|
|
|
|
|
|
|
|
|
Immediate Implants in Type II Extraction Sockets
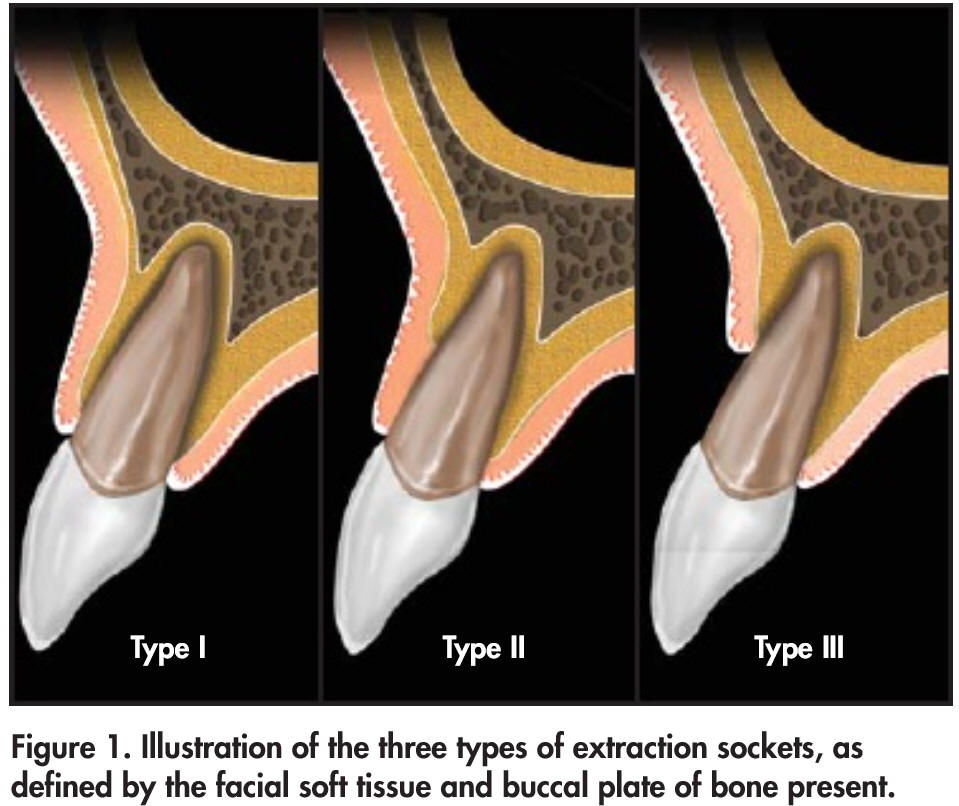
Extraction sockets are classified into three types (Eian et al, 2007).
In Type I Socket, the facial soft tissue and buccal plate of bone are at normal levels in relation to the cementoenamel junction of the pre-extracted tooth and remain intact post-extraction (Fig.1).
In Type II Socket, the facial soft tissue is present but the buccal plate is partially missing following extraction of the tooth.
In Type III Socket, the fial soft tissue and the buccal plate of bone are both markedly reduced after tooth extraction.
It appears that immediate implant indicated in Type II socket, whereas the hard tissue and the soft and hard tissues need to be regenerated for Type II and III sockets, respectively, prior to implant placement.
In this article, we are going to discuss that the extraction socket classification seems to be oversimplified and that immediate implants can be safely placed in Type II Sockets from the central incisor to the 2nd molar.
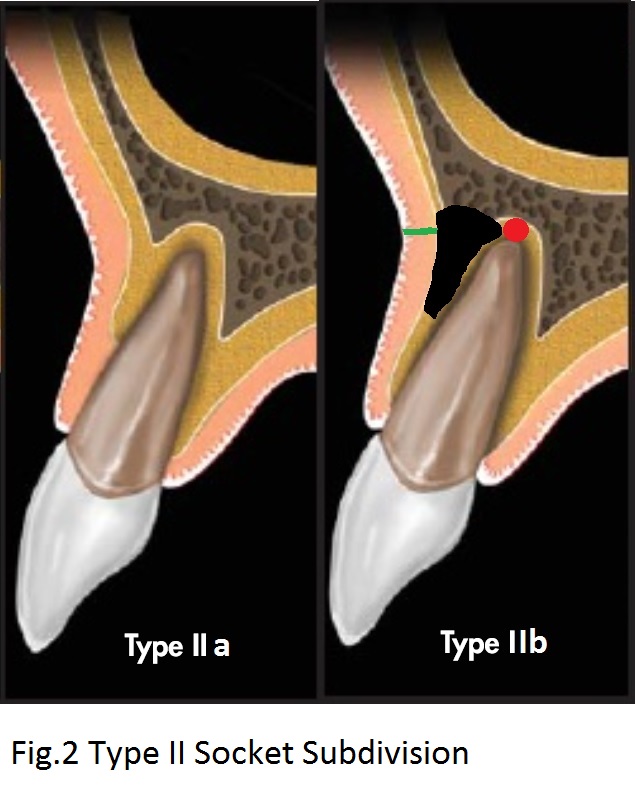
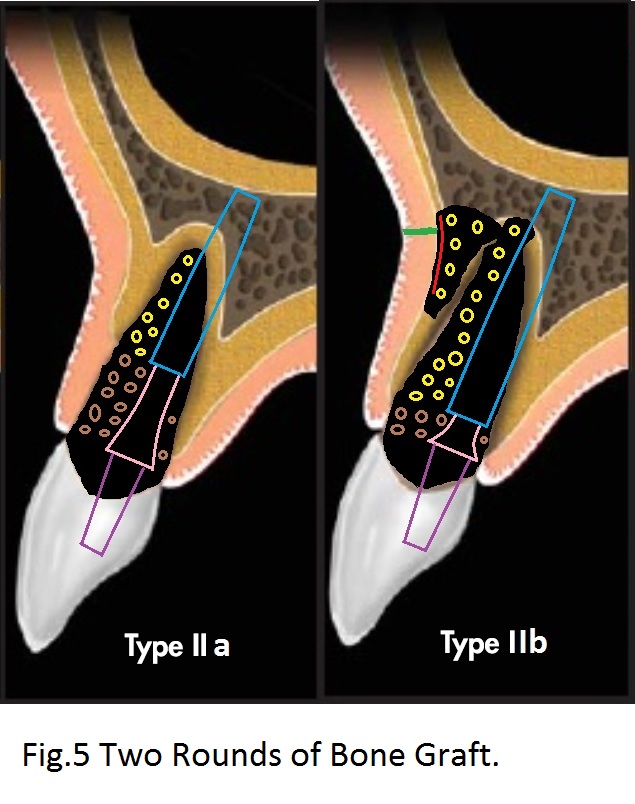
The typical Type II Socket (with loss of the coronal portion of the buccal plate) proposed by Elian et al is often observed in periodontitis patients (Type IIa, Fig.2), whereas the apical portion of the buccal plate is resorbed (Type IIb black area) in association with endodontic lesion (red circle) with or without apical fistula (green).
