
|
|
|
|
|
|
|
|
|
|
|
Acrylic Dressing Replace-ment I
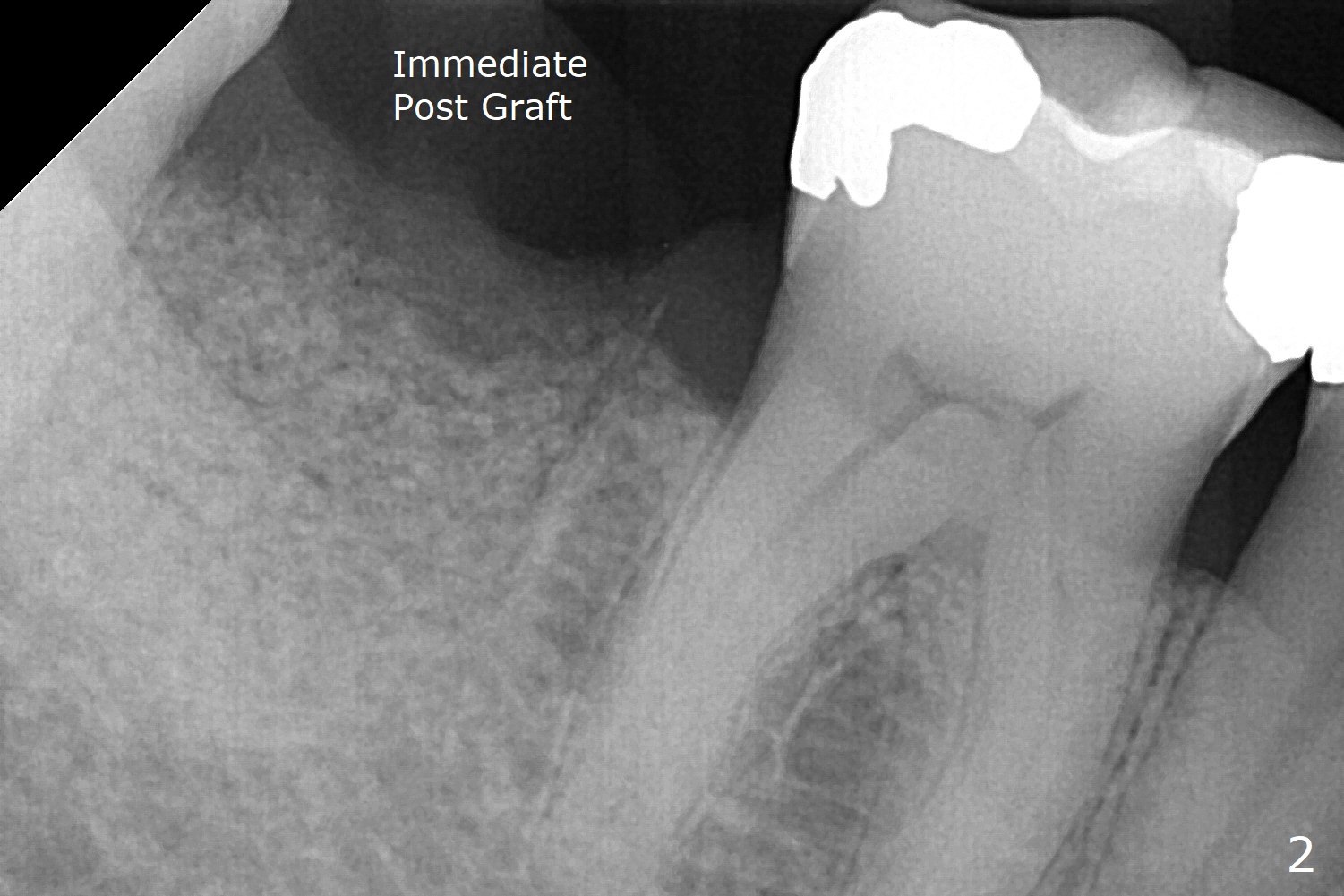
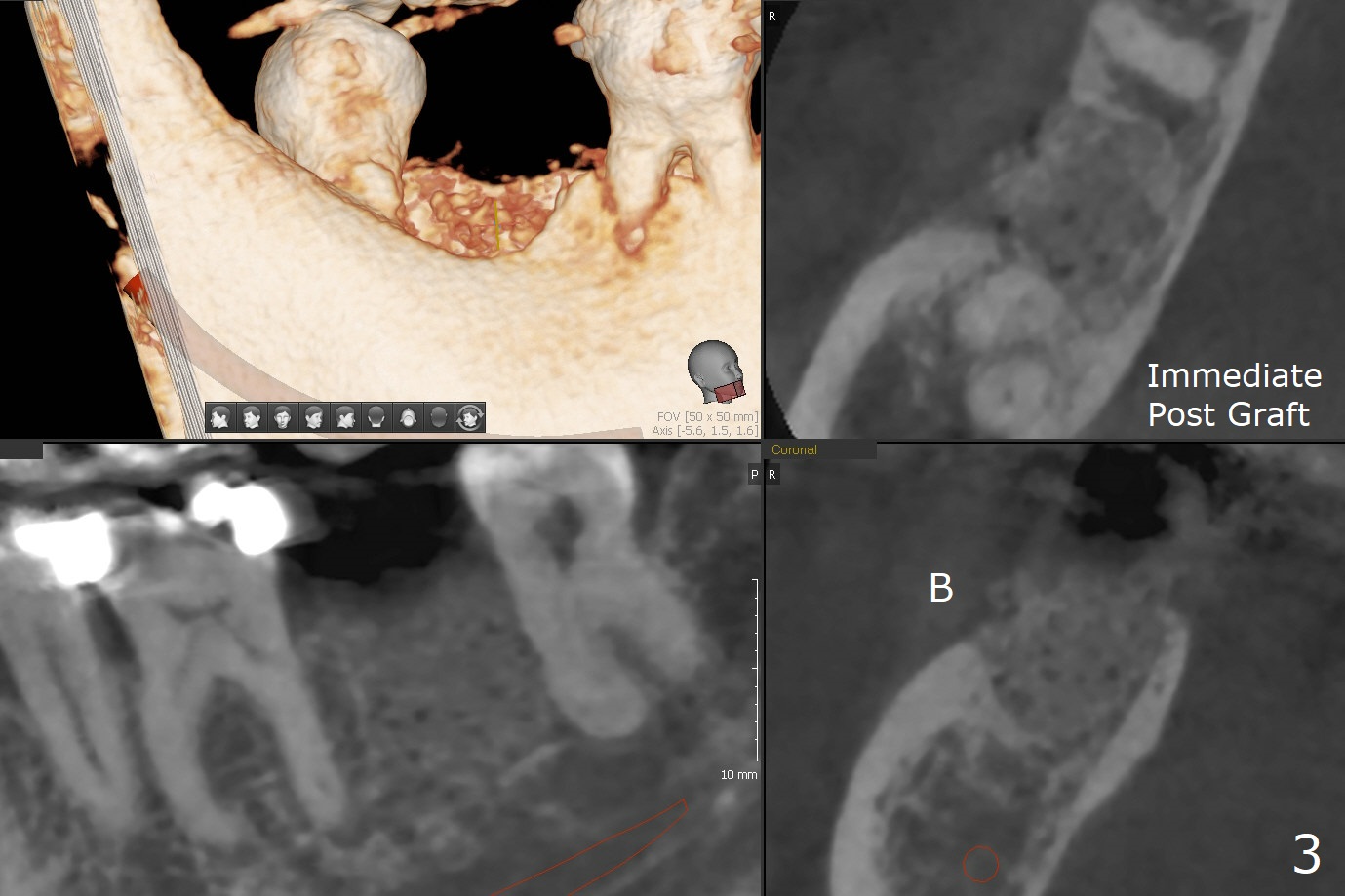
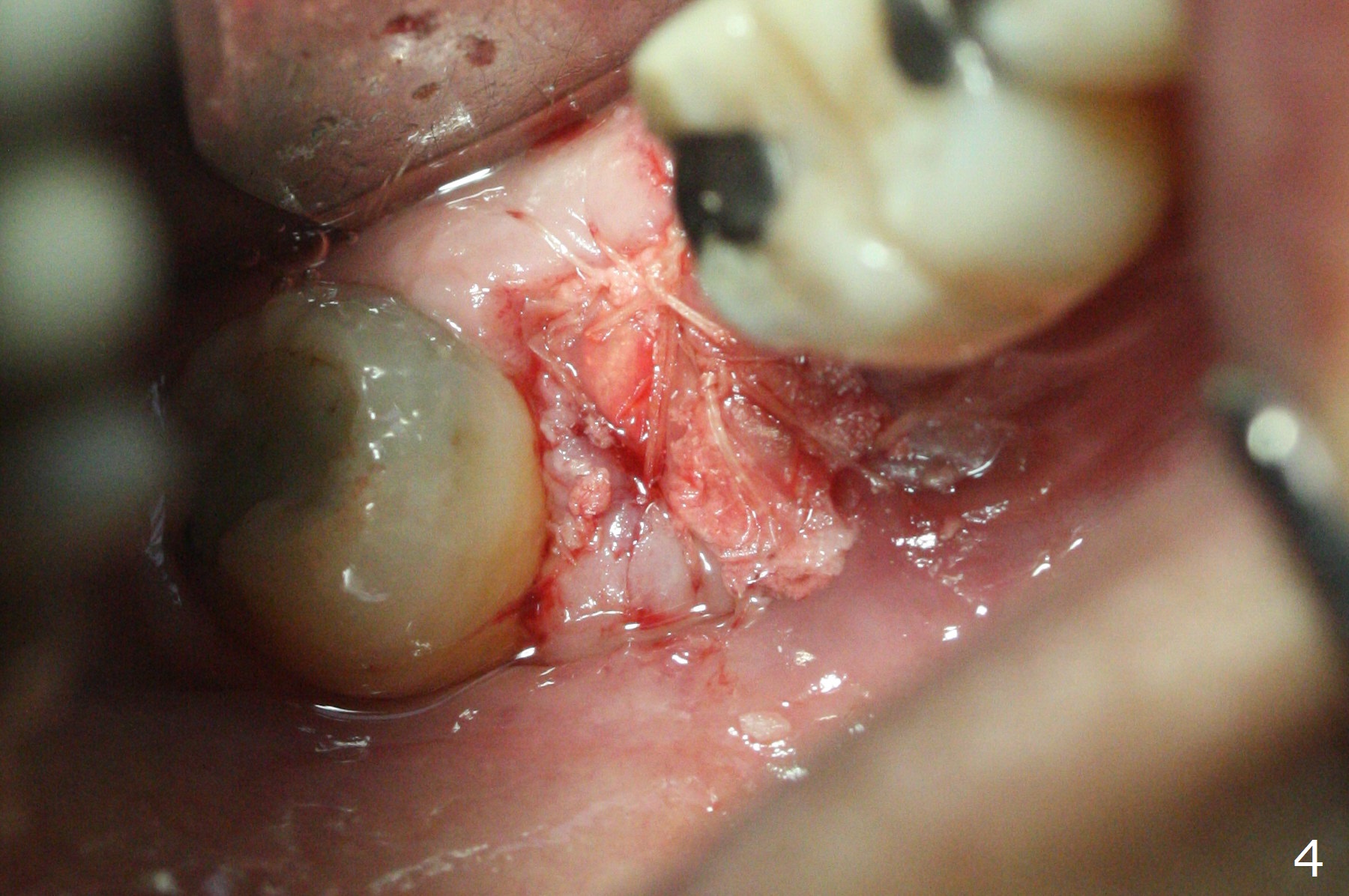
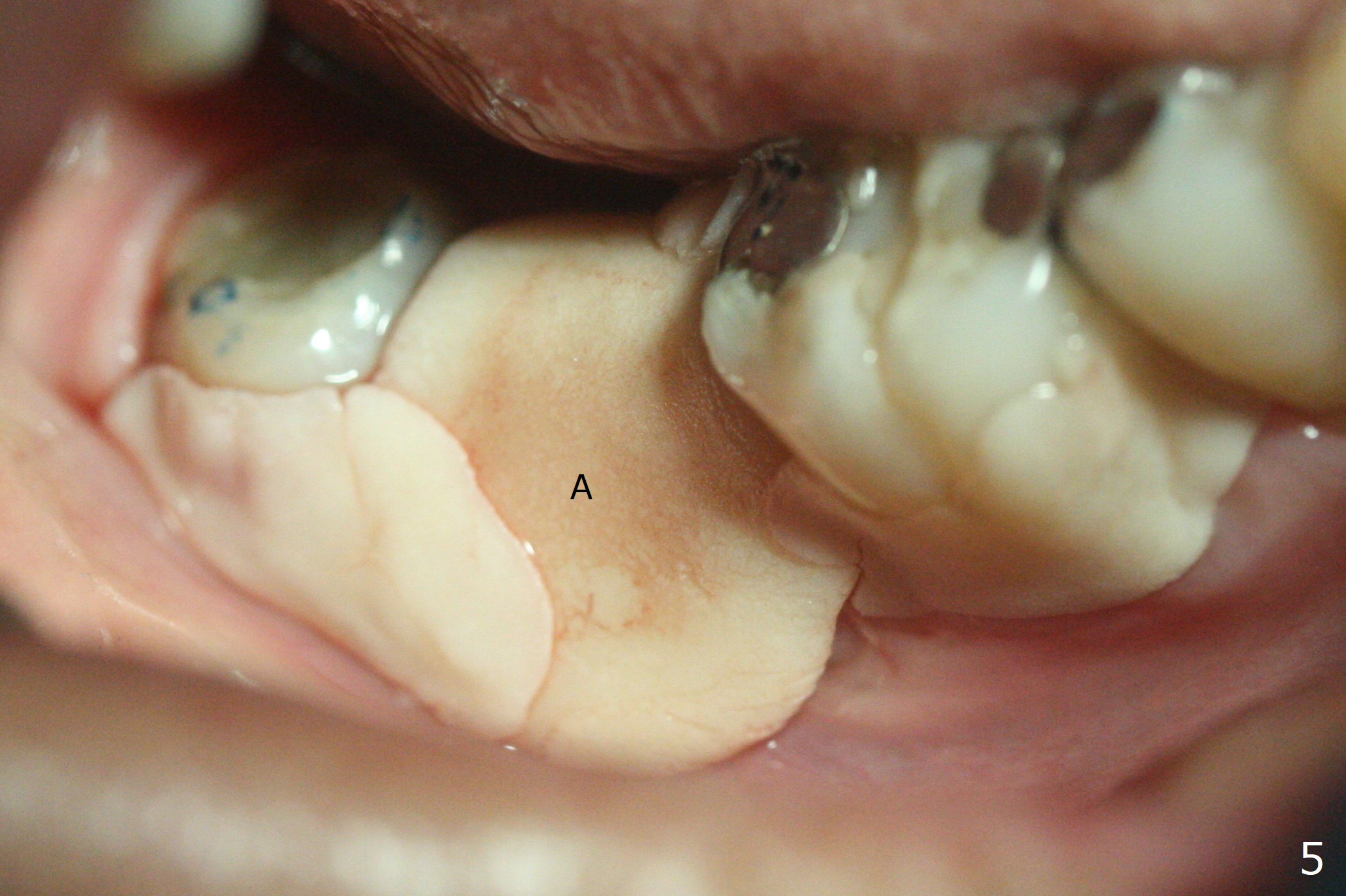
In fact the buccal gingival recession at #31 is asso-ciated with cervical caries perfor-ation (Fig.1 P). The debrided socket is packed with mine-ralized cortical: cance-llous mix (50:50) (better using