

,%20Vanilla,%20trimmed%20abutment,%2026.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
2 mm 1-Piece
Implant
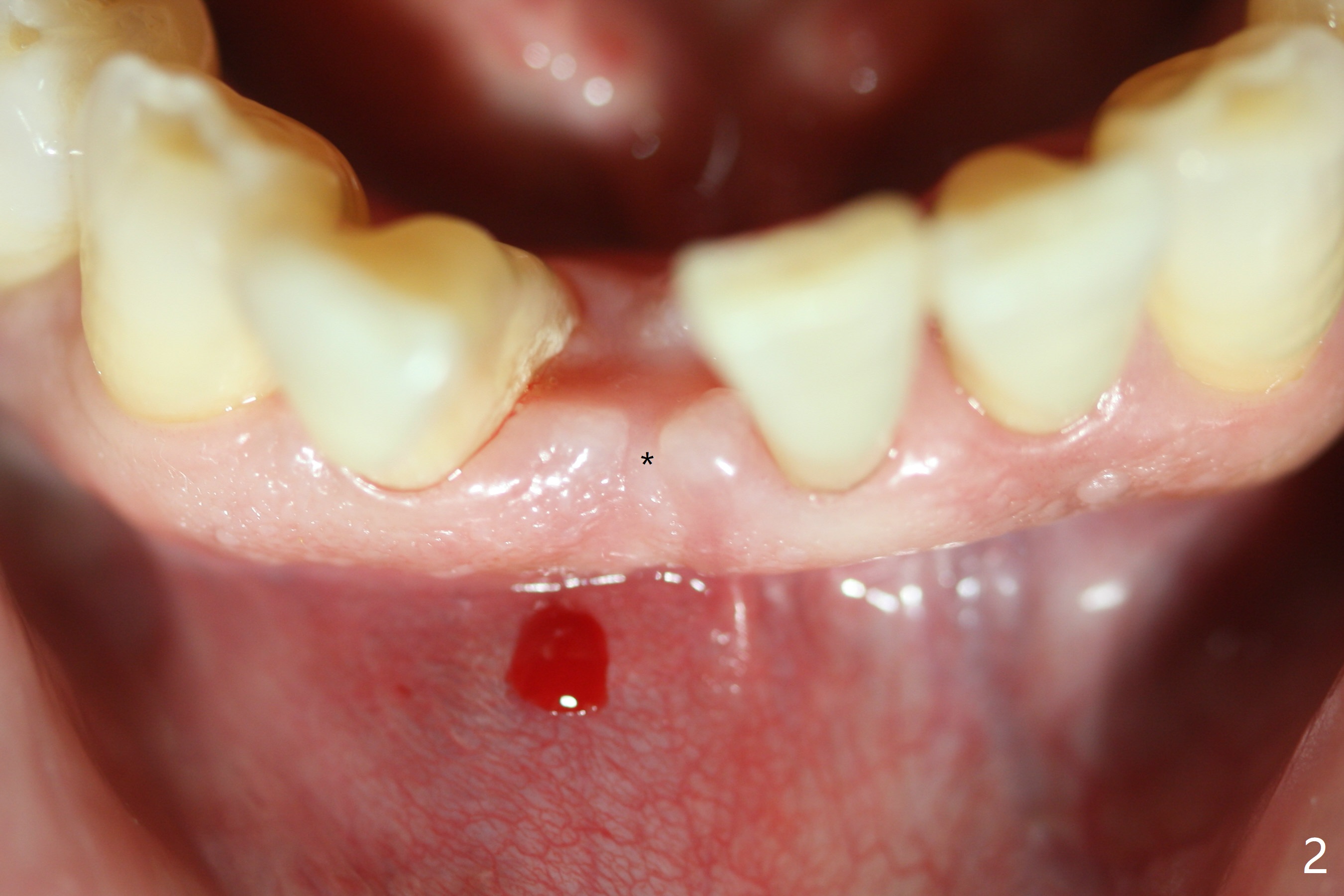
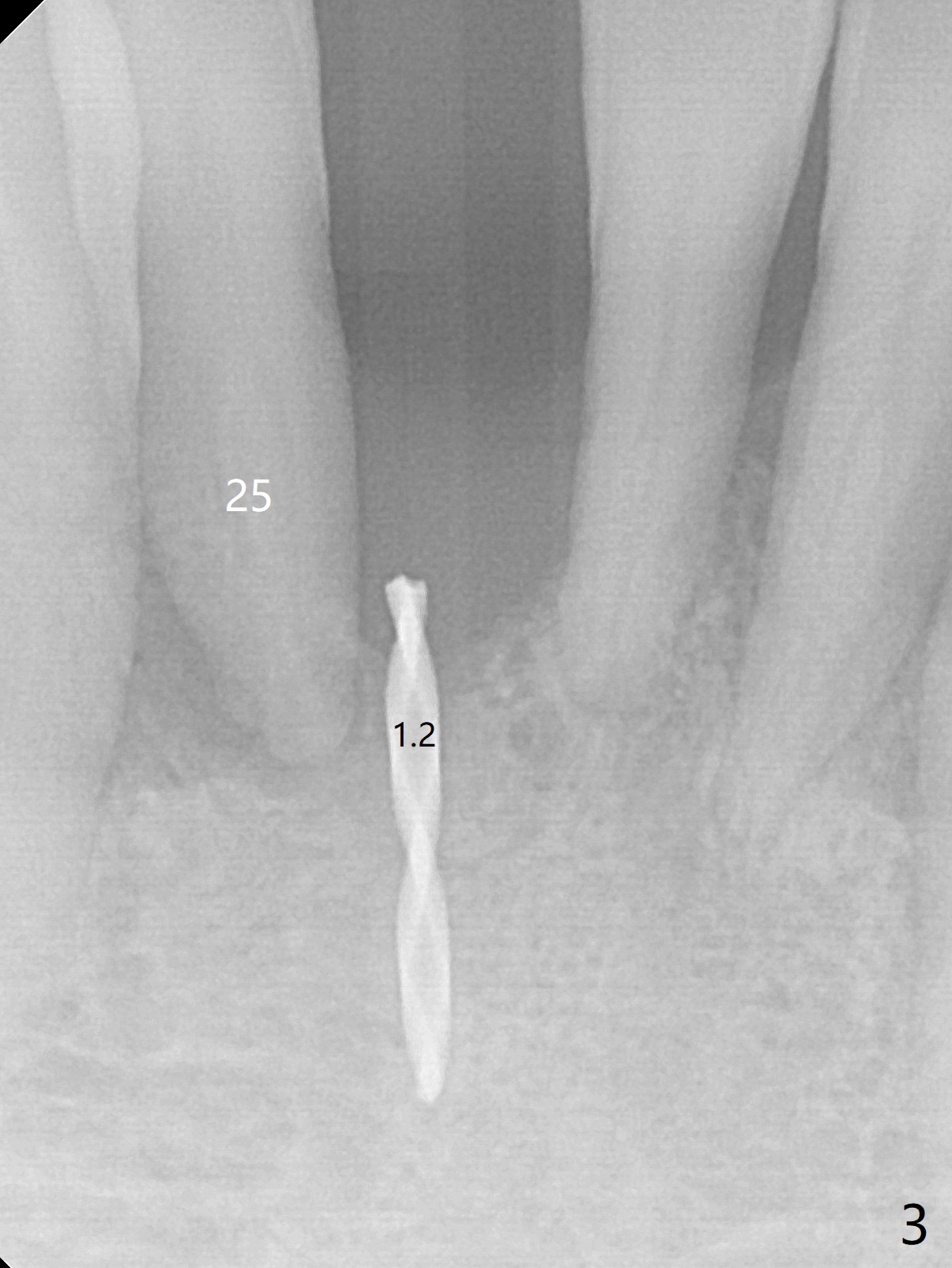
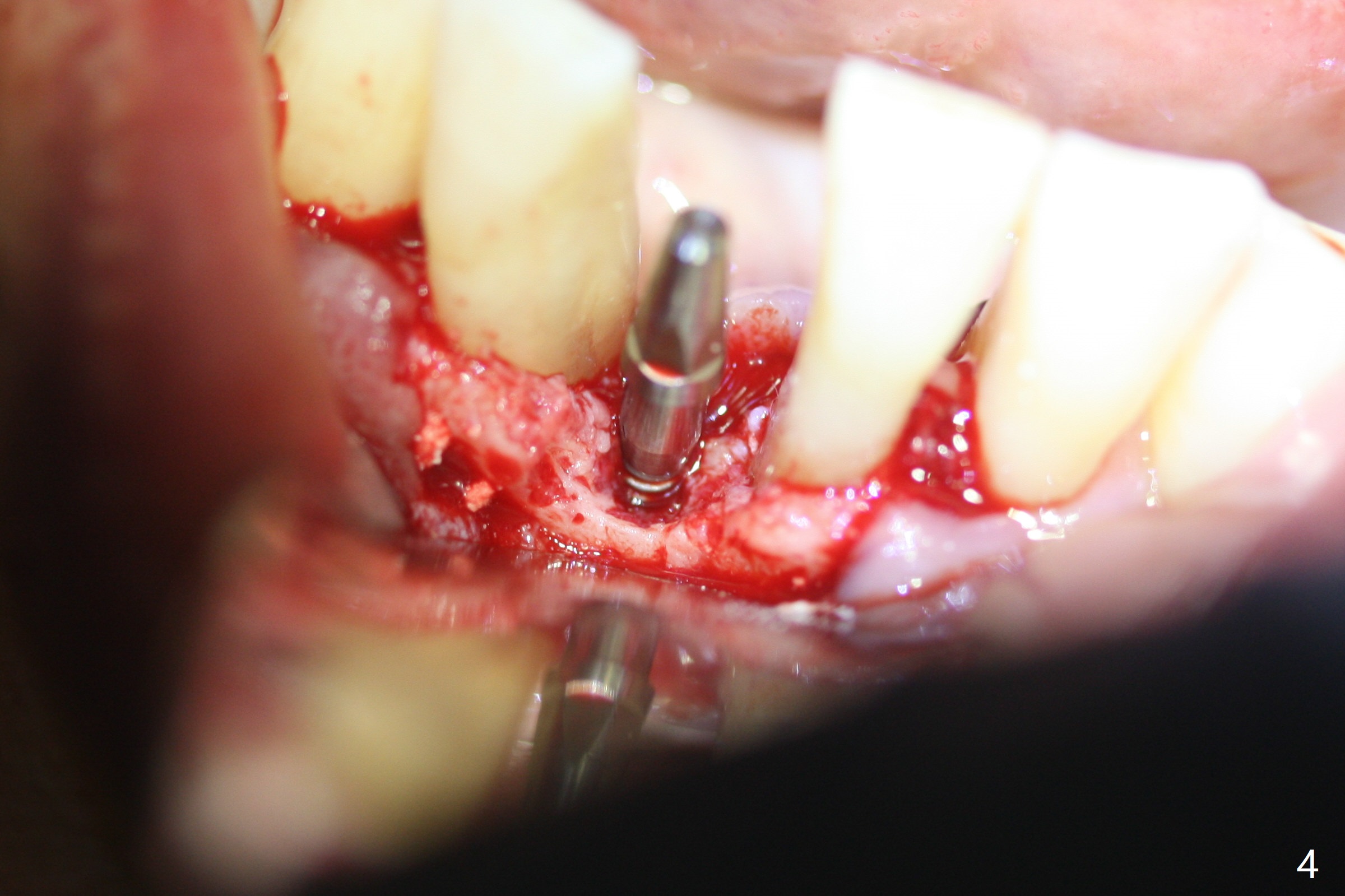
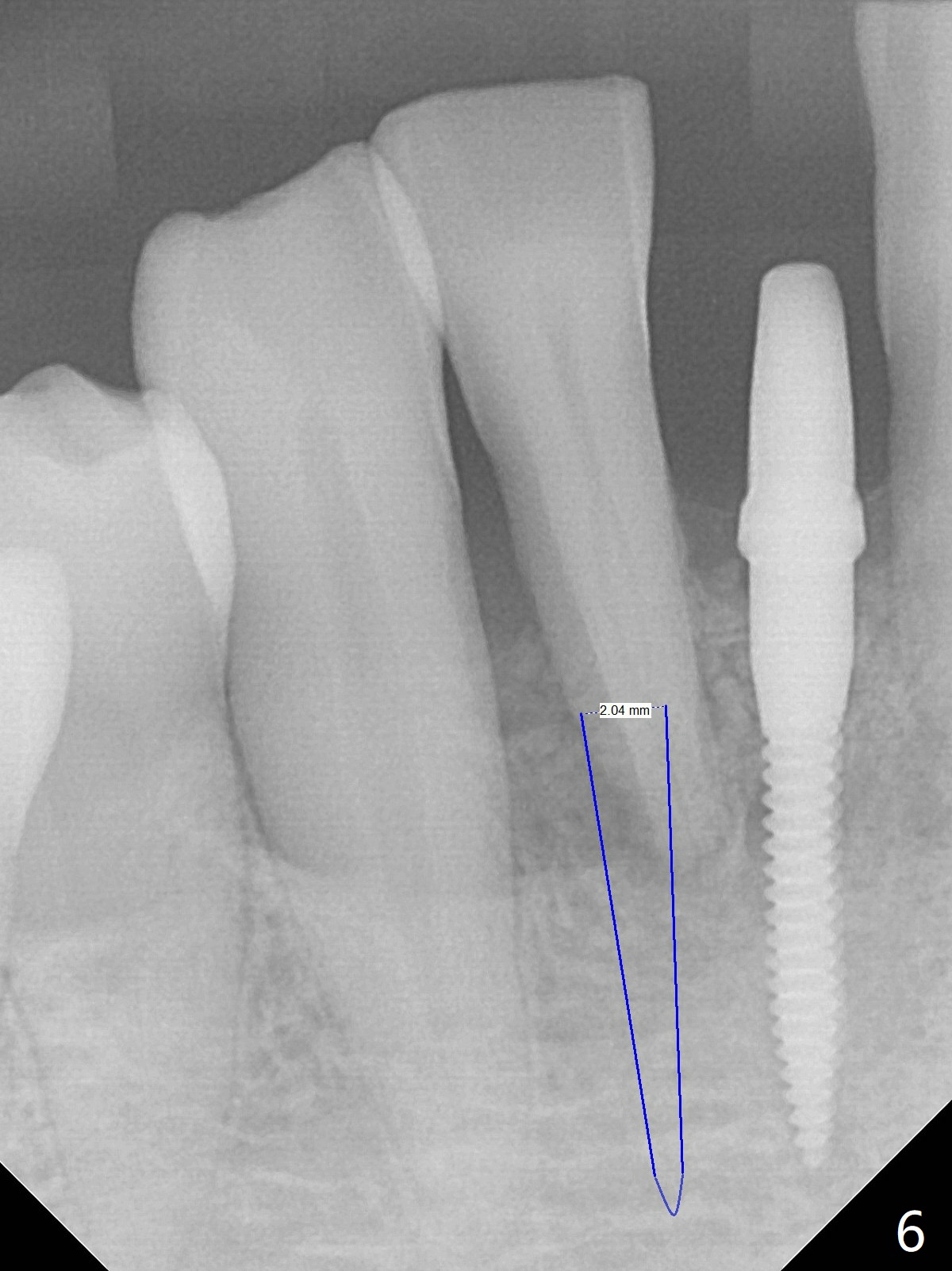
