
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cement Uniposts or Not
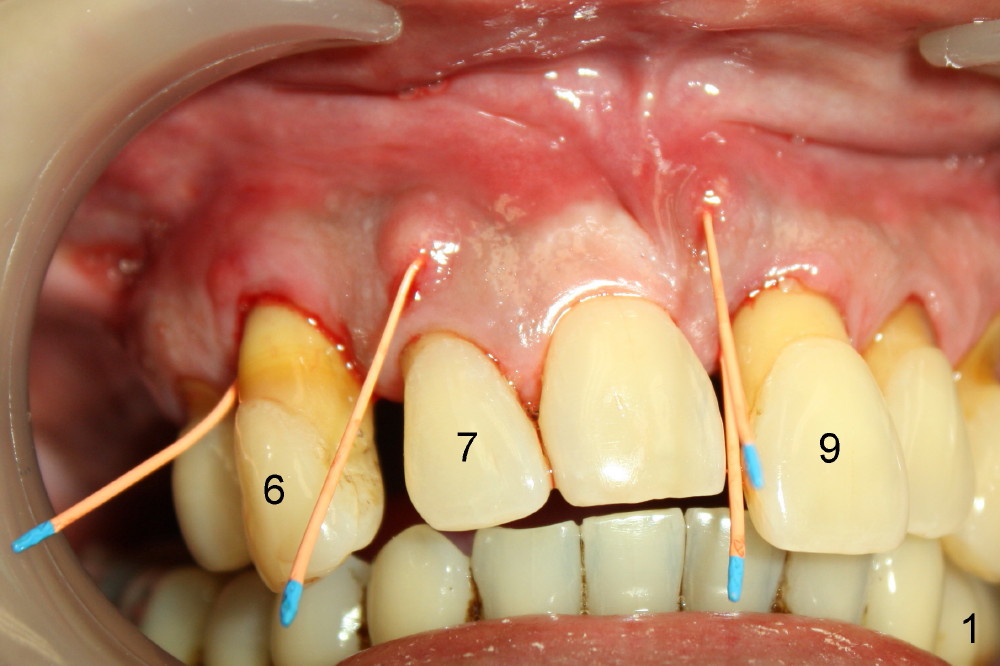
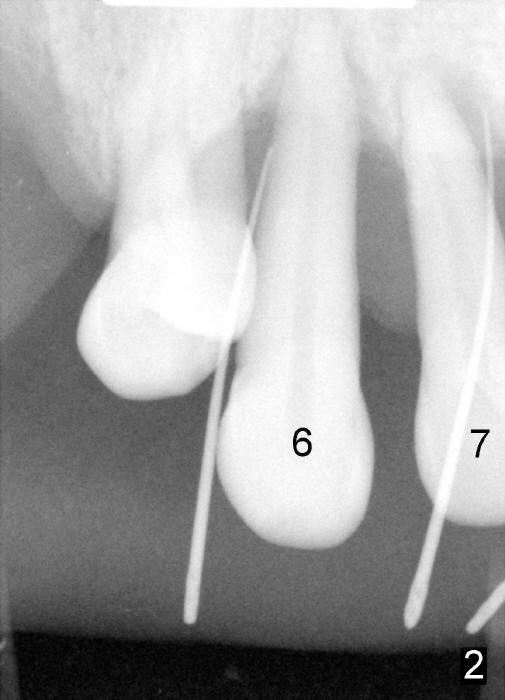
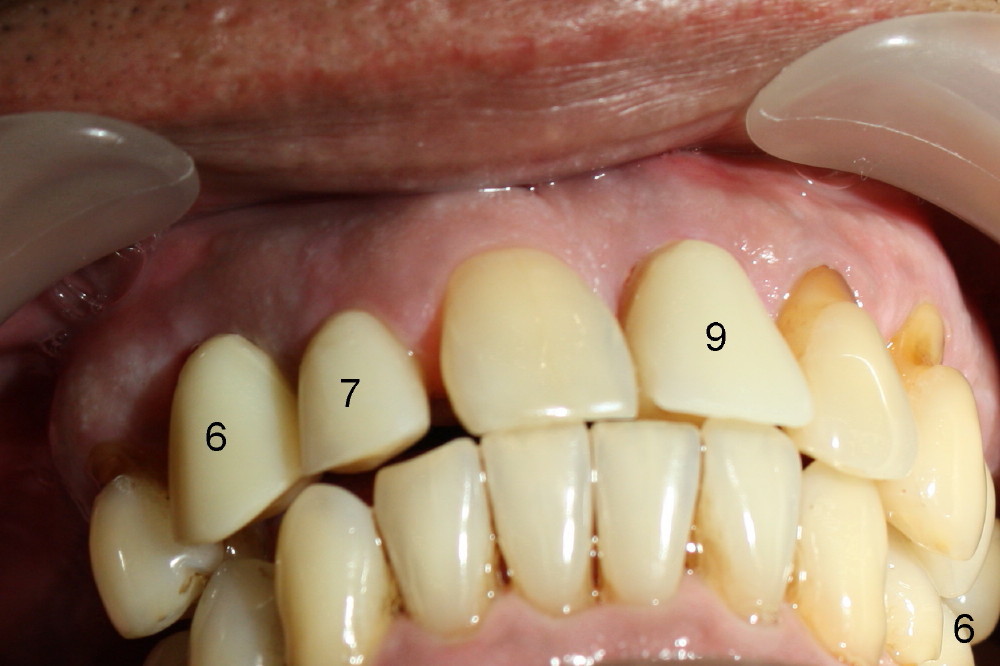
A 52-year-old man has severe periodontal disease (Fig.1-3). It appears that the upper teeth are non salvageable and are best treated by hybrid denture. But his finance is strained.
