


|
|
|
|
|
|
|
|
|
|
|
|
Prevent Debracketing M
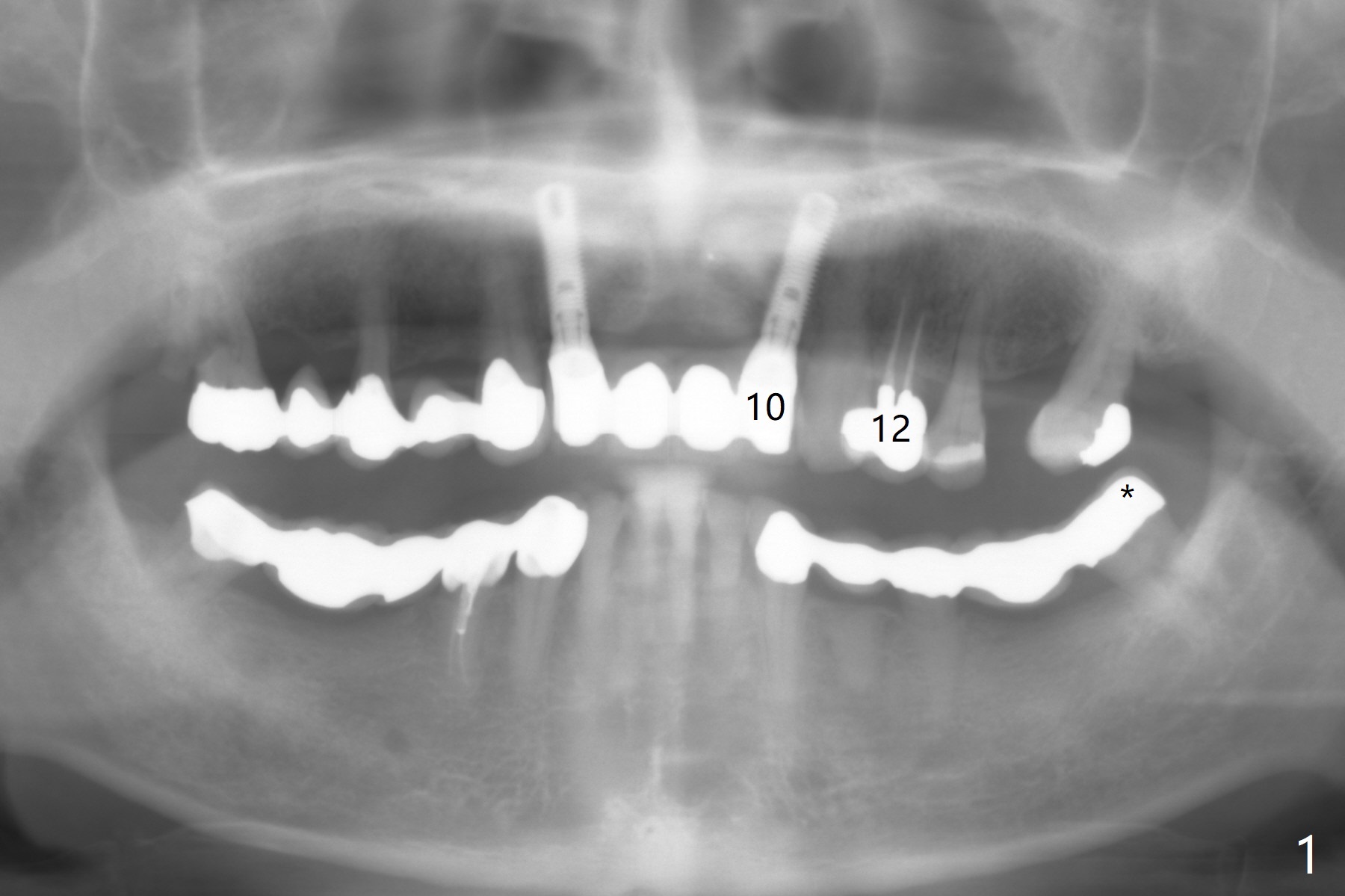
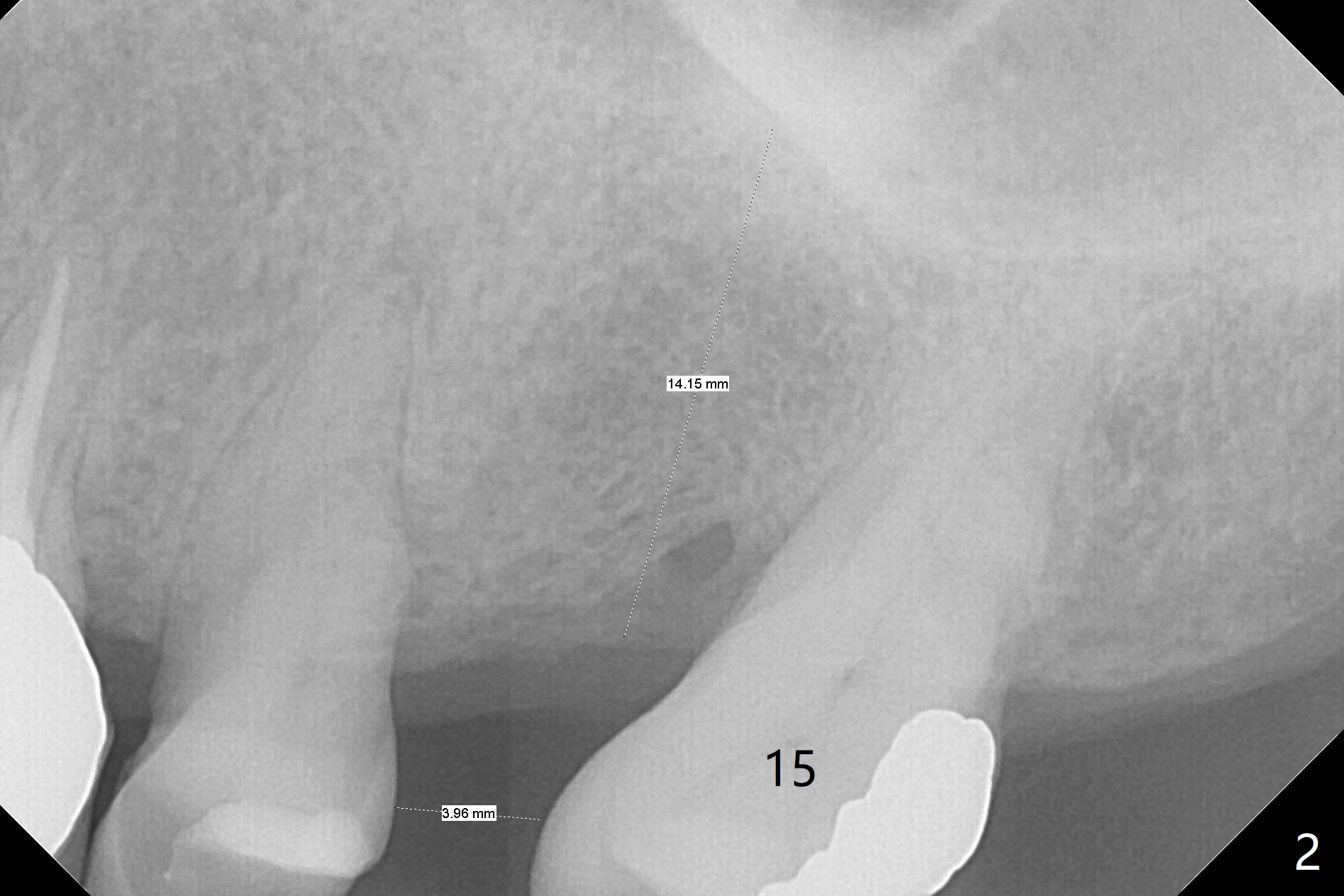
A 64-year-old man has multiple restorations. The tooth #2 seems to have root resorption. The tooth #27 has recently finished RCT. It appears necessary to establish sound occlusion on the left side by placing an implant at #14. First at all, the mesially tilted tooth #15 needs to be uprighted (Fig.2). The implant crown at #10 will be used as an anterior anchorage, since the three teeth (#11-13) are usually not strong enough to distalize the 2nd molar. To prevent debracketing at #10, a diamond bur will be used to roughen the crown surface and new bonding agent is applied. The second easily debracketing spot is #12 (crown), which could be used bicuspid band. The 3rd option to reduce debracketing is not to use rectangular wire initially. When the space at #14 increases to 8 mm mesiodistally, an implant will be placed. Once the implant is osteointegrated, a band is applied. From that point on, a rectangular wire could be used. If debracketing occurs at #10, it does not matter, as the posterior anchorage has taken over. Save all of wires used initially, since wires may have to return to thinner ones when #14 band is loaded. To unlock the occlusion (to distalize #15 without interference), composite will be applied to one of FPDs on the right side. The distal marginal ridge of the tooth #18 (Fig.1 *) may need to be trimmed.
