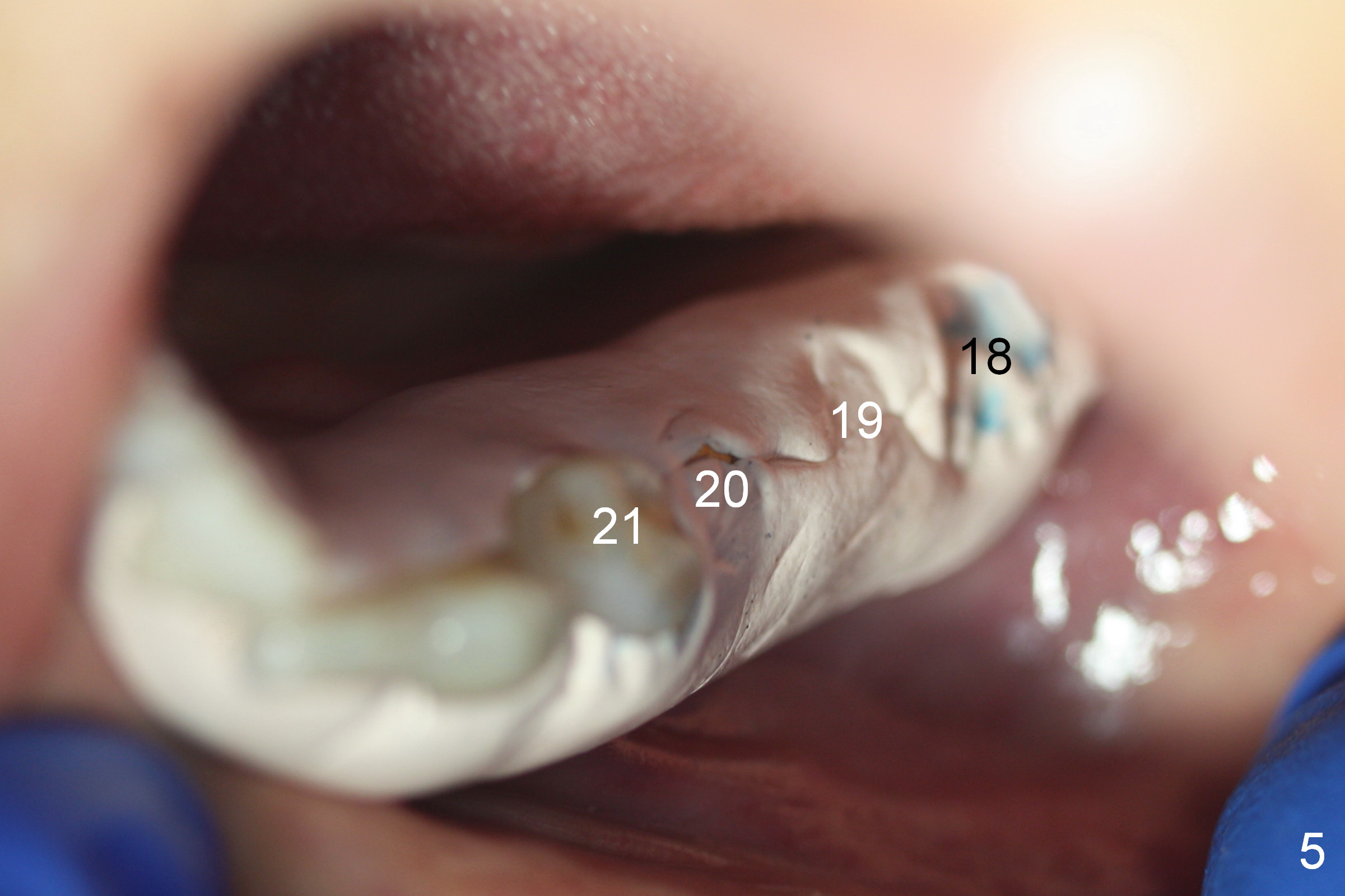
Immediate placement of abutments (Fig.2,3 A: 6.8x4(20, 5.8x4(2) mm) allows detection of buccolingual trajectory issue intraoperatively and early fixation. Due to decreased insertion torque and more importantly #15 supraeruption/lack of interocclusal space, immediate provisional is postponed. Periodontal dressing is applied around the abutments for increased retention (Fig.5); through the dressing, it appears that implant placement alignment is acceptable (#18-20).