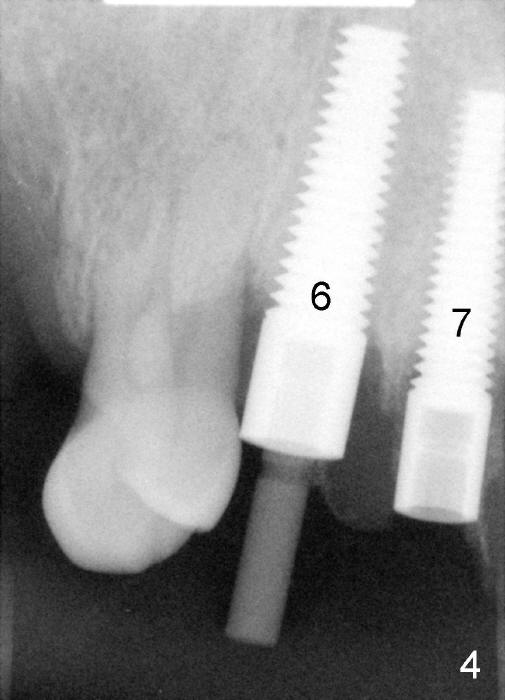
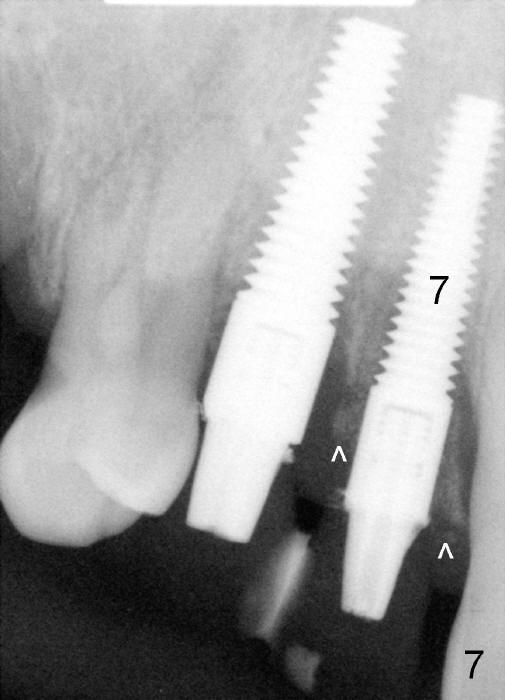
The most severely affected teeth (#6,7 and 9) are extracted and immediately replaced by 4x20 mm (#7) and 5x20 (#6,9) implants (Fig.4,5). Straight (0 degree) uniposts (3 and 4 mm, respectively) are rotated tightly into the wells of the implants by hand screw driver. In order to have reversibility to hybrid denture in the future, these uniposts are not cemented. Heavy retention grooves are placed between the uniposts and implants. Provisionals are fabricated immediately and cemented temporarily. To increase stability, flowable composite is added to the area between the provisionals of #6 and 7.
Fig.6 shows these provisionals 1 week postop. The patient is happy with the result. His diet is confined to soft food. The provisional at the site of #9 is slightly mobile.
Tomorrow (1.5 months postop) the patient will return because of a loose temporary crown. What should I do? Retighten the loose unipost or permanently cement it?
