
,%204.5x7.5(4).jpg)

|
|
|
|
|
|
|
|
|
|
|
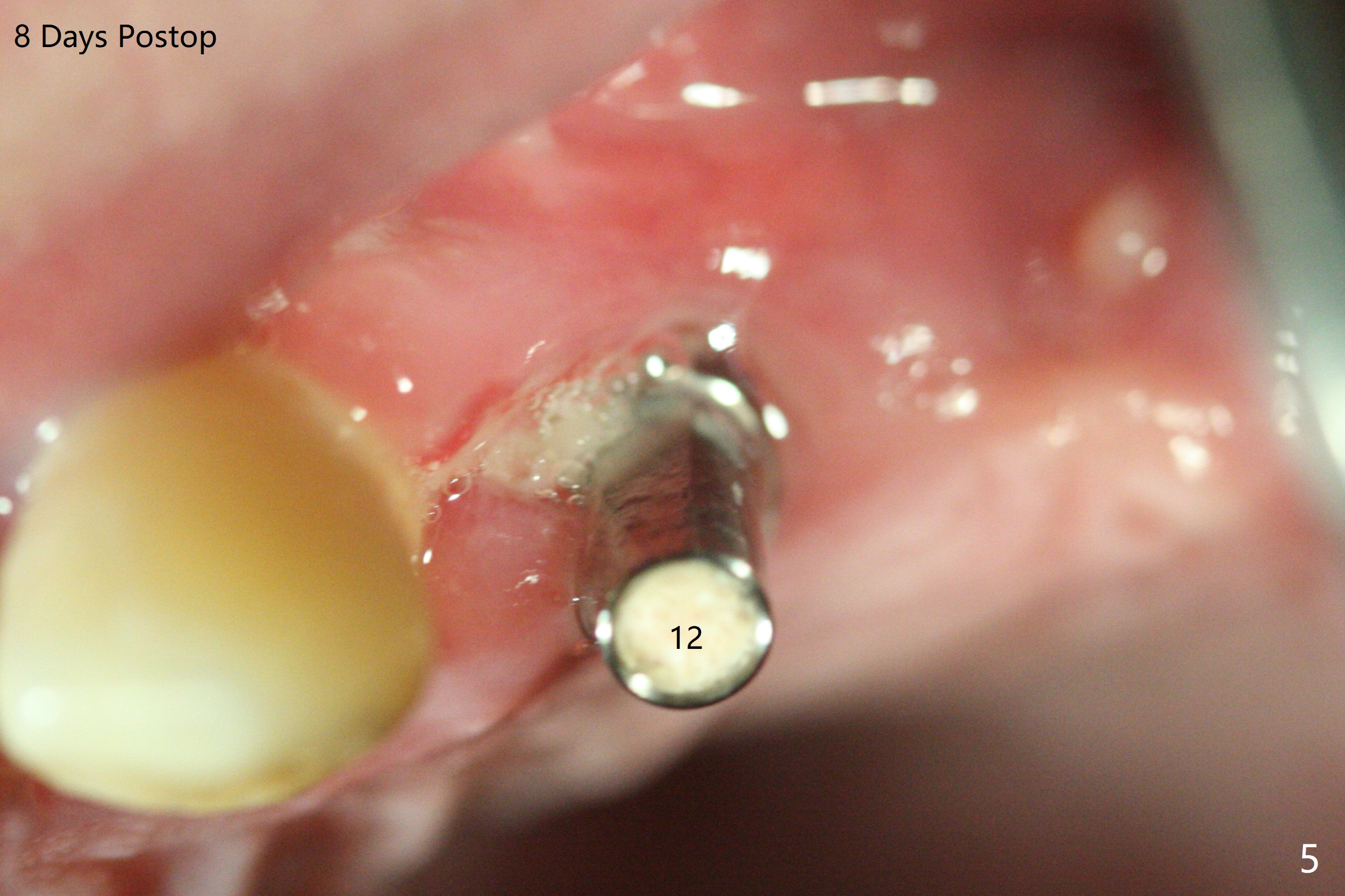
Acrylic Dressing M
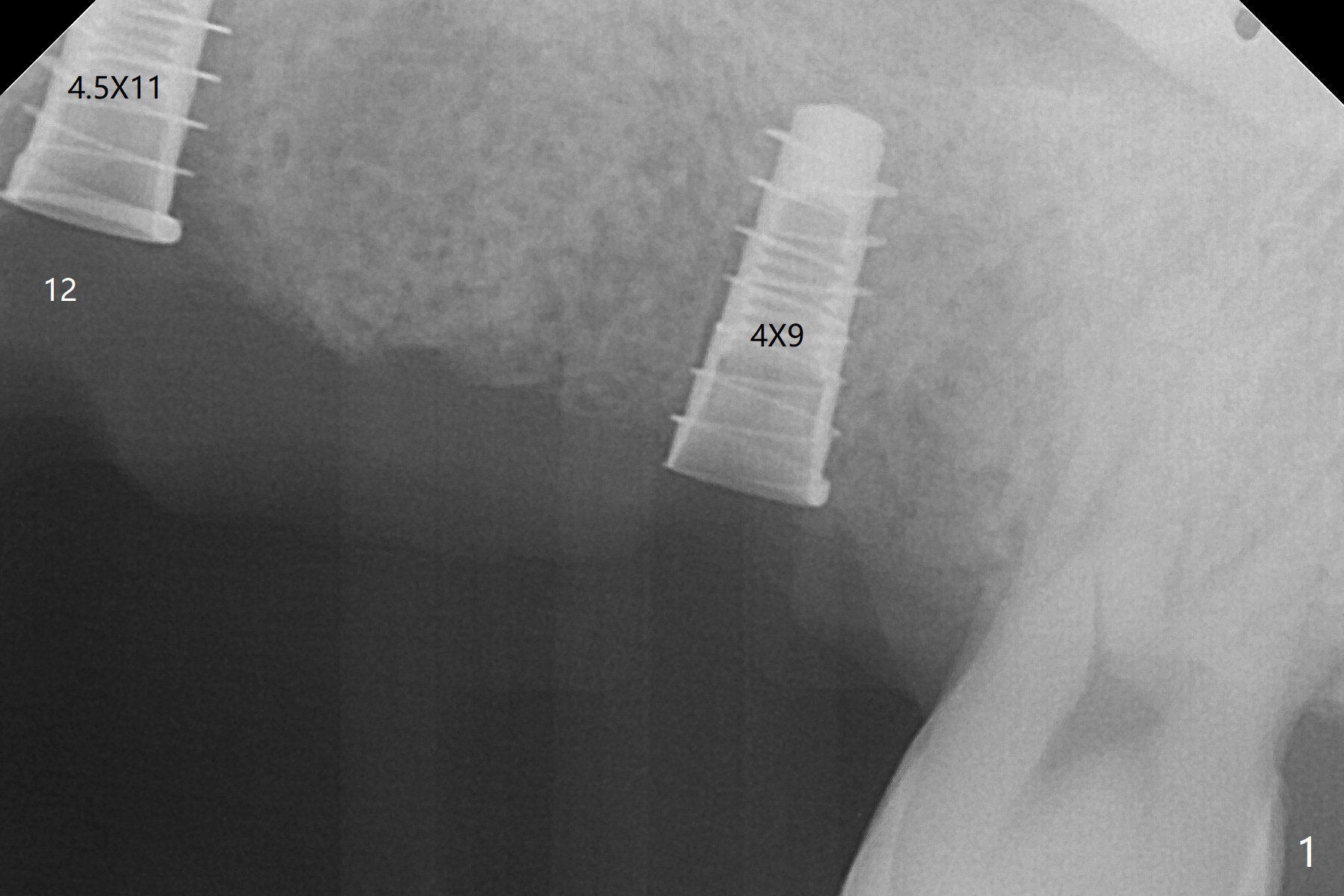
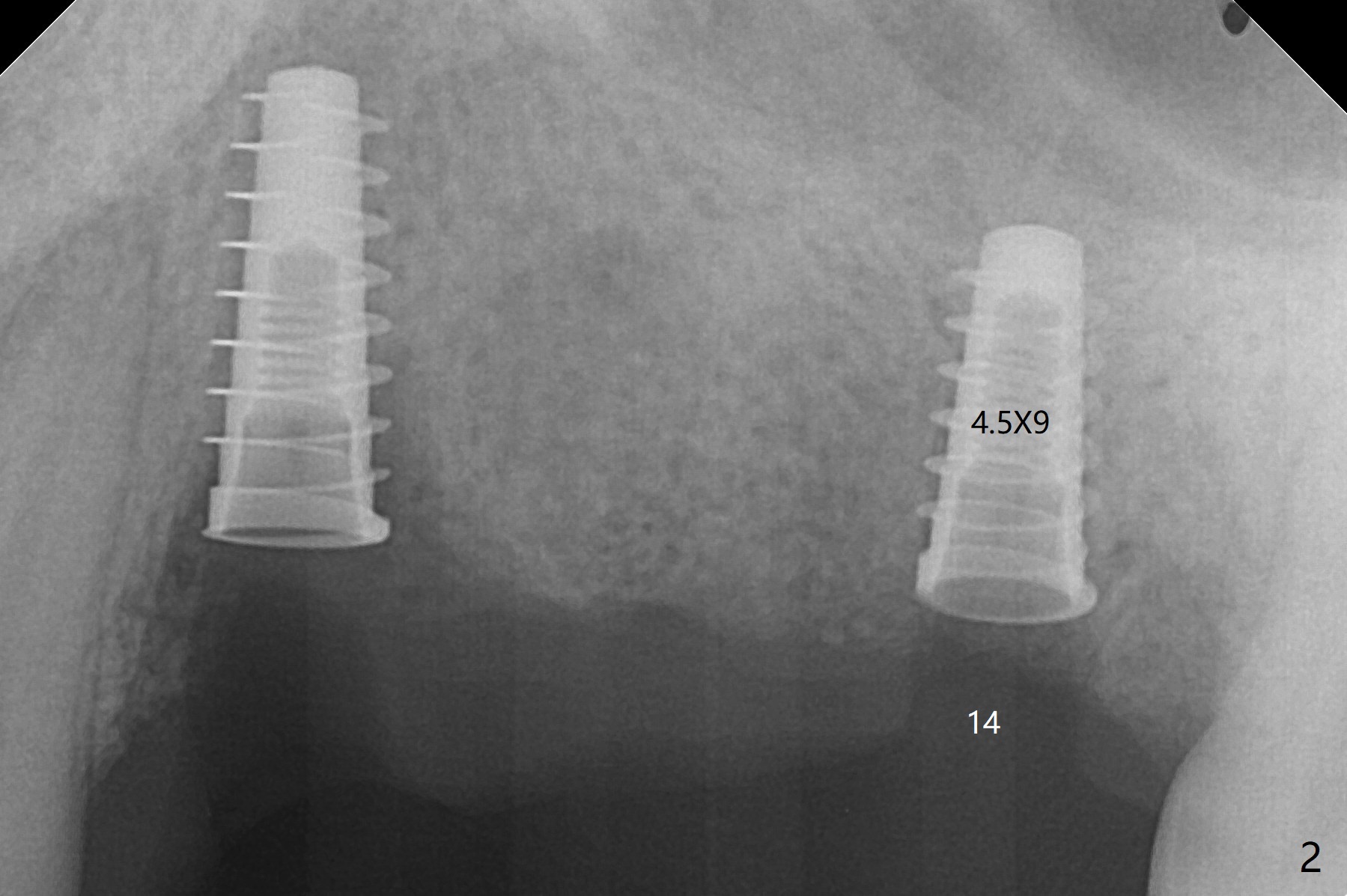
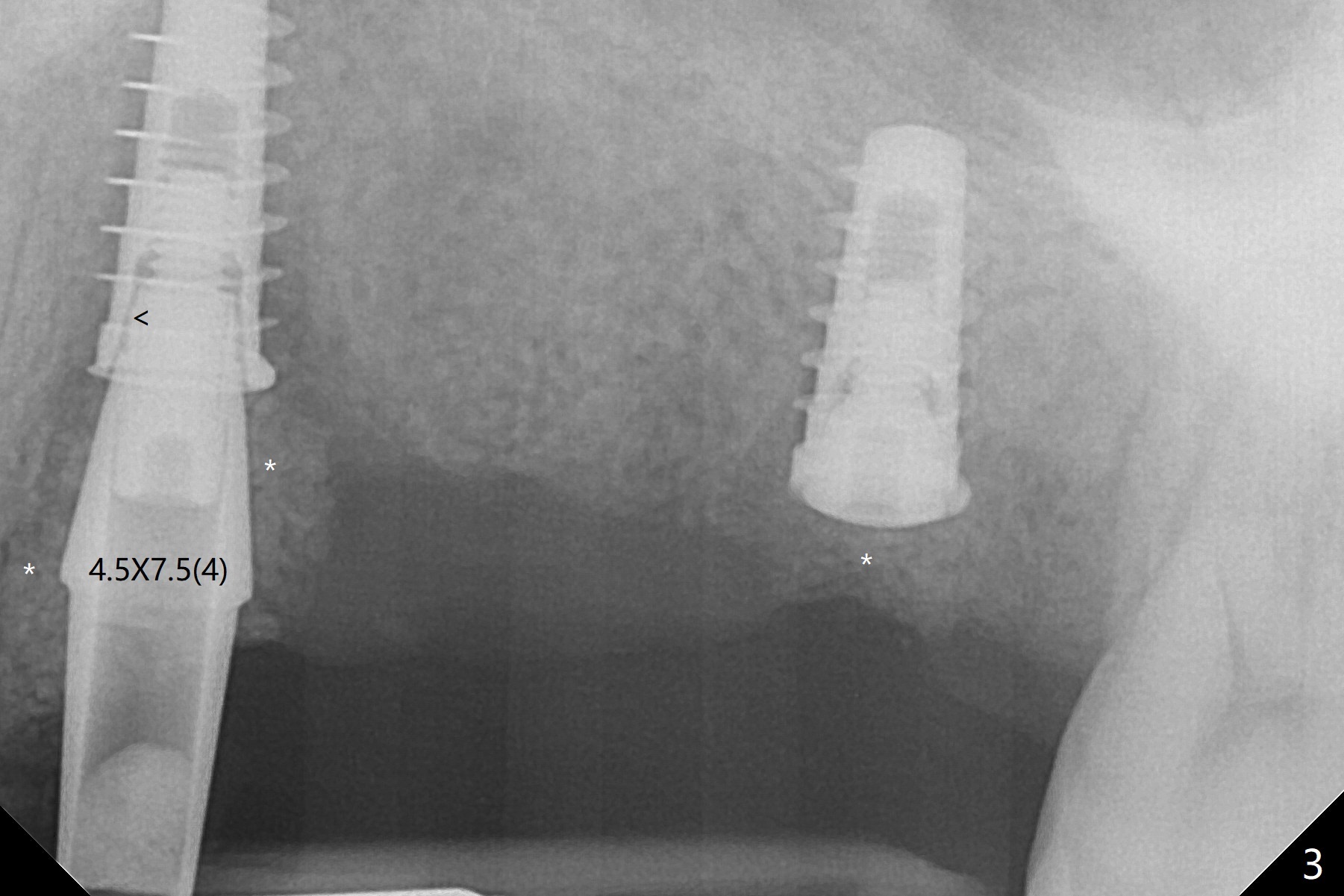
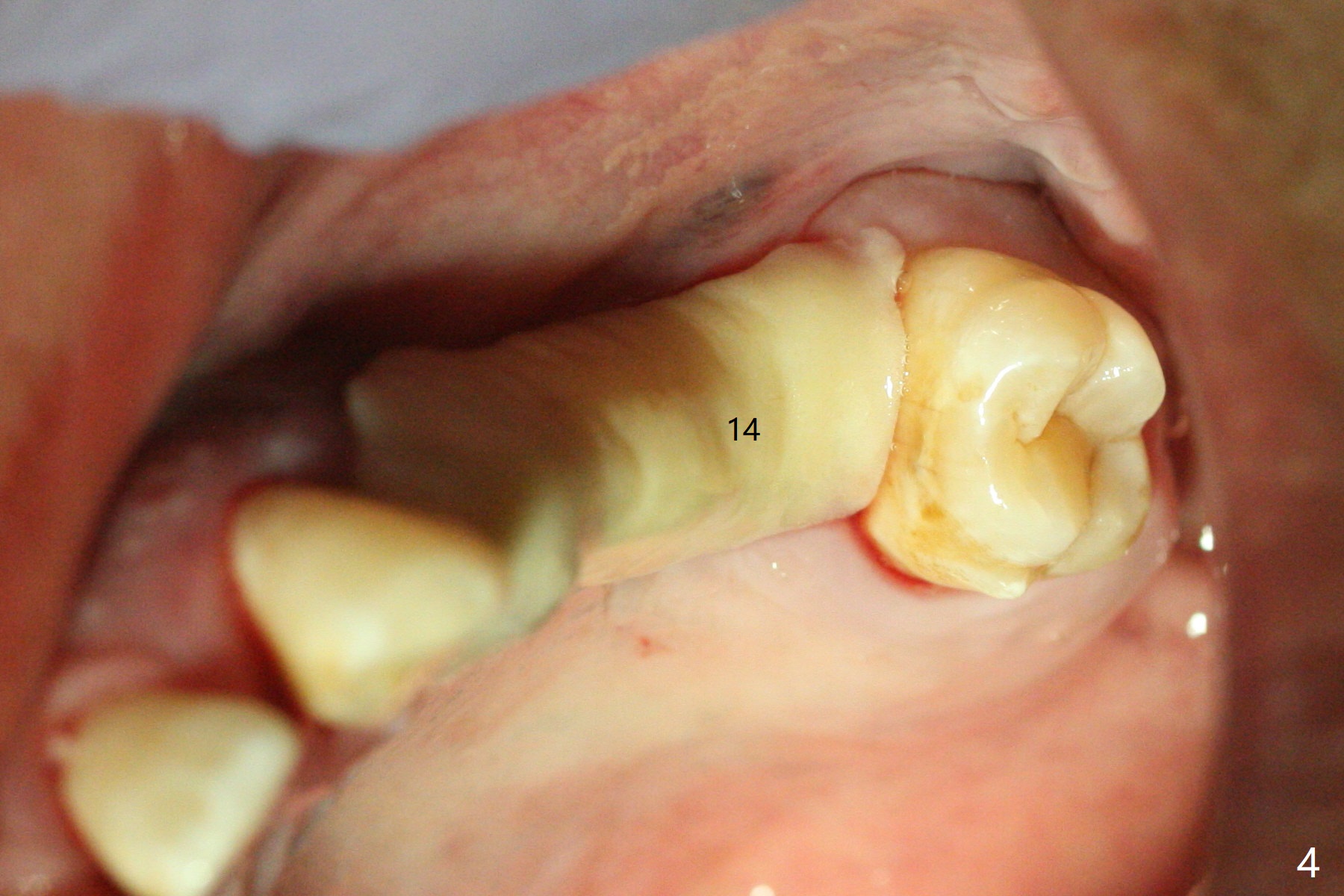
Immediate placement at #12 is smooth with 20 Ncm, whereas