|
|
|
|
|
|
|
|
|
Mesiodens Does Not Cross Midline Suture
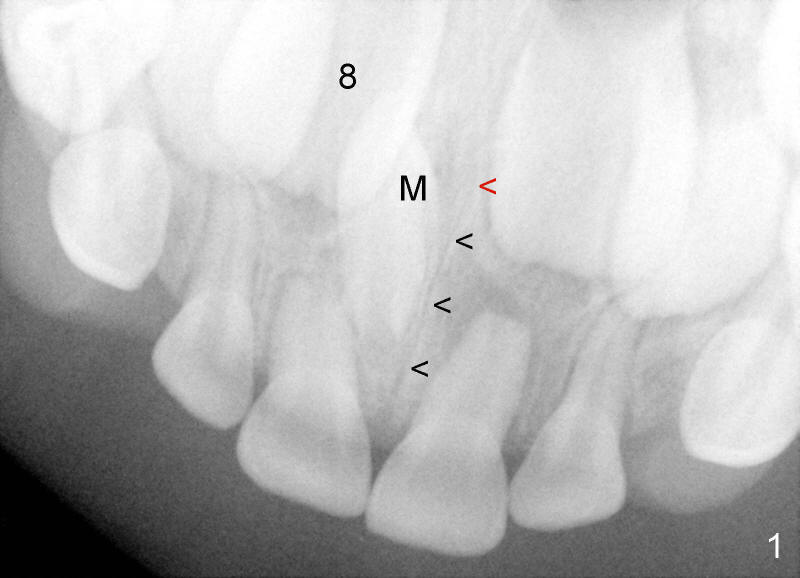
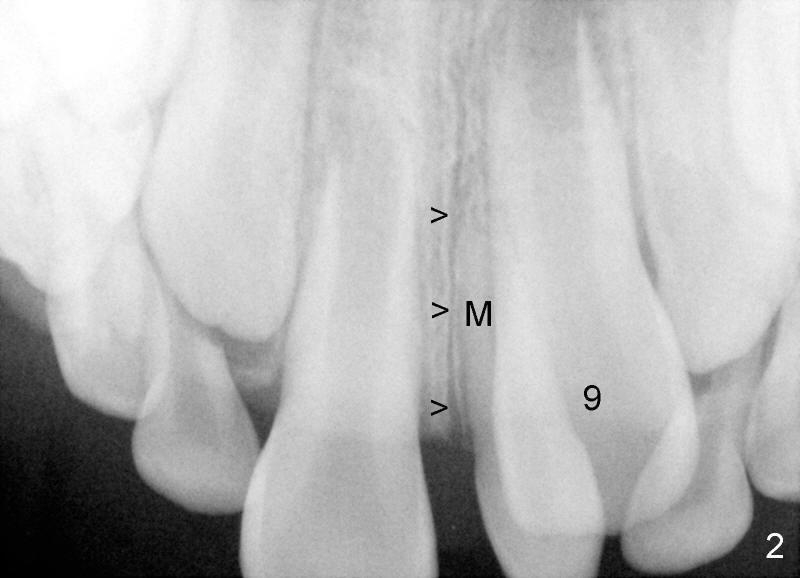
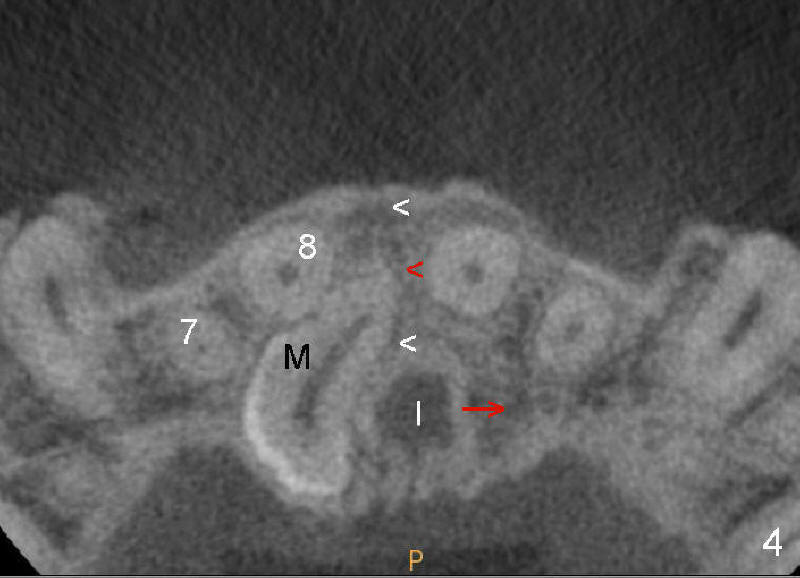
Crown of mesiodens (M) may be oriented toward apically (Fig.1), coronally (Fig.2) or palatally (Fig.4 axial section of CBCT). A common characteristic of mesiodens is that it does not cross midline suture (Fig.1,2 black arrowheads, Fig.4 white arrowheads), although it can push and deform midline suture (Fig.1,2,4 red arrowheads).