When fabricating definitive crowns, can we afford not to cement the uniposts so that convertibility into hybrid denture is possible?
Dr Wei, I do not like hybrid dentures, my personal bias. I would cement posts and splint crowns from #6 - #9. Neither is wrong ! Dr B
Dr. Wei, Of course me not being a clinician I can only comment from a mechanical viewpoint. If straight abutments are used, and large, deep vertical grooves are used extending onto the implant itself, it should work. In early years, Dr. Tatum didn’t cement straight abutments all the time either. Tony
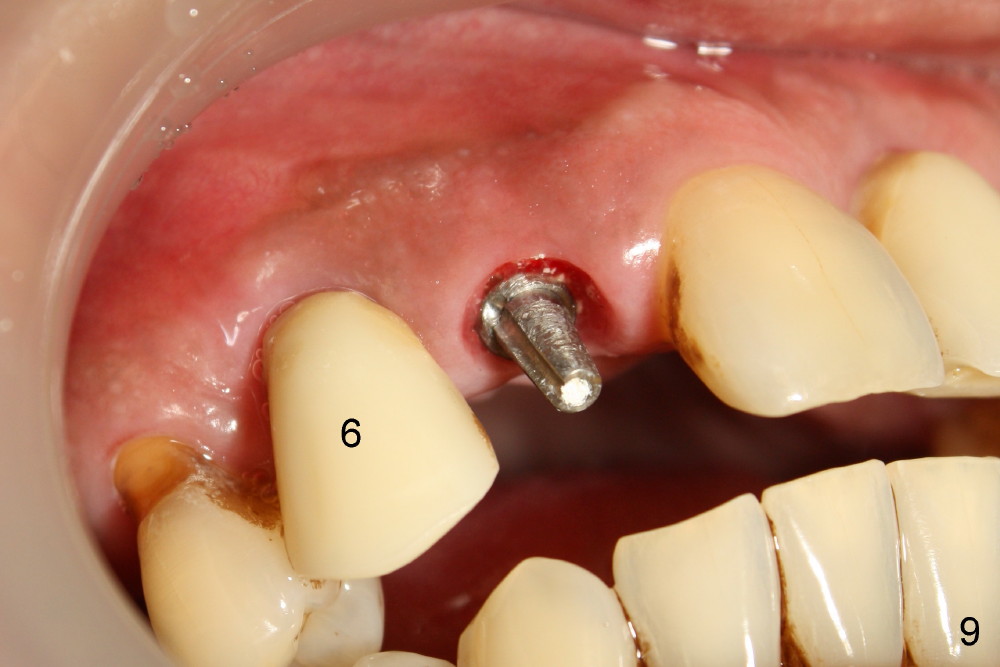
Dear Tony and Dr. Borgner: Thanks for the input. The patient showed up today. The provisional of #7 is off (Fig.9) and then recemented and bonded to the provisional of #6 with flowable composite. Open the magnified Fig.9 to see whether the vertical groove is wide and deep enough or not. By the way, the diameters of the implant and of the abutment are 4 and 3 mm, respectively.
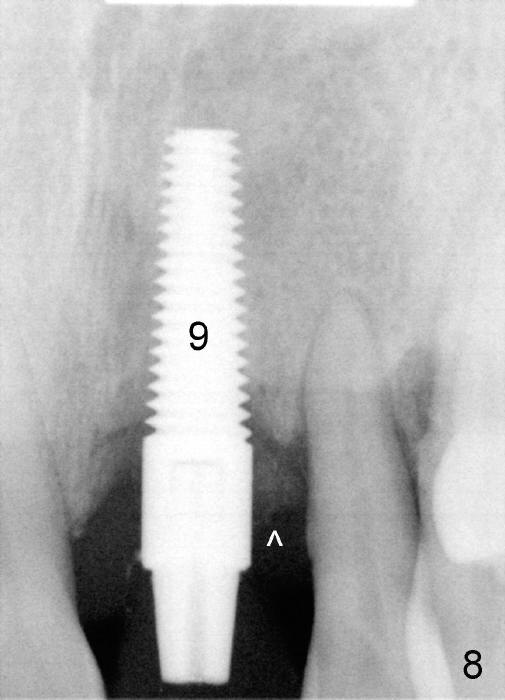
The provisional of #9 is still wiggling a little bit buccolingually. It is probably due to loose connection between the implant and the abutment, although follow up PAs do not support it (Fig.7,8; ^: bone graft at the time of immediate implants).
Xin Wei, DDS, PhD, MS 1st edition 12/16/2013, last revision 12/18/2013