

|
|
|
|
|
|
|
|
|
How Does Immediate Implant Help Close Buccal Apical Defect Without Bone Graft?
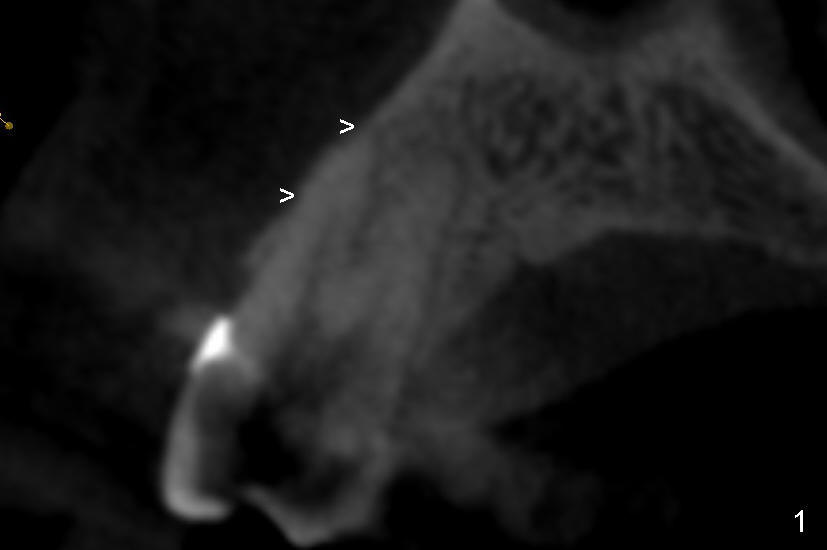
It is known that that buccal wall (apical) of anterior teeth including bicuspids is thin (Fig.1 between arrowheads). Fig.1 is a CT coronal section of an upper first bicuspid, whereas Fig.2 is a diagram showing after extraction. We are going to show how immediate implantation is to push the septum buccally (arrow) to close the buccal apical defect.
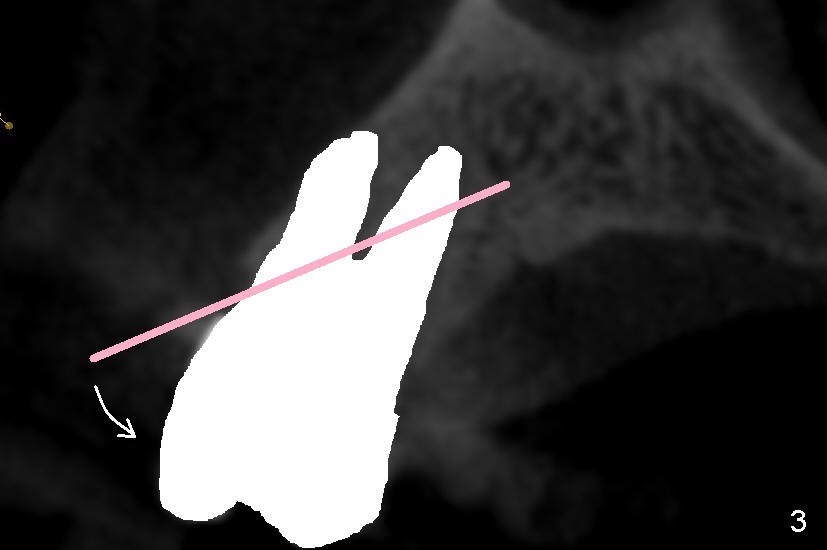
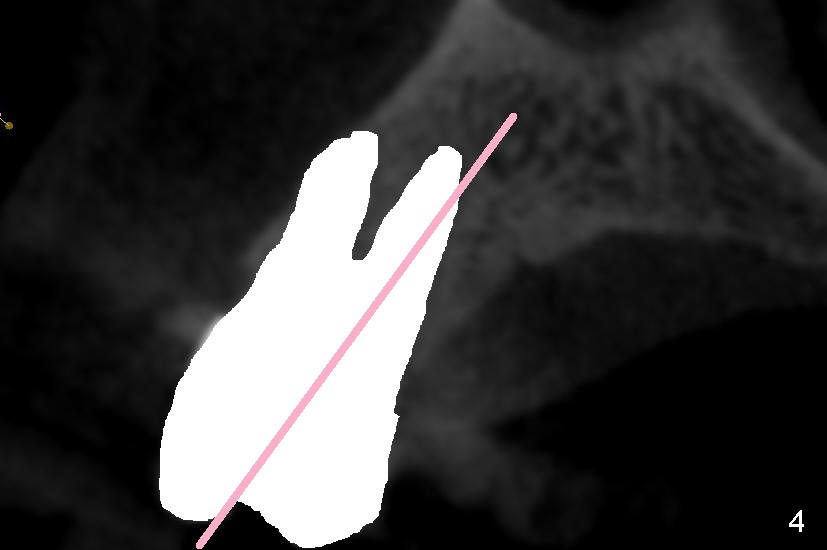
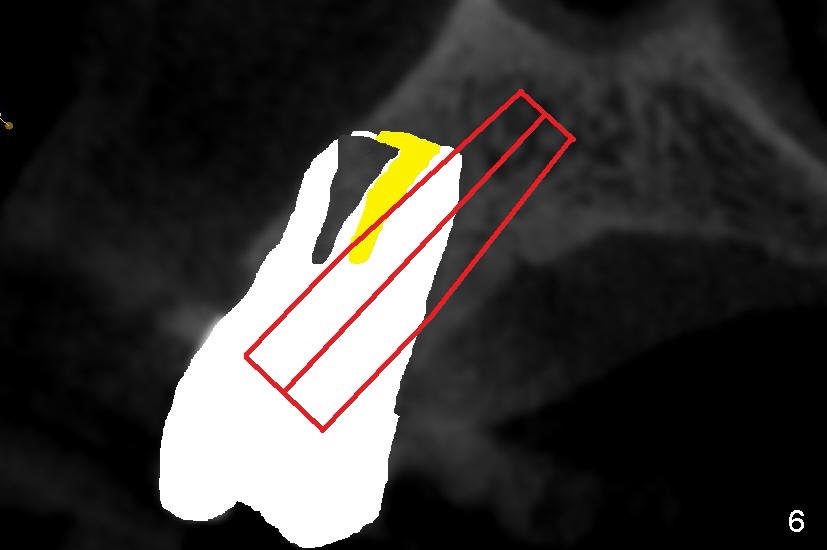
Even in a single root socket, osteotomy is to be created in the palatal wall. To get a "catch", a drill or osteotome (RT for example; Fig.3 pink line) is placed more or less perpendicular to the palatal wall. Once the catch is achieved, the axis of osteotomy is changed (Fig.3 curved arrow), more or less parallel to the bone morphology (buccal and/or palatal walls, Fig.4). Gradually the osteotomy is increased in diameter (Fig.5 pink area). In the single root, a separate, palatal socket has been created with formation of a septum. Subsequently, taps and the implant (tapered, Fig.6 red portion) will push the existing or just formed septum buccally (from yellow area to grey area). The fractured and displaced septum is going to participate in repairing the buccal apical defect if the pre-existing infection is under control under protocol proposed by Tatum group.
Xin Wei, DDS, PhD, MS 1st edition 06/22/2013, last revision 09/14/2014