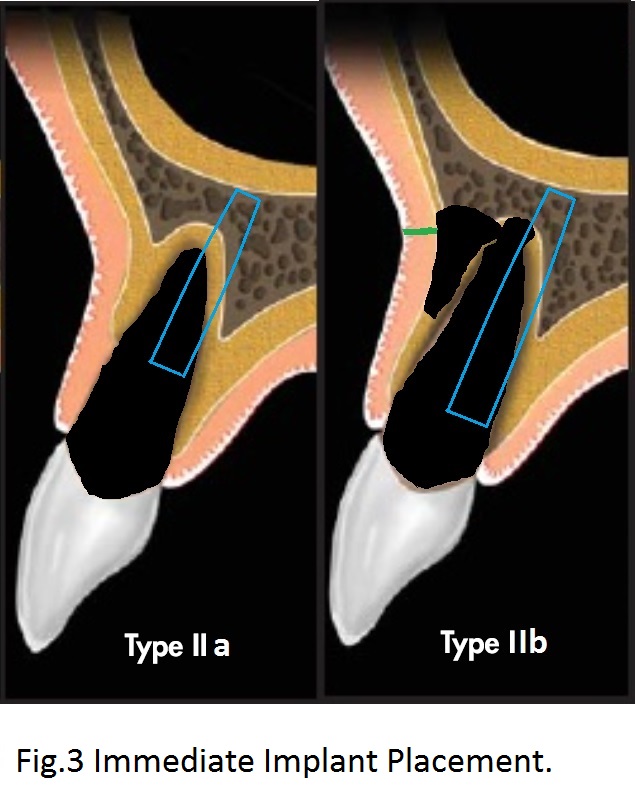
To reduce periimplantitis, the immediate implant (Fig.3 blue) should be placed placed as low as possible (subcrestal). If the coronal loss of bone of Type IIa is severe, the implant could be slightly supracrestal.
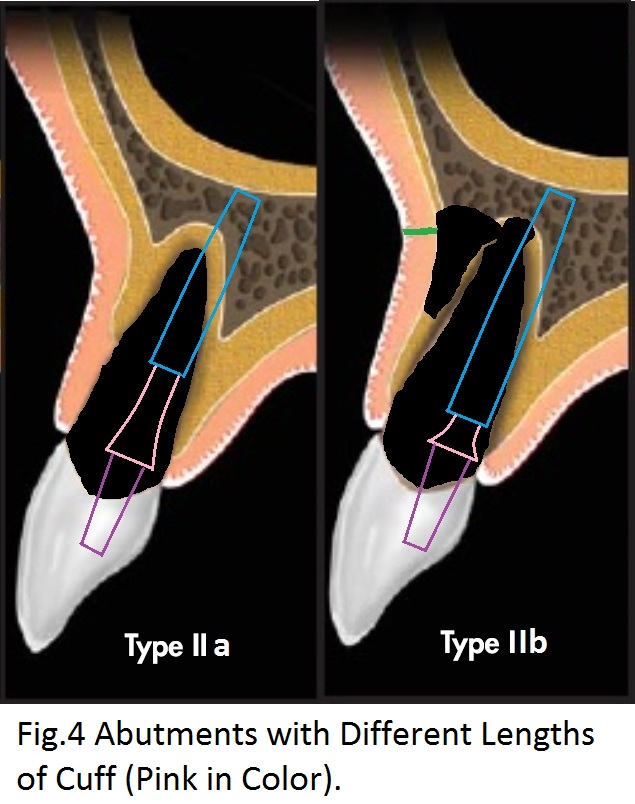
To compensate for deep placement of the immediate placement, an abutment (Fig.4 purple) with long cuff (pink) is placed for Type IIa socket.
Next bone graft is placed around the implant and abutment after their placement in 2 rounds (Fig.5). It appears that the implant and abutment are excellent framework, functioning similar to Titanium mesh for guided bone regeneration.
Return to
Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/14/2017, last revision 12/06/2020