



|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
Next |
Progressive Loading
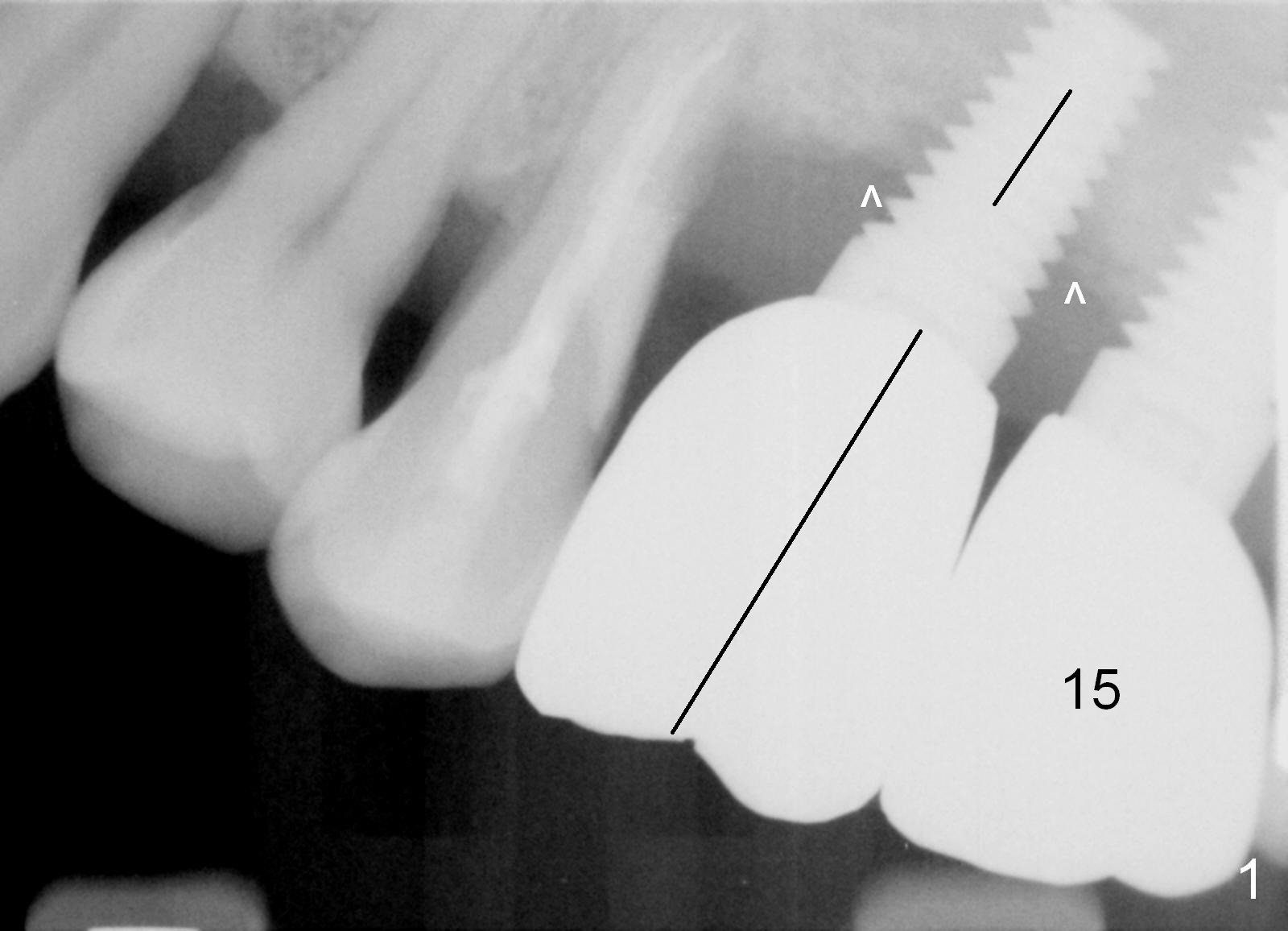
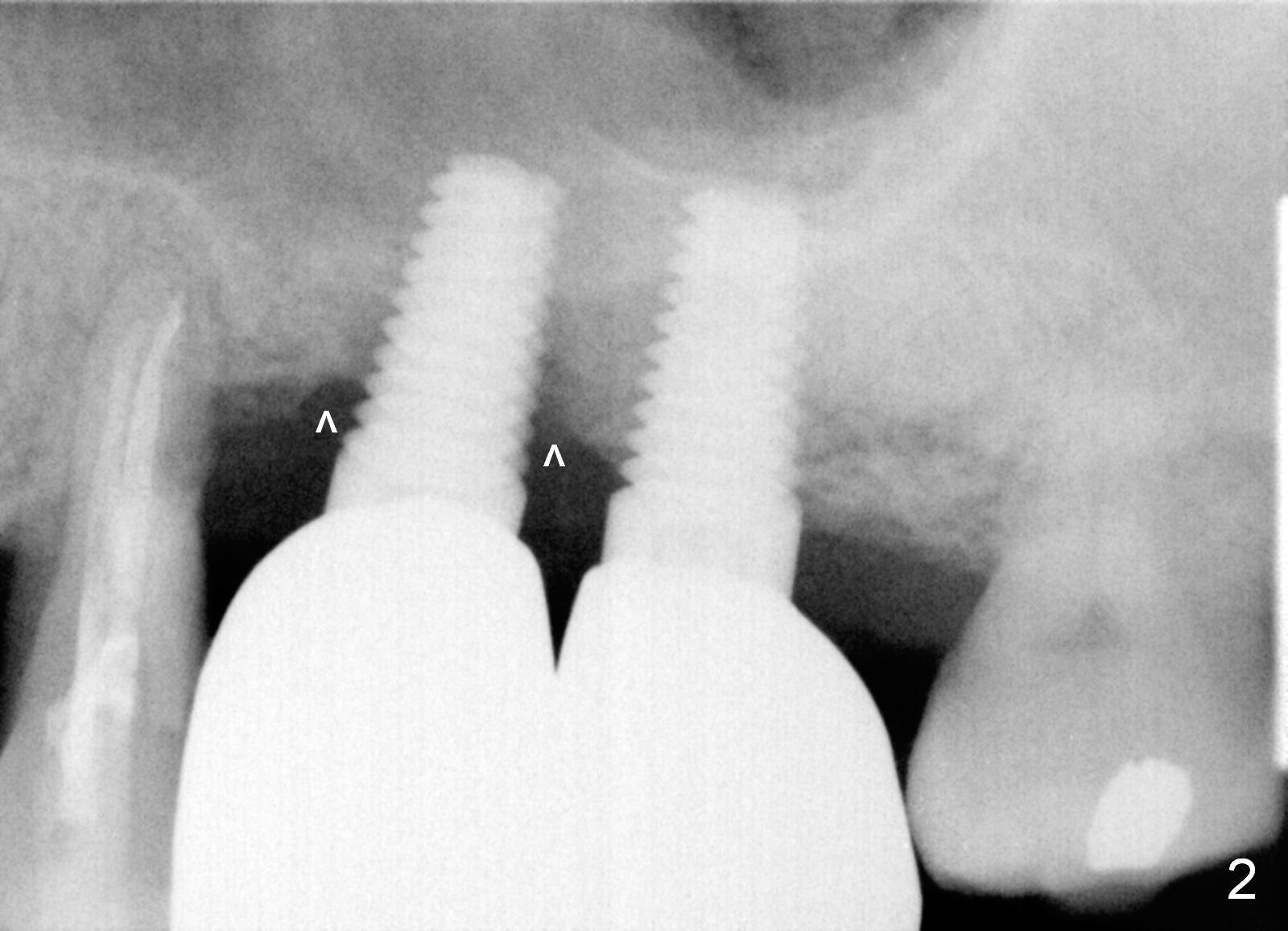