The mesiodens in Fig.1 should be removed because its potential upward growth may interfere with #8 eruption. The PA is taken when the patient is 5.5 years old. The surgery is done when the patient is 6 years old. Initially the mesiodens is difficult to locate through buccal approach. It appears that CBCT is required prior to surgery to reduce surgical trauma.
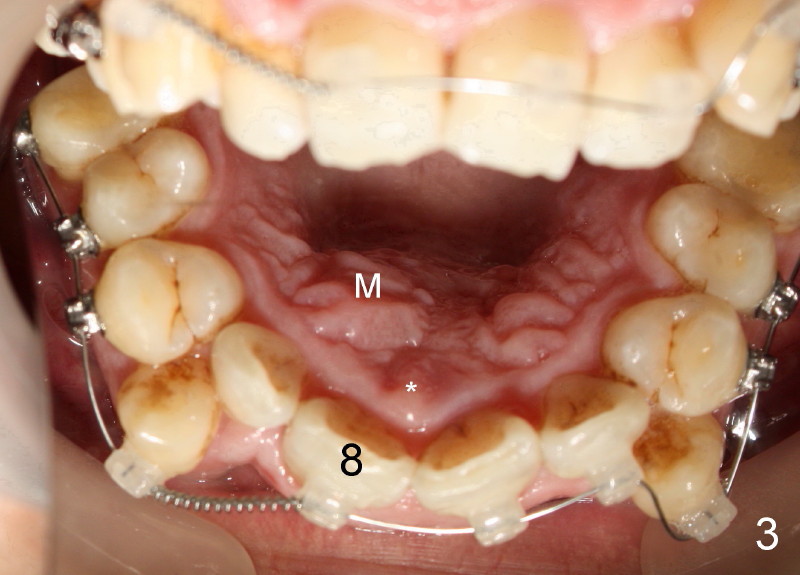
When a 39-year-old man presents for new patient exam and possible orthodontic treatment, PA shows a mesiodens associated with #8. Without careful basic exam, CBCT is ordered to determine surgical approach.
CBCT shows that the crown of the mesiodens is palatal (Fig.4: P). Second visual exam of the palate demonstrates an elevation (Fig.3: M) lateroposterior to the incisal papilla (*, a midline structure). It appears that CBCT is not so critical in deciding surgical approach for this case.
