



|
|
|
|
|
|
|
|
|
|
|
|
||
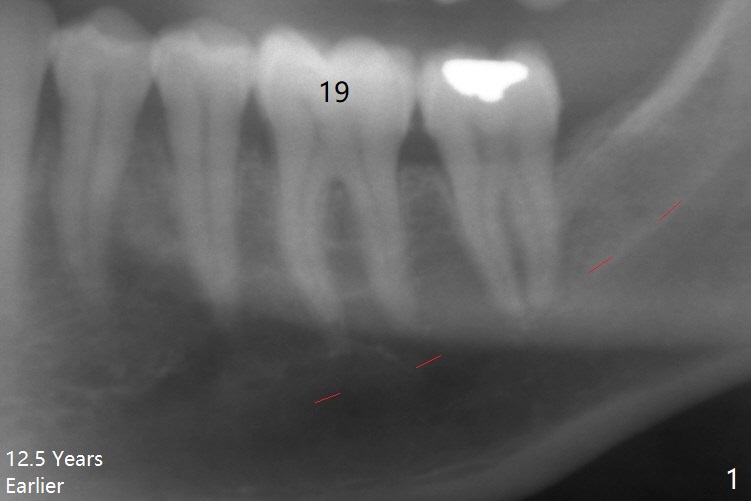
Why Not Immediate Implant?
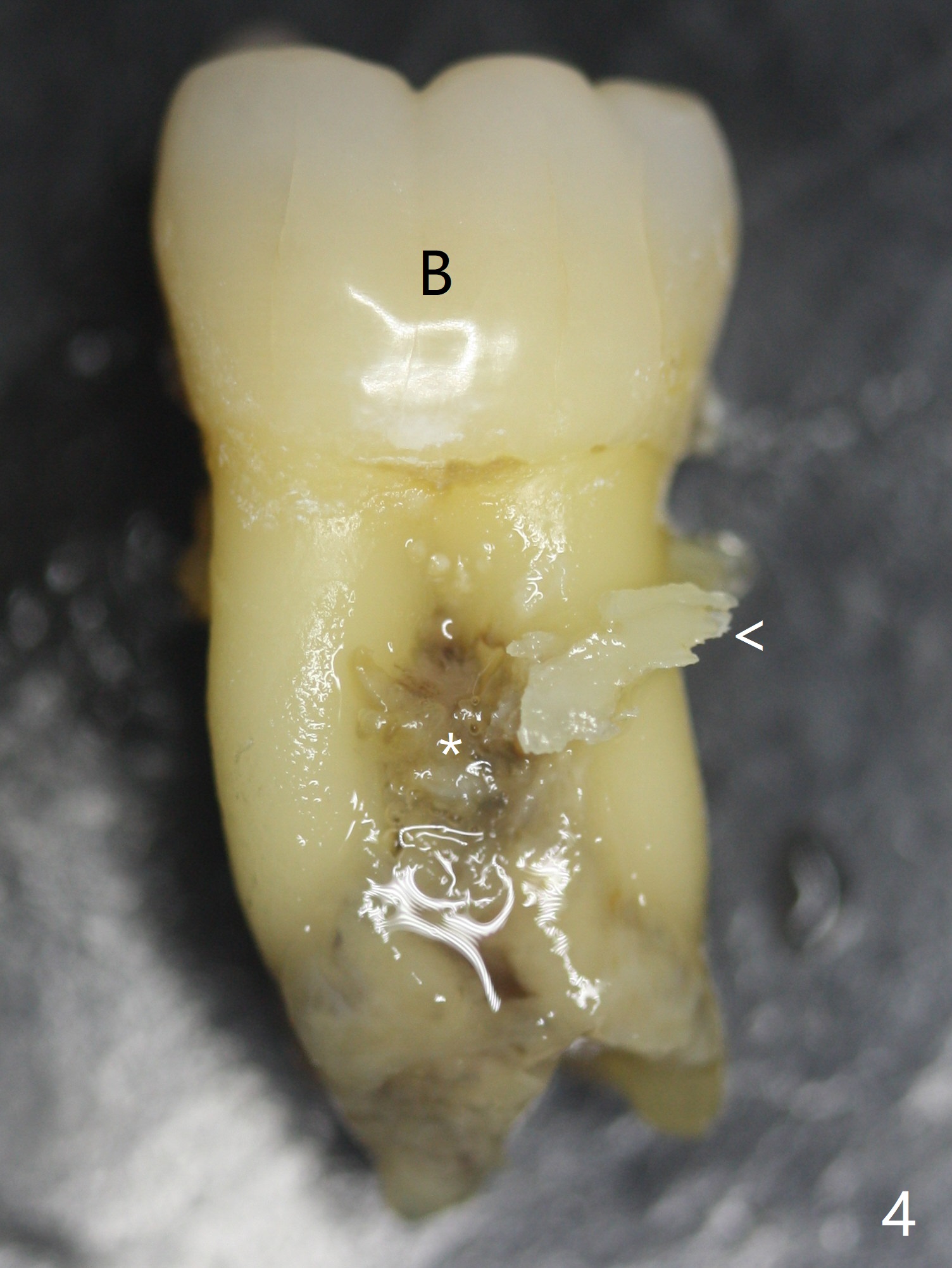
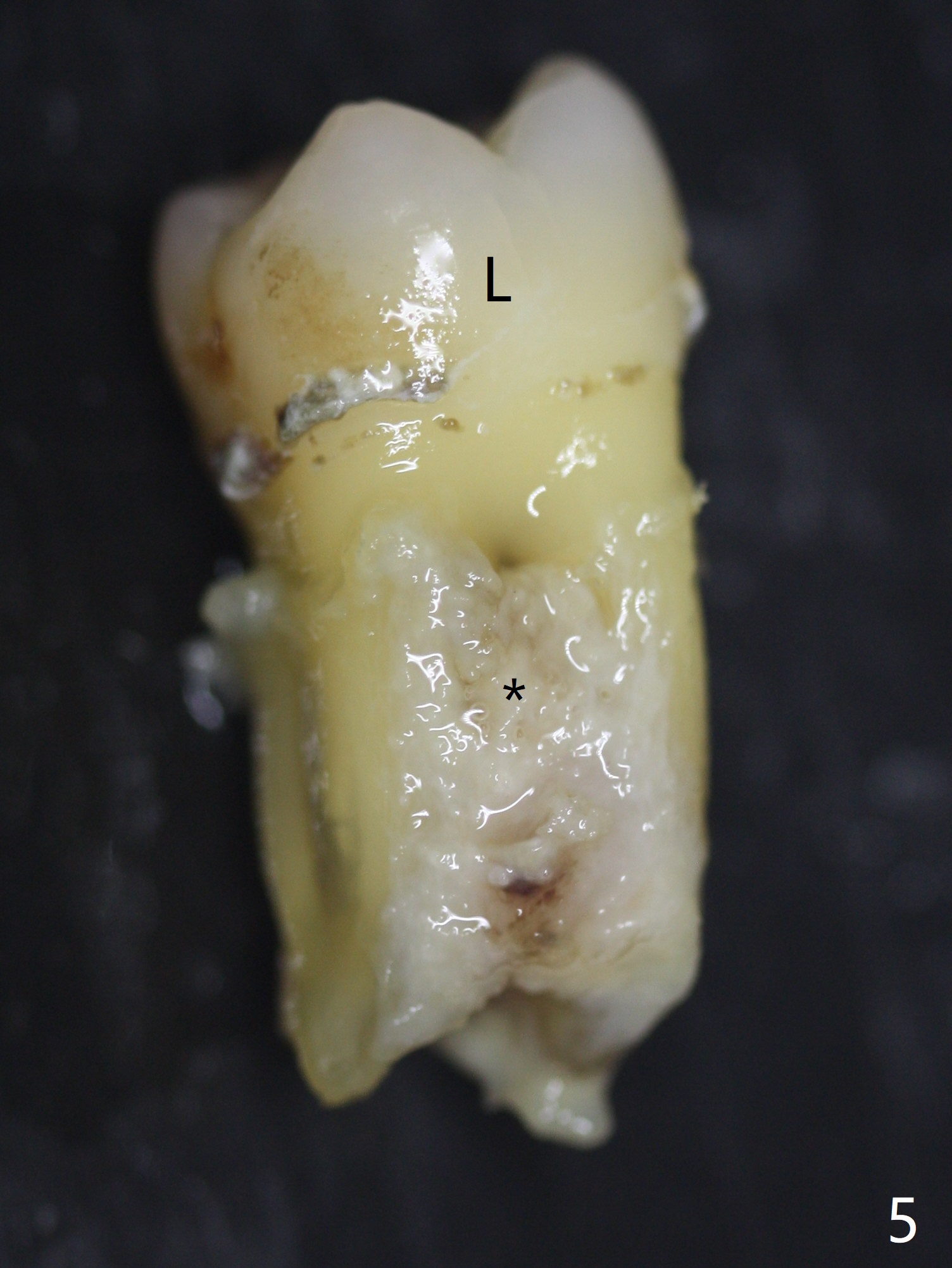
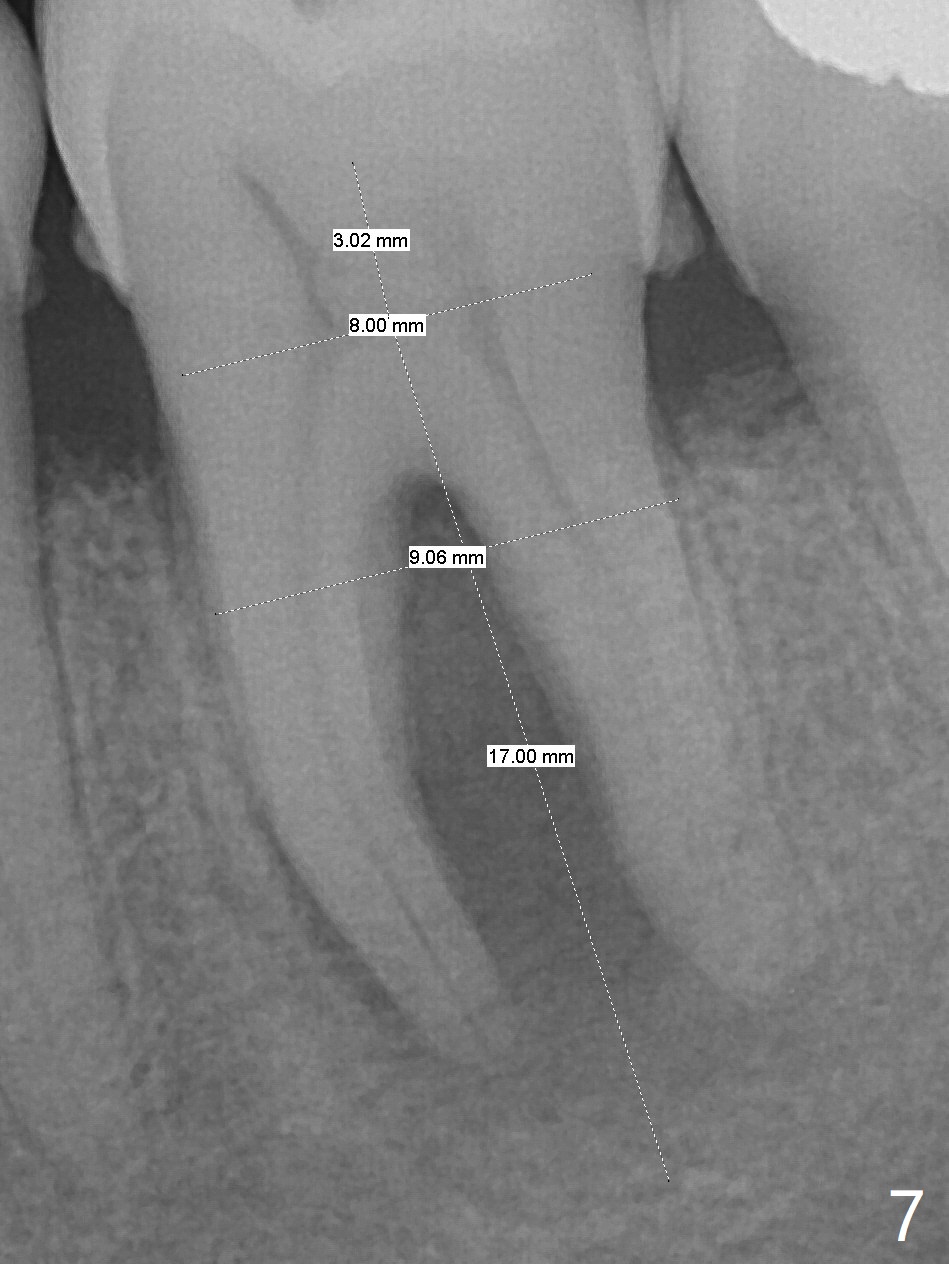
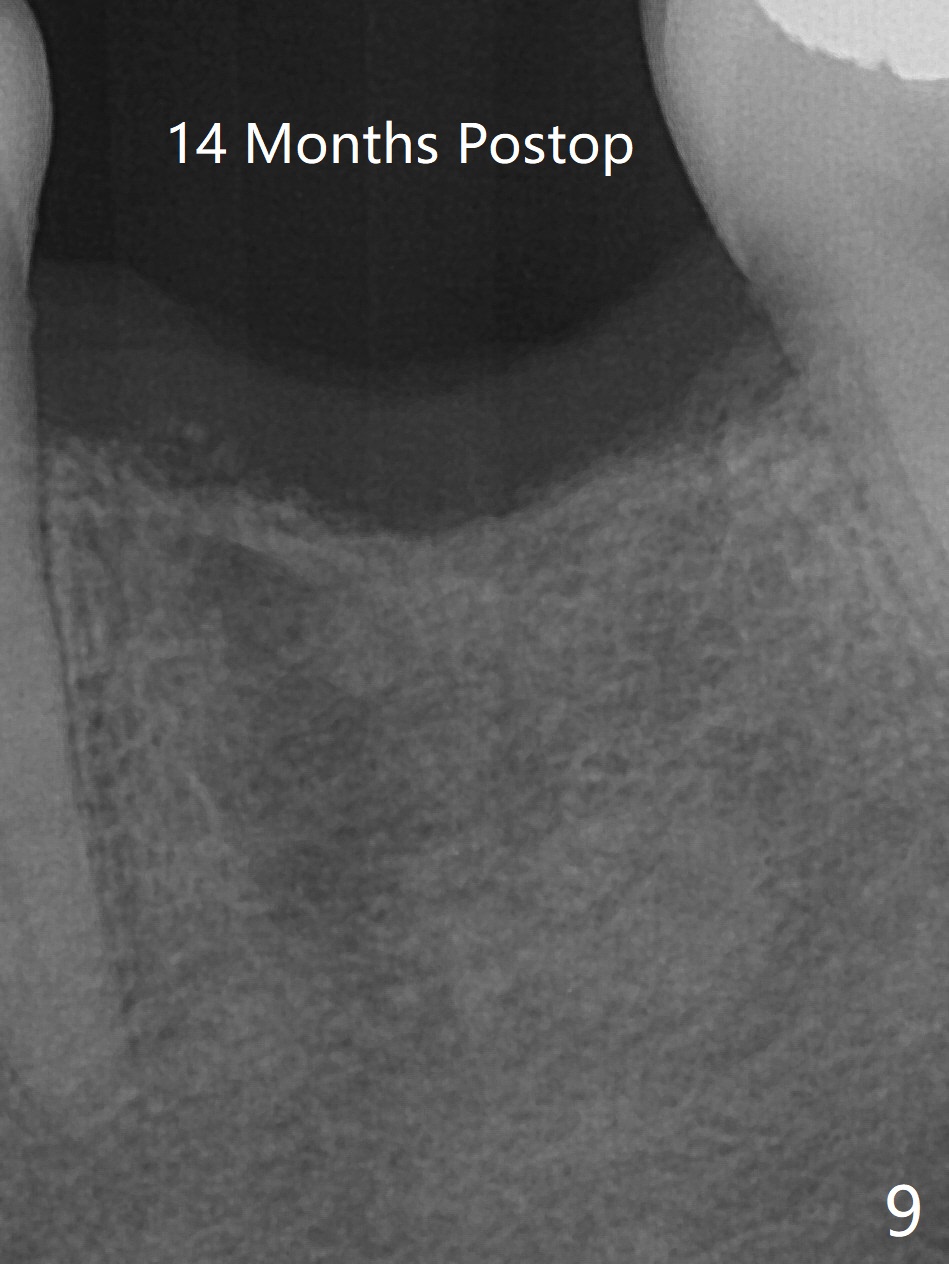
A 62-year-old man (smoker, 1.5 packs a day) has had no dental visit for 12.5 years (Fig.1). His chief complaint is pain at #19 after eating popcorn. The septal bone resorbes (Fig.2,3 *) with granulation tissue between the mesial and distal roots (Fig.4,5 *). Although there is no bony wall defect, the socket is single and large (9x9 mm, Fig.7). The largest (8 mm) cylindrical implant should not be able to obtain primary stability. The biggest challenge for immediate implant is ambiguous the Inferior Alveolar Canal (Fig.1,3 red dashed line). If there were no financial or time issue for immediate implant, CBCT should have been taken. Socket preservation is done instead with Vanilla graft, Human Amniotic Chorion Allograft (membrane) and Osteogen Plug (Fig.6). If he returns for SRP and implant, perform flapless bone expansion for osteotomy. When the patient returns 14 d postop, #19 socket is healing and filled with bone graft (Fig.8 (panoramic X-ray)). When he returns 14 months postop, the socket heals (Fig.9, as compared to Fig.6).
Return to Lower Molar Immediate Implant, Armaments, Systemic Diseases SP Xin Wei, DDS, PhD, MS 1st edition 05/11/2018, last revision 09/12/2020