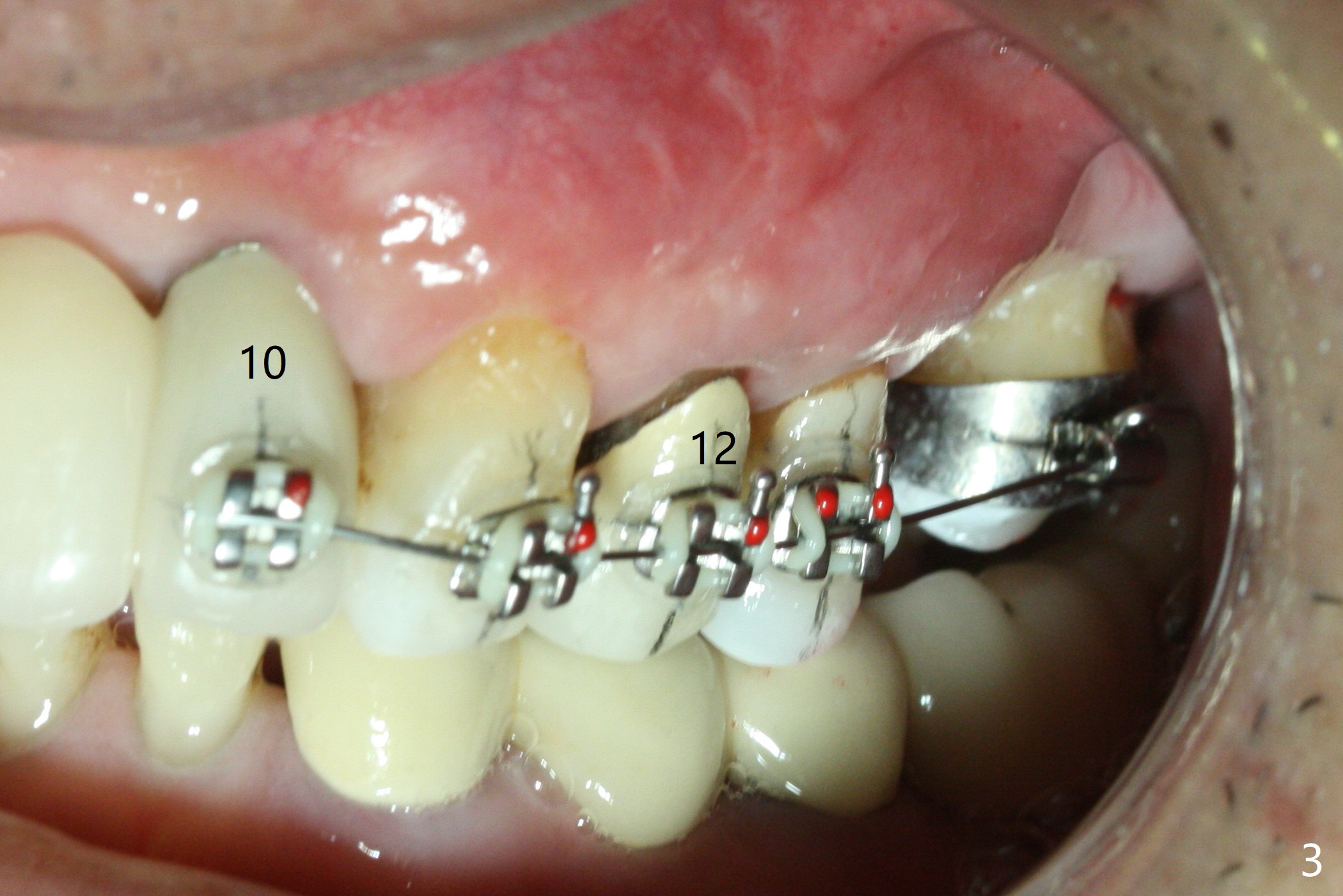
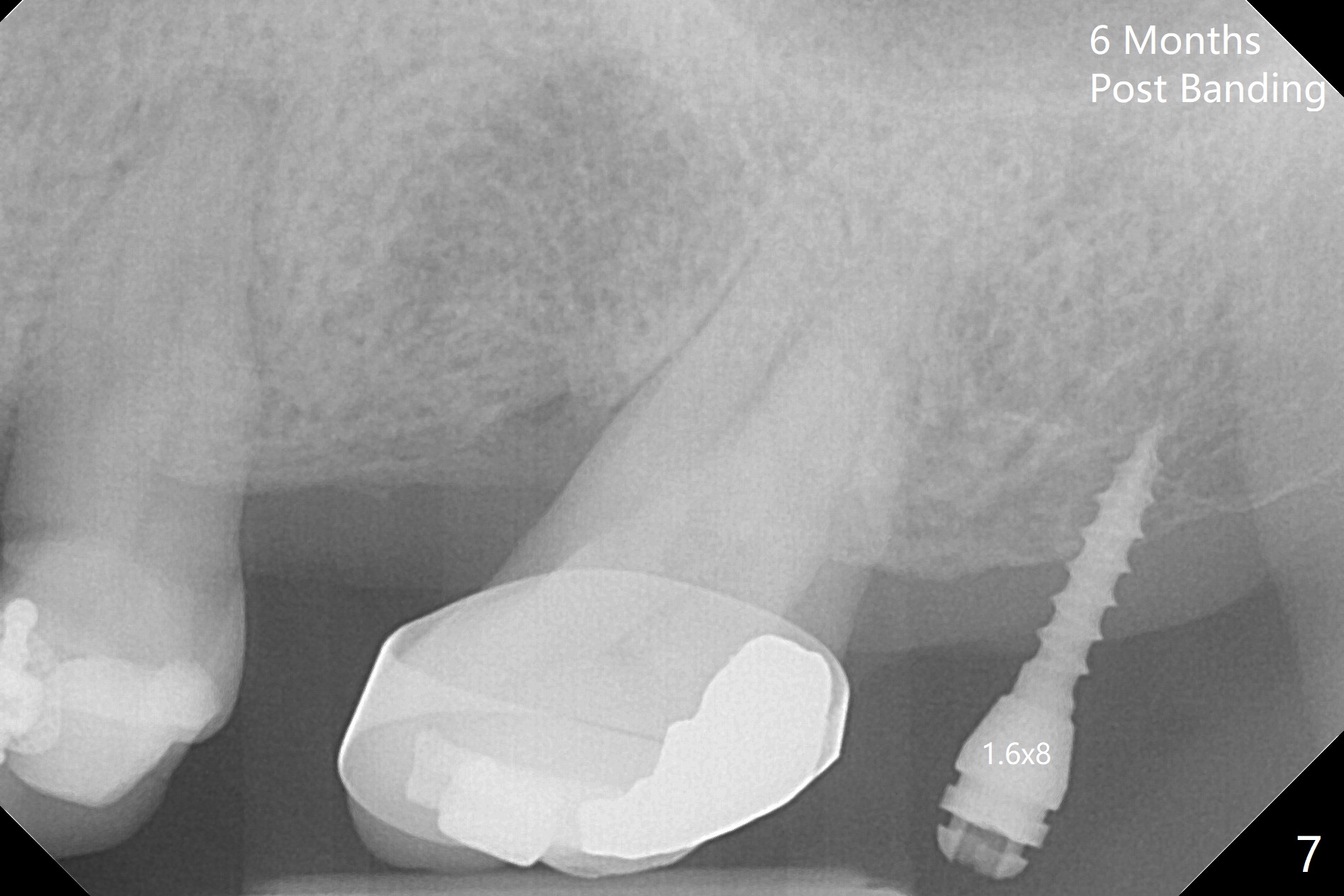
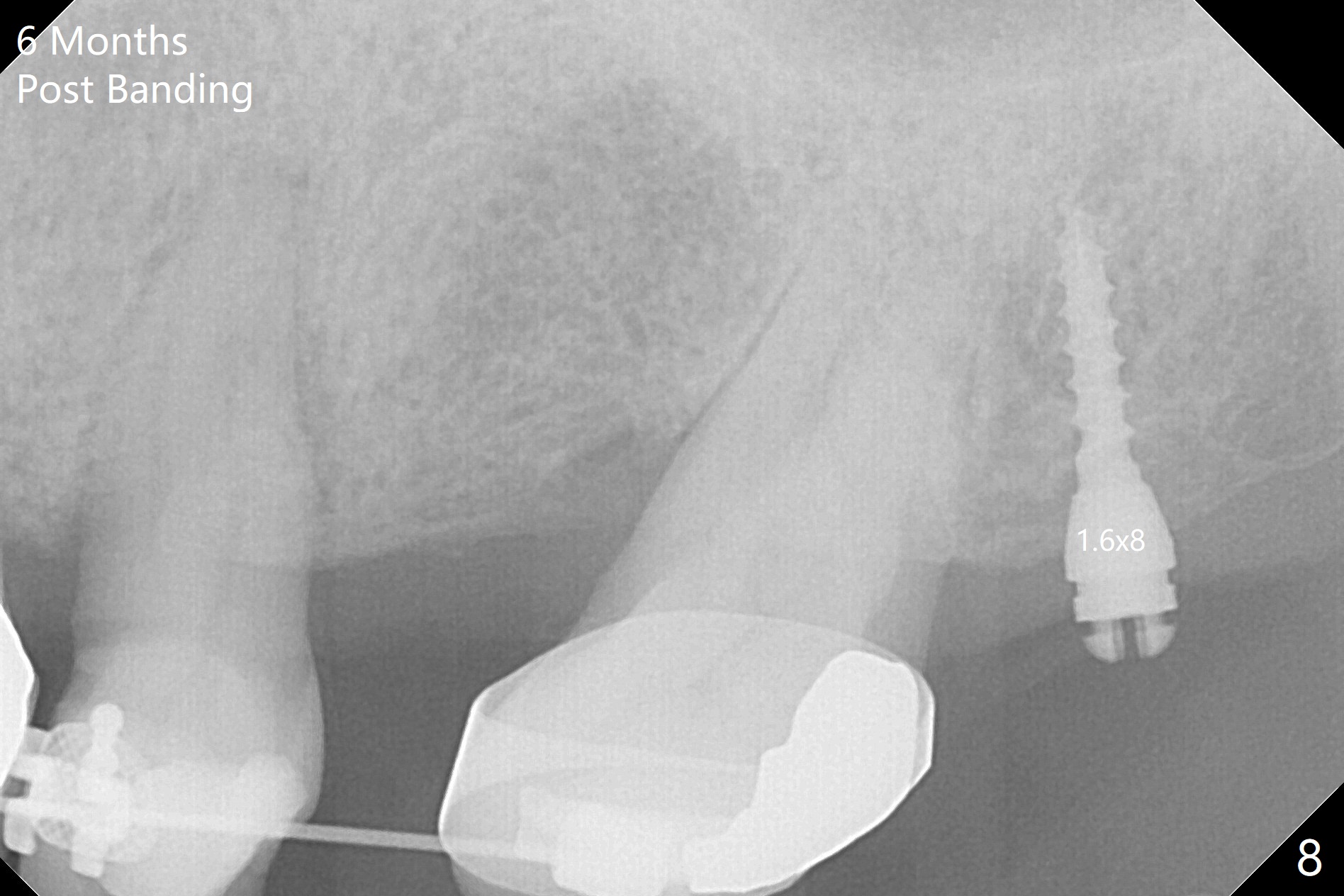
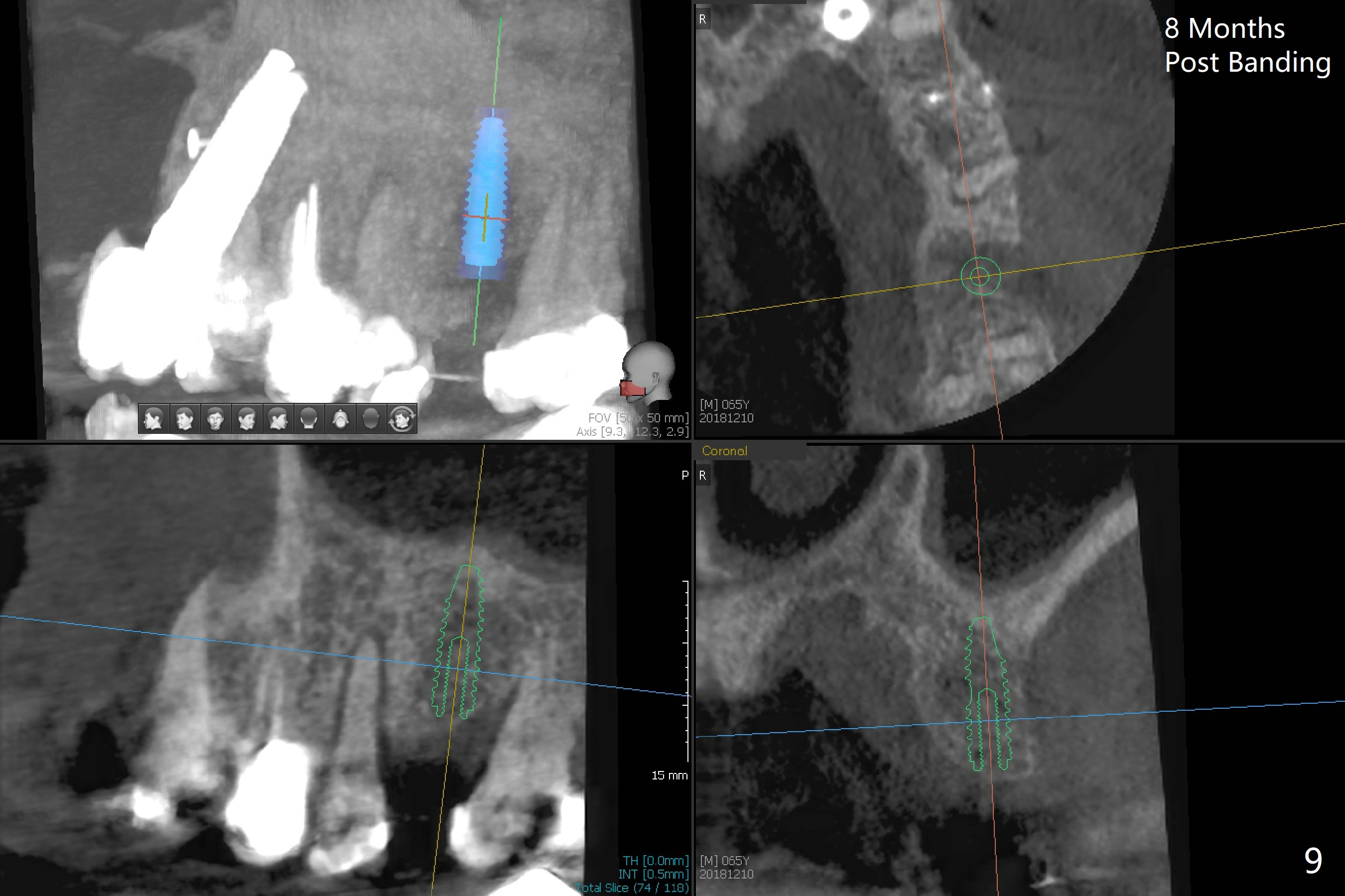
Ultradent Prime and Bond is used bracketing. The bonding system appears to be able to attach the brackets to porcelain crowns at #10 and 12 (Fig.3 (14 niti wire)). The 14 niti wire is not fully engaged (Fig.4). An open coil spring is used when the wire changes to 18 ss (Fig.5,6). Composite is placed to have clearance for UL7 to be distalized (Fig.5 *). To have the best anchor involving the implant at UL2, ligature wire is used between UL2-5 (Fig.6). In fact the anterior teeth are not good anchor. The bracket detaches from UL2 (implant) and UL5 keeps rotated, while UL7 is not distalized when open coil spring is placed between UL5-7. Nearly 6 months post banding, a 1.6x8 mm anchor pin is placed (Fig.7,8). Next visit the pin is loose and replaced with a ball type 1-piece implant (2x10(2) mm). Although the latter remains apparently stable, UL7 appears to remain in place. It seems necessary to place a restorative implant at UL6 as a future anchor (Fig.9: 3.5x11.5 mm).
Return to Upper Molar Immediate Implant, Armaments, Ortho Cases, Trajectory, 2/3 下一例 矫正,糖尿病,种植水平 植牙,导板与正畸 Xin Wei, DDS, PhD, MS 1st edition 04/09/2018, last revision 01/03/2021