
.jpg)
.jpg)




.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
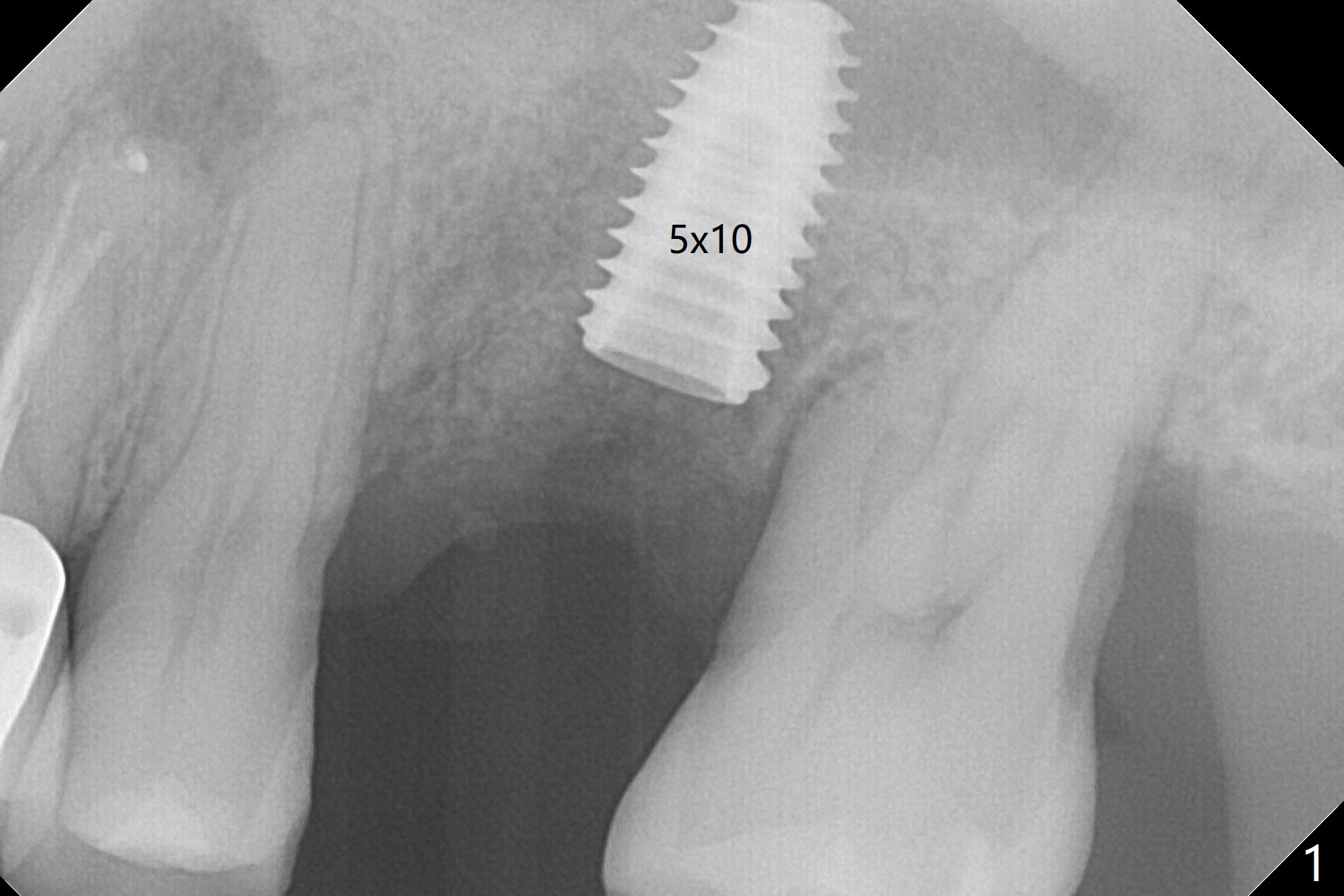
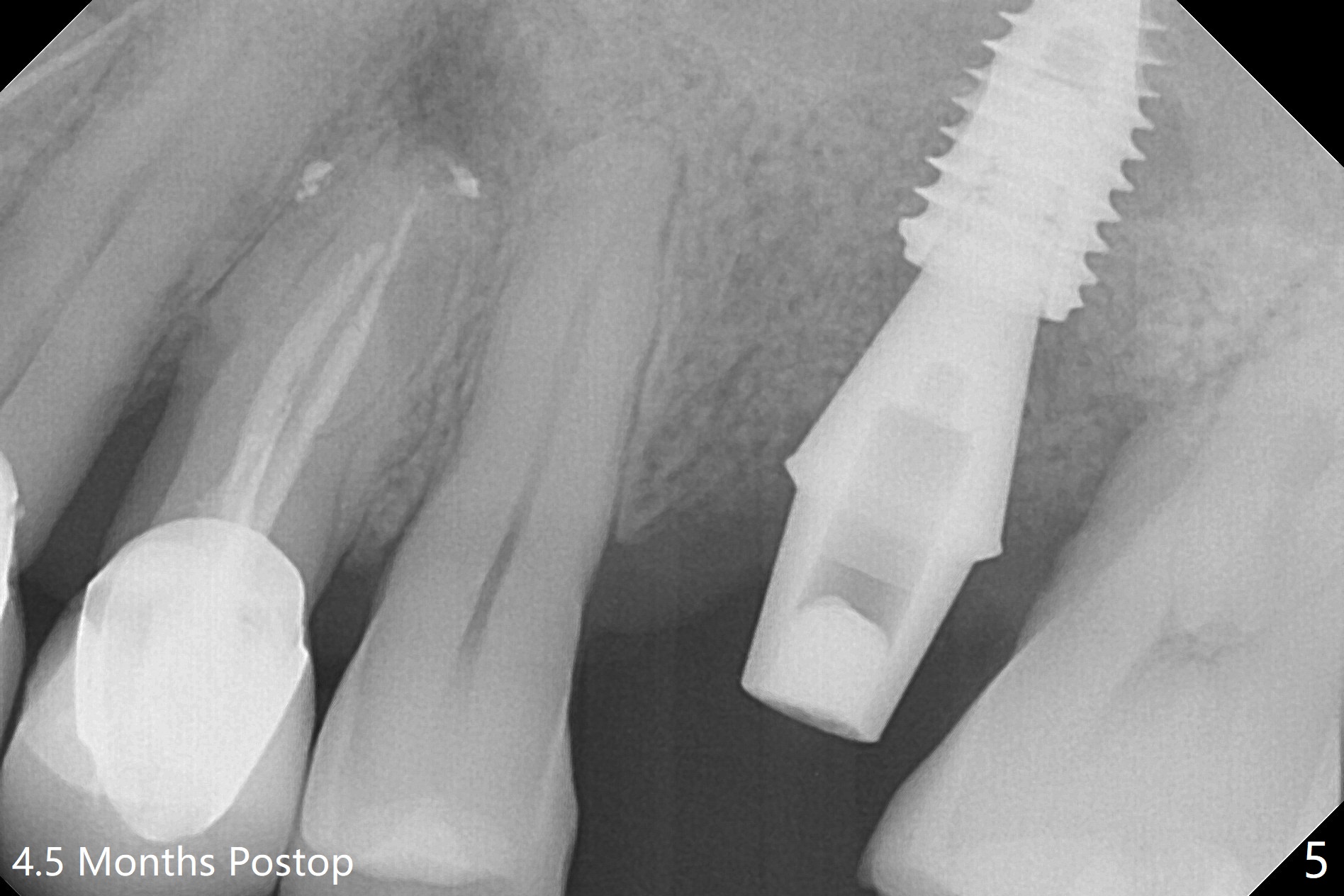
3rd Placement
Six months post 2nd placement at #14, the 5x11 mm IBS implant is unstable. The patient smokes a cigarette a day. After implant removal, the palatal wall of the osteotomy is intact, although low. With removal of minimal granulation tissue, a 5x10 mm IS dummy implant is placed with stability and slightly subgingival palatal (Fig.1,2). A 5x8.5 mm definitive implant is placed with ~ 40 Ncm and 3-4 mm subgingival palatal (Fig.3,4). A 5.7x5.5(5) mm abutment is placed to hold periodontal dressing in place. If the implant fails again, bone graft should be placed. The abutment and implant are stable 4.5 months postop (Fig.5); a provisional is fabricated for progressive loading. The provisional at #14 is narrow mesiodistally, while the tooth #15 is mesially tilted and shifted because of chronic periodontitis and 1 year 4 months of edentulism (Fig.6*). Limited orthodontics is necessary prior to final restoration. The 1st step is to raise the occlusion with #14 temporary reline (Fig.7 *); the tooth #15 is distalized initially with a separator, which is inefficient. It appears that brackets and bands should be placed for distalization. A month post banding, open coil spring is placed between #14 and 15; with occlusal composite on the opposing tooth (#19) (Fig.8), the tooth #15 is distalized instantly probably related to its periodontal condition (Fig.9 mirror view). The tooth #15 is further distalized 2 weeks post open coil spring placement (Fig.10). To act an anchorage, the abutment needs to be torqued with wrench (25-30 Ncm) and the provisional has to be permanently cemented. The distalization appears to be ~ 1 mm shy 1.5 months post open coil (Fig.11).
Return to
Upper
Molar Immediate Implant,
Armaments,
Ortho
Xin Wei, DDS, PhD, MS 1st edition 05/04/2018, last revision 01/04/2019