delayed one at #14 involves sinus membrane perforation; after insertion of PRF and mixture of autogenous bone and allograft, a shorter dummy implant tries in with stability (Fig.1). The final implant at #14 has ~60 Ncm, but the coronal palatal bone may be insuficient (Fig.2). Sticky bone is placed to bury the implant at #14 (Fig.3 *). After placement (incomplete, Fig.3 <) of a 4.5x7.5(4) mm pair abutment, setting acrylic is applied around the abutment, over the bone graft at #14 (to prevent loss) and pressed into the undercuts of the proximal surfaces of the neighboring teeth for retention (Fig.4). The sockets at #12 heals 8 days postop when a 2nd acrylic dressing dislodges (Fig.5). It appears that the retention of 3-unit acrylic dressing is poor. The wound at #14 also heals, but it would be better to make an incision to save the soft tissue (Fig.6). The bone/implant gap reduces at #13 five months postop (Fig.7 (complete abutment seating)). There is no implant thread exposure at #13 (immediate), while minor exposure mesial to #15 (delayed). The patient complains of food impaction between #13 and 14 buccally 6 months post cementation (Fig.8). Return to Upper Molar Immediate Implant, No Deviation 19 Next Case Xin Wei, DDS, PhD, MS 1st edition 01/21/2020, last revision 02/03/2021