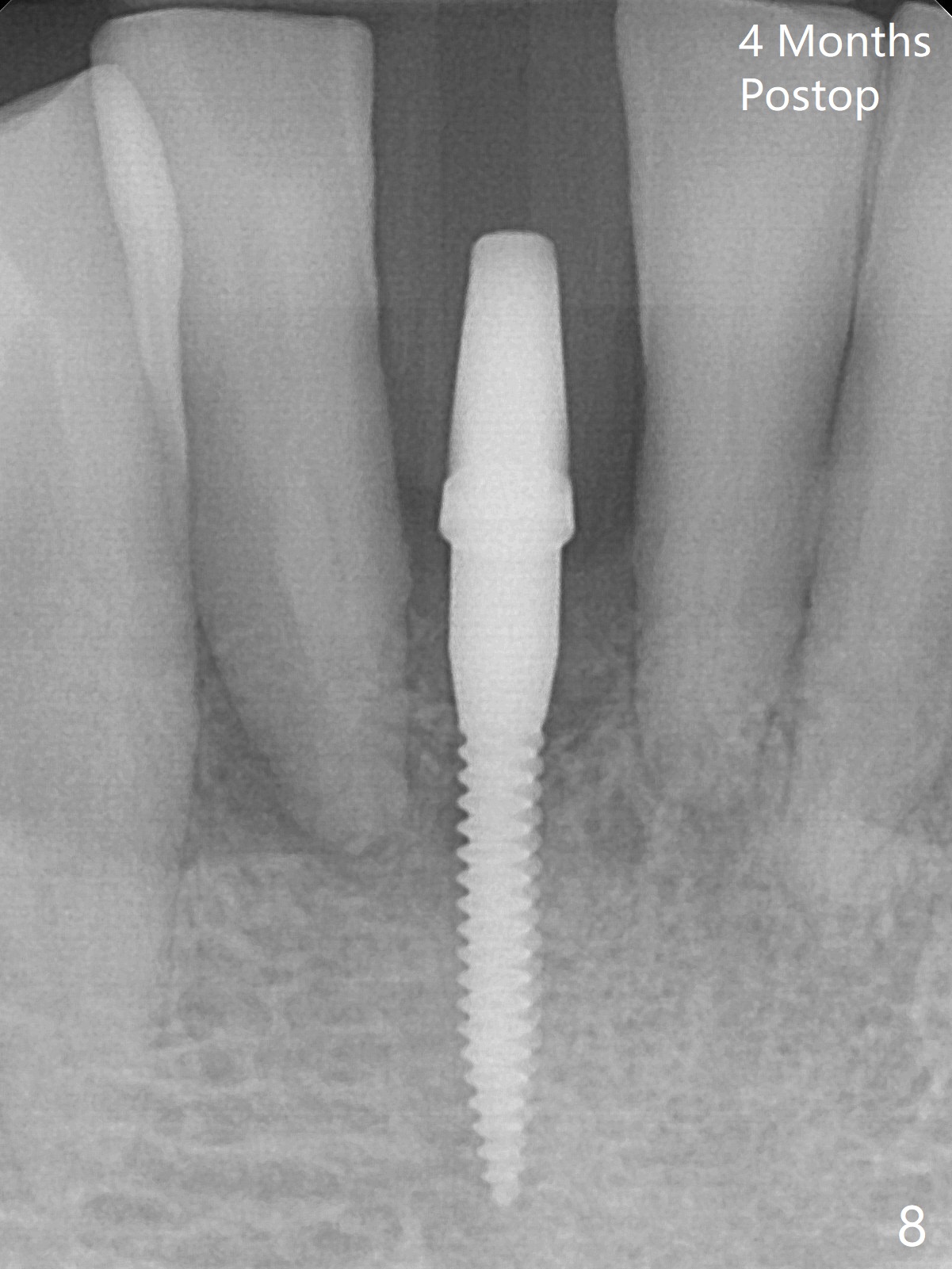
Out of financial concern, the patient does not agree to have the tooth #26 extracted. Due to atrophy of the most coronal ridge buccally at #25 (Fig.1,2 *), osteotomy is initiated difficult and distal (Fig.3). After 1.2 mm drill removal (Fig.3' black area), Lindamann bur is used to move the osteotomy mesial (red area). A 2x12(4) mm 1-piece implant is placed (Fig.4,5); the buccal defect is packed with allograft (Vanilla, .5-1 mm cancellous/cortical mixture, *). When the tooth #26 fails, a 2 mm implant will be placed (Fig.6 blue). Following abutment adjustment, a provisional is fabricated (Fig.7 P); note the lower incisal edges of #25 and 26, as compared to those of the neighboring teeth. To reduce occlusal trauma, the incisal edge of the tooth #26 has been decreased (Fig.5 open arrow). The implant threads seem not to be exposed 4 months postop (Fig.8), although the tooth #26 has mobility II.
Return to
Lower Incisor Immediate Implant,
Trajectory Weichat
Xin Wei, DDS, PhD, MS 1st edition
01/28/2019, last revision
05/30/2019