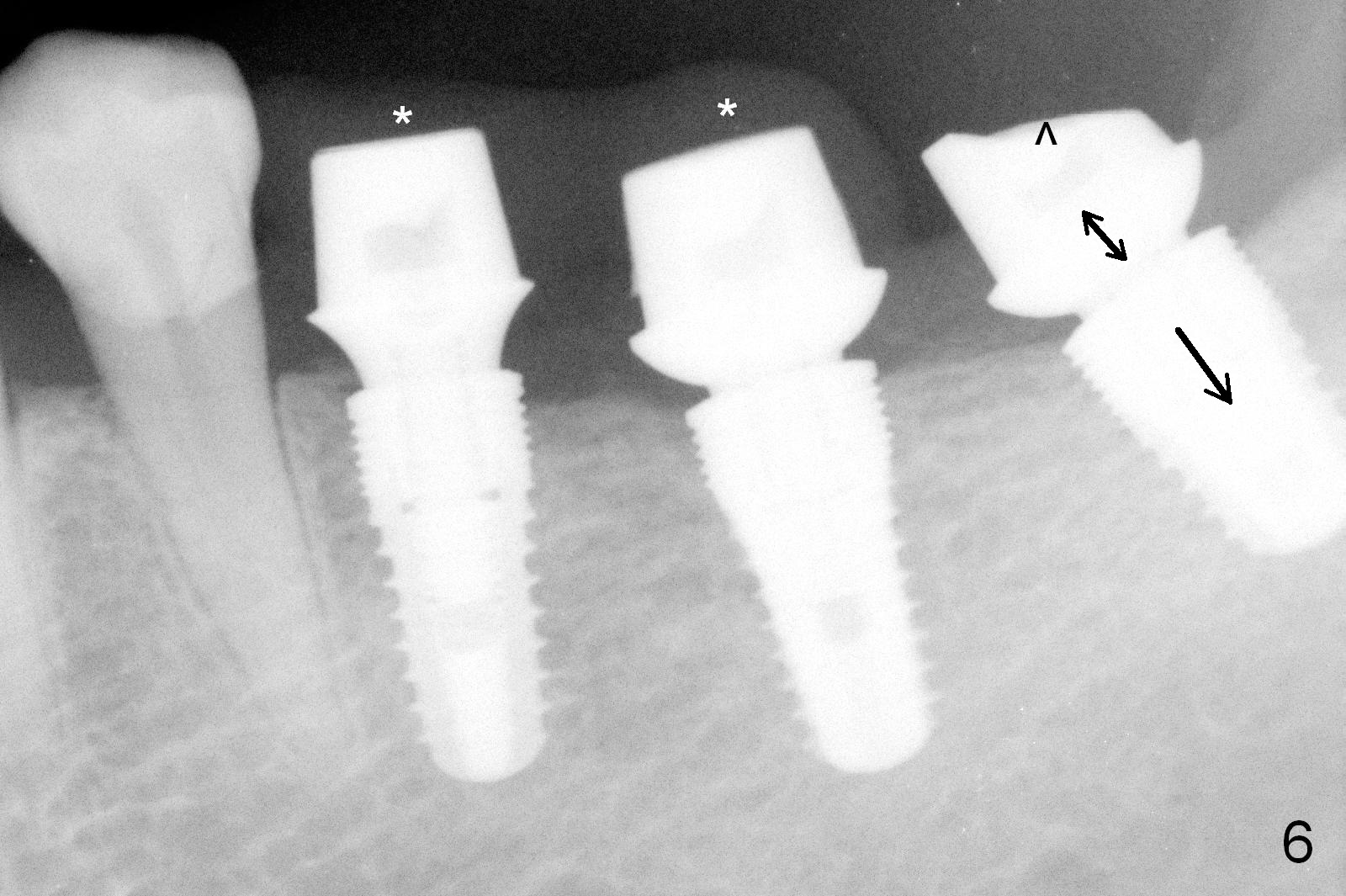
Early provisional is provided when the dressing dislodges. The tooth #15 will be intruded orthodontically using mini-implants. In fact a splinted provisional is fabricated at #19 and 20 (Fig.6 (PA taken 3 months postop) *). In spite of heavy reduction in abutment height at #18 (^), there is not enough clearance for provisional. The implant should have been placed deeper (single arrow), while the cuff height (double arrows) shorter.
Return to Lower Arch
Reconstruction,
Implant & Ortho
2
Xin Wei, DDS, PhD, MS 1st edition 09/16/2015, last revision 04/30/2017