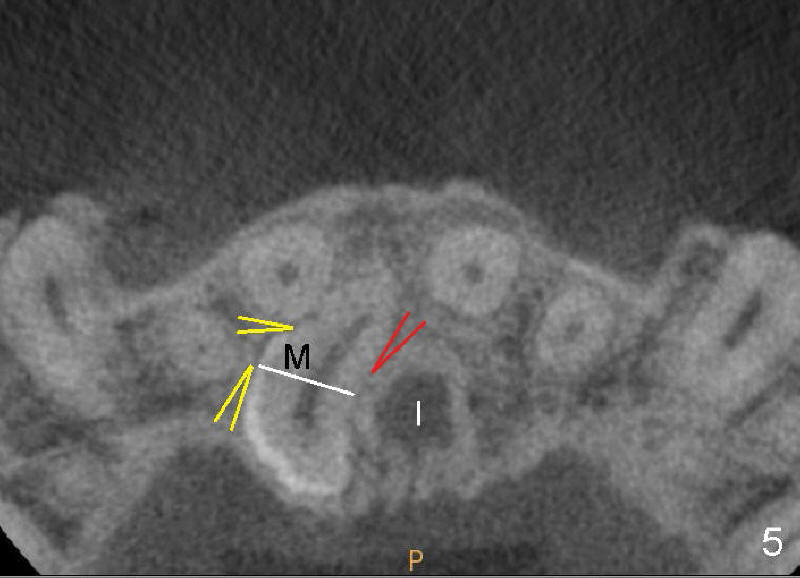
There is no problem to expose the mesiodens palatally with mucoperiosteal flap reflection. But the mesiodens is difficult to be luxated after placement of purchase point lateral to the mesiodens (Fig.5 yellow arrowheads). The supranumerary tooth is sectioned (white line). The coronal portion is easy to be removed, but the radical portion is stable (probably ankylosis). Out of desperation, a purchase point (red arrowhead) is placed between the mesiodens and the incisal canal (I). It helps remove the root, but there is oozing after suturing flap. It seems that the neurovascular bundle is violated when the medial purchase point is made.
Although the midline suture and the incisal canal can be pushed to the other side by the expanding mesiodens (Fig.4: red arrowhead and arrow), the mesiodens does not seem to be able to grow across the midline suture.
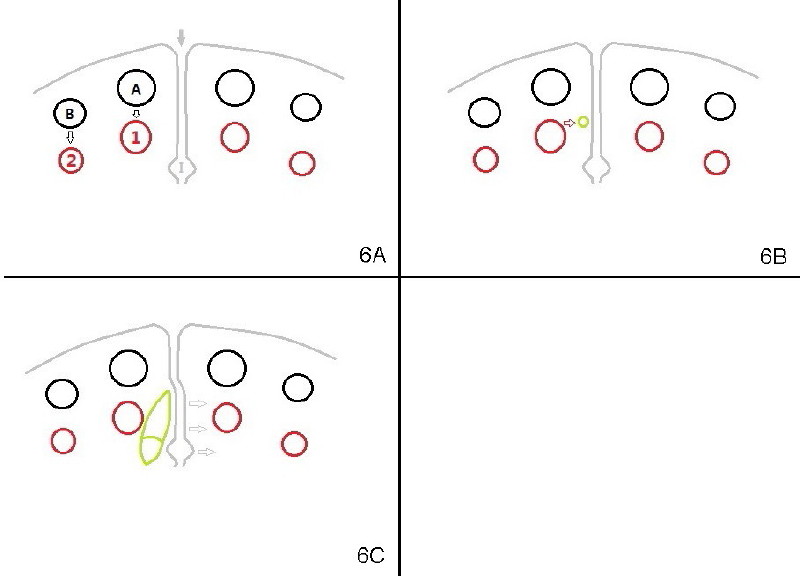
How does this happen? Here is a hypothesis. Fig.6A diagrammatically shows the developing premaxilla, which consists of the right and left portions, separated by the midline suture (solid arrow) and the incisal canal (I). As well-known, the developing deciduous incisor tooth buds (A, B) give rise palatally to permanent tooth buds (1,2), respectively (open arrows). For unknown reasons, the developing permanent central incisor tooth bud produces medially an extra tooth bud (mesiodens, green circle in Fig. 6B). The cortices of the developing midline suture appears to be a barrier for the developing mesiodens. Unlike deciduous or permanent teeth, the development mesiodens apparently does not have its definitive growth pattern (probably due to its absence of deciduous precursor). It may grow upward (Fig.1), downward (Fig.2) or palatally (Fig.4,6C) along suture cortex.
Xin Wei, DDS, PhD, MS 1st edition 12/16/2011, last revision 12/17/2011