






|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Sticks to What You Believe
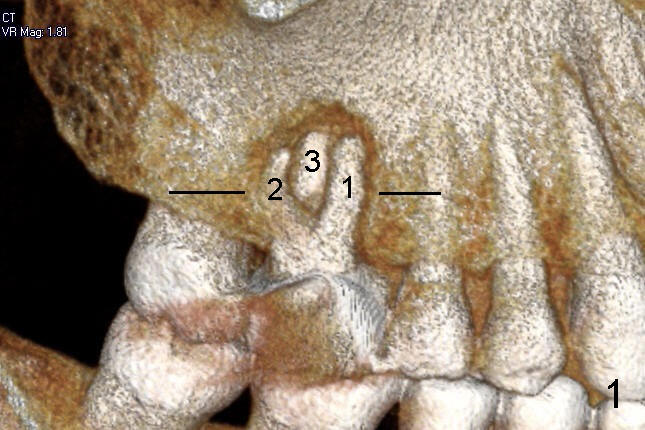
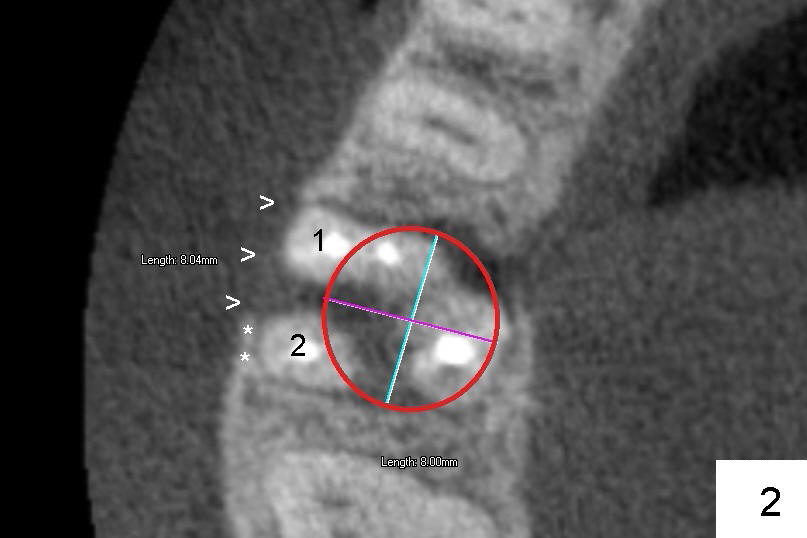
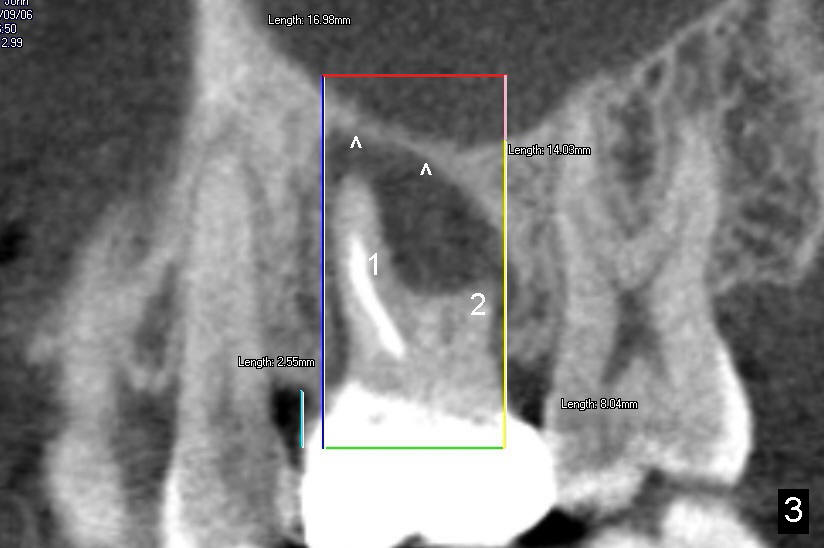
The tooth #3 of a 40-year-old man has endo failure (Fig.1-4) with resorption of the mesiobuccal plate (Fig.2). Ideally a 8x17 mm cylindrical implant is placed immediately post extraction (Fig.2,3). The patient wants to remove the tooth first and wait until his insurance gets approval for the implant coverage. No bone graft is placed in the extraction socket.