mine-ralized cortical allograft (future particle size: 125μm – 850μm)) hydrated with ~ .25 ml of .3 mg/ml of rhPDGF-BB (one compo-nent of GEM21S, Fig.2,3). It is extremely difficult to close the socket opening with buccal defect with Osteogen Plug, 12x12 mm BioXclude and 4-0 PGA suture (Fig.4). Acrylic dressing is unstable in spite of several reline (Fig.5 A). Its replace-ment is GEM Cap RCM (regenerative collagen membrane), 9-12 month resorption time, which will be fixed in place with Perio Glue. Watch Video. In fact, 2 pieces of the reline dislodge in the 1st 2 days postop, while the whole piece 3rd days postop. The patient feels better when the acrylic dressing is out. It appears that the bone graft does not fall out, according to phone visit during coronavirus outbreak. A third method to close the buccal defect is to make mesial and distal release incisions (Fig.6) and transfer the flaps (Fig.7). In fact the bone graft gets lost, revealed over phone. Immediate implant is the most secure method to keep the bone graft. PRF may be more retentive. The fourth way is to place Cytoplast, which is fixed with spacer and periodontal dressing.
Return to
No Deviation
Plug
GEM21S
Cases
Next Case
Xin Wei, DDS, PhD, MS 1st edition
03/18/2020, last revision
09/19/2020