Surgical Exposure of Impacted Upper 2nd Molar?
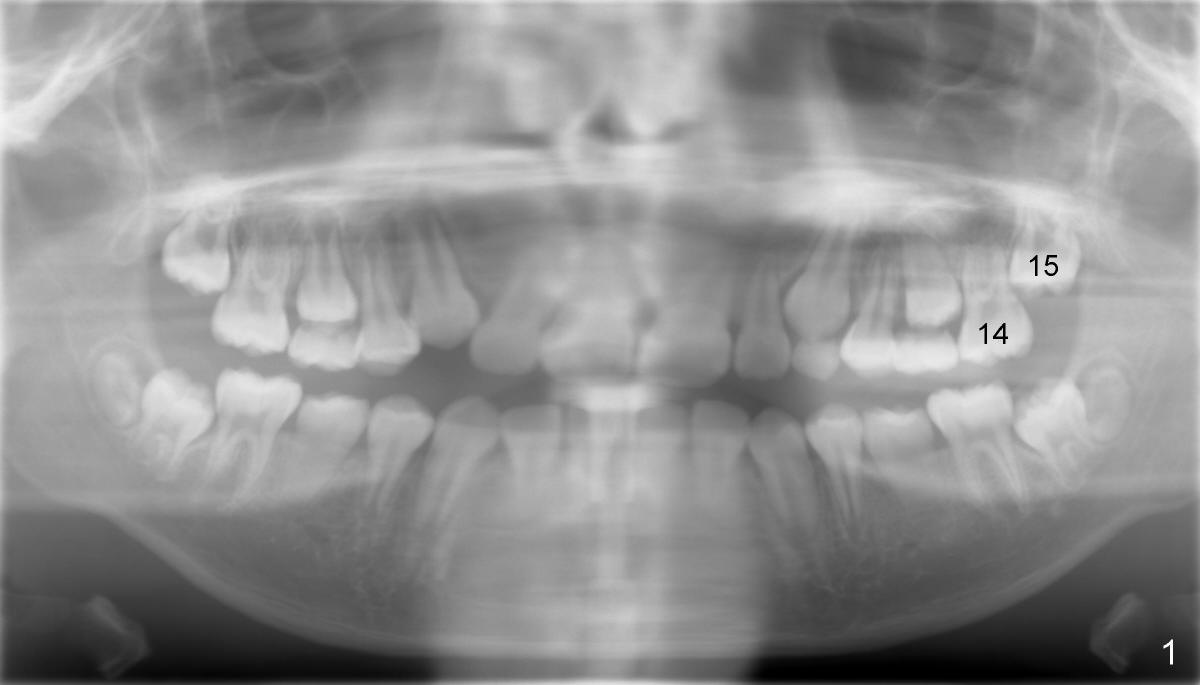
An eleven-year-old Chinese boy presented to my office for new patient exam in
2009. Panoramic X-ray shows crowded dentition (Fig.1).
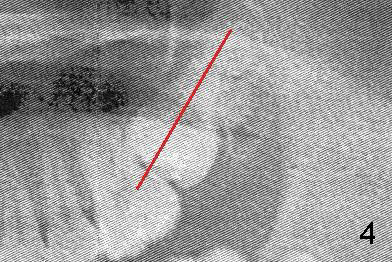
Orthodontic treatment was finished by a specialist in 2012. Post-op X-ray
shows that the tooth #15 (upper left 2nd molar) is impacted (Fig.2).
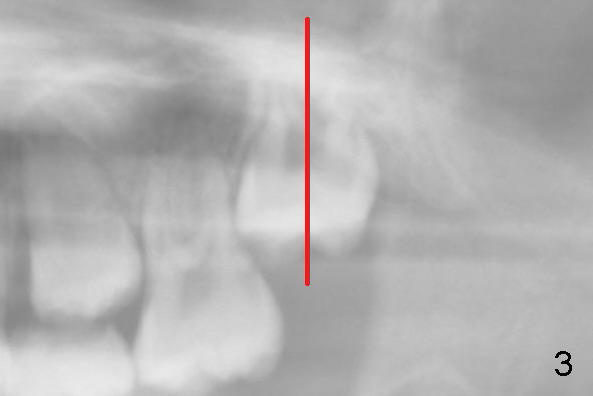
Fig.3 and 4 are magnification of Fig.1 and 2, respectively, demonstrating the
change in the axis of #15 from 2009 to 2012 (red line).
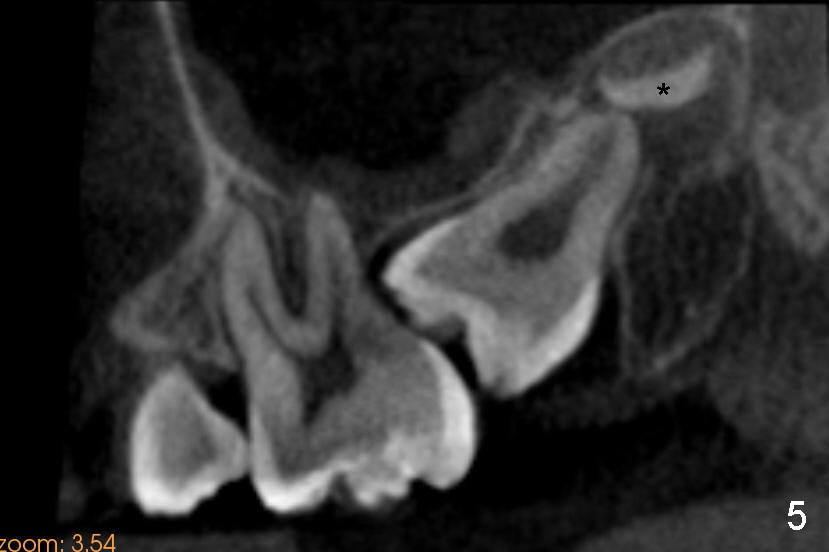
Cone-beam CT confirms the impaction of #15 (Fig.5).
The palatal apex is closing. The asterisk (*) is the tooth bud of #16 (3rd
molar).
What is the treatment plan?
Hi Xin,
Incredible bad luck Xin. And my first choice would be to have the surgeon or
your self luxate the tooth kindly, in an
effort to change the axial inclination. It seems to me when I have done this
in the past it has been with lower second molars. I do not ever remember an
upper second molar. Some type of material may be required to create distance
between 14 and 15. The tooth generally survives the procedure and does not
require RCT. However, that is the worst case scenario. I know of an example
where the tooth did require RCT. Bears losing the tooth though. Now, your
ace in the hole: If the third molar develops into a viable tooth, it can be
substituted for the second molar. But currently, I am not willing to go that
route because it looks very immature, and who knows what will become of it?
Tim Shaughnessy, DDS (orthodontist in Atlanta) 11/18/2012
Xin Wei, DDS, PhD, MS 1st edition 11/17/2012, last revision
11/18/2012