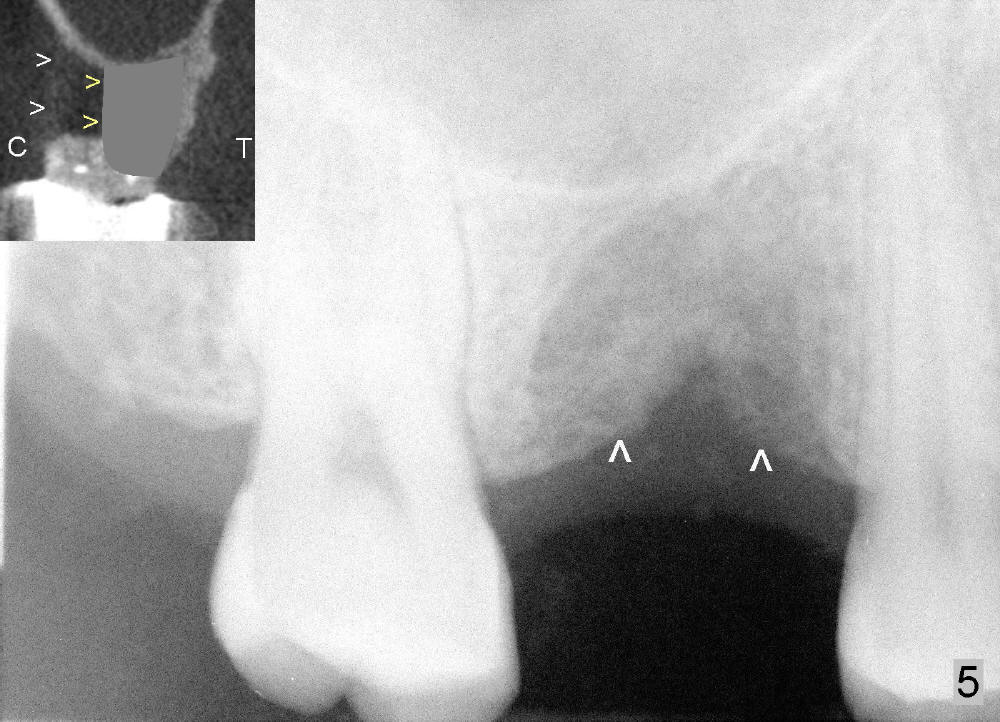
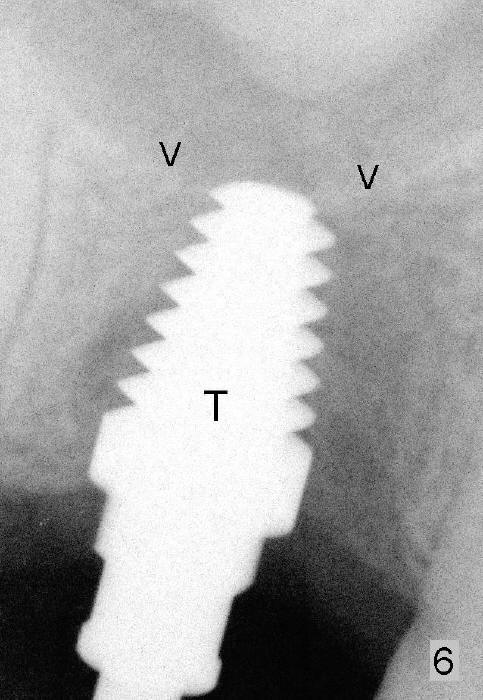
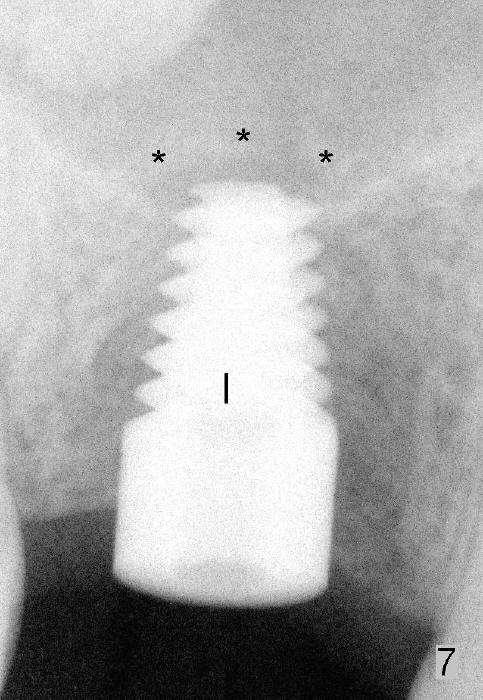
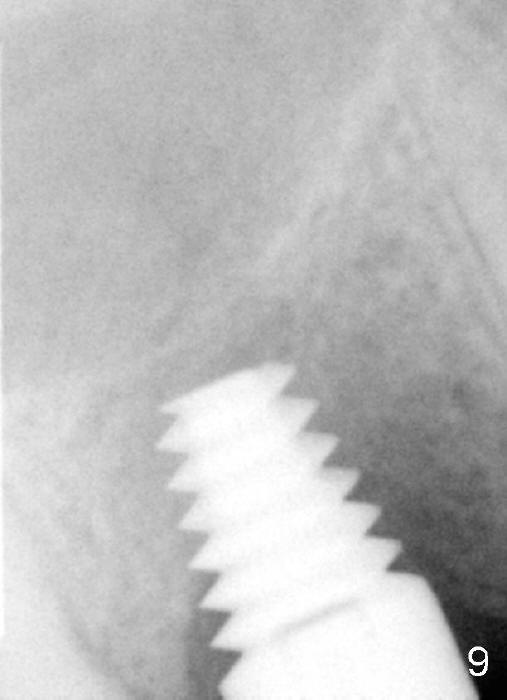
Six months and a half later, the socket appears to be empty (Fig.5) with apparently buccal plate collapse (as indicated by inset in Fig.5). The bony ridge is measured to be ~ 5 mm buccolingually using bone gauge. Osteotomy forms by bone expansion technique. In short, #15 blade is used to split the ridge (slightly lingual), followed by bone scalpels 4,5, and 6 mm, bone blades 4, 5.5 and 7.5 mm, and round tapered osteotomes 2, 3, 4 and 5 mm (Tatum Surgical). The depth is approximately 11 mm. When the last osteotome (4.5 mm round blunt) is used, it deviates too much lingually. A surgical curet is used to explore the osteotomy site. The bony wall appears to be intact except lingual. A 6x11 mm tapered tap is inserted with some resistance (Fig.6). In contrast it is difficult to engage 5.8 mm round tap into the osteotomy site. A 6x11 mm tapered implant is placed with insertion torque 40 Ncm (Fig.7). Amoxicillin is prescribed. The patient is doing fine postop, although the implant is not stable with mild tenderness. Six month post-implantation, the implant appears to have been descended (Fig.8,9, compare to Fig.7).
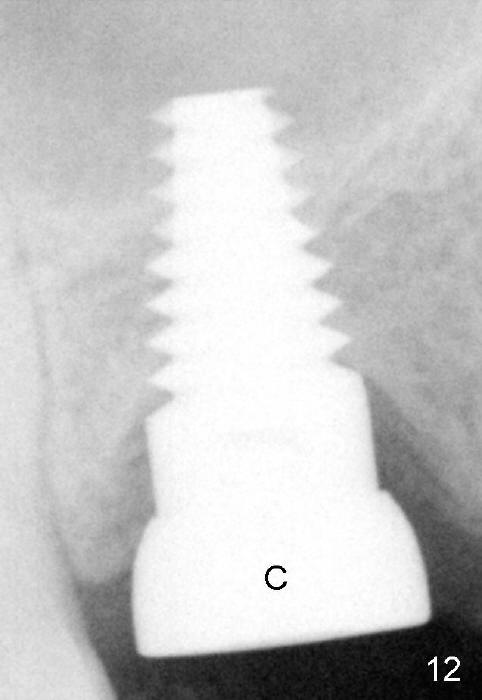
Following local anesthesia, the failing implant is removed without resistance. The sinus floor is present. The lateral walls are intact, although probably short. A series of rounded tapered osteotomes (2-5 mm in diameter) are used for sinus lift at the depth of 14 mm. A 4.5x14 mm tap is inserted (Fig.10). One more carpule of Lidocaine is administered. A 6x14 mm implant is placed with torque more than 60 Ncm without additional bone graft (Fig.11). A 6-month postop PA confirms osteointegration (Fig.12). An abutment is placed (Fig.13) for a definitive crown (Fig.14). PA taken 6 months post cementation shows that bone density mesial to the implant increases (Fig.15 <).
This case suggests the importance of immediate implant for the first and second times of surgery. The maxillary implant should be engaged into the sinus floor for primary stability.
The low insertion torque (40 Ncm) is associated with failure of osteointegration (1st placement), whereas the high one (>60 Ncm) is related to osteointegration (2nd placement of longer implant). What should be done when a 7x17 mm implant fails
Return to When Implant Fails, Immediate Implant Complications
Xin Wei, DDS, PhD, MS 1st edition 04/20/2014, last revision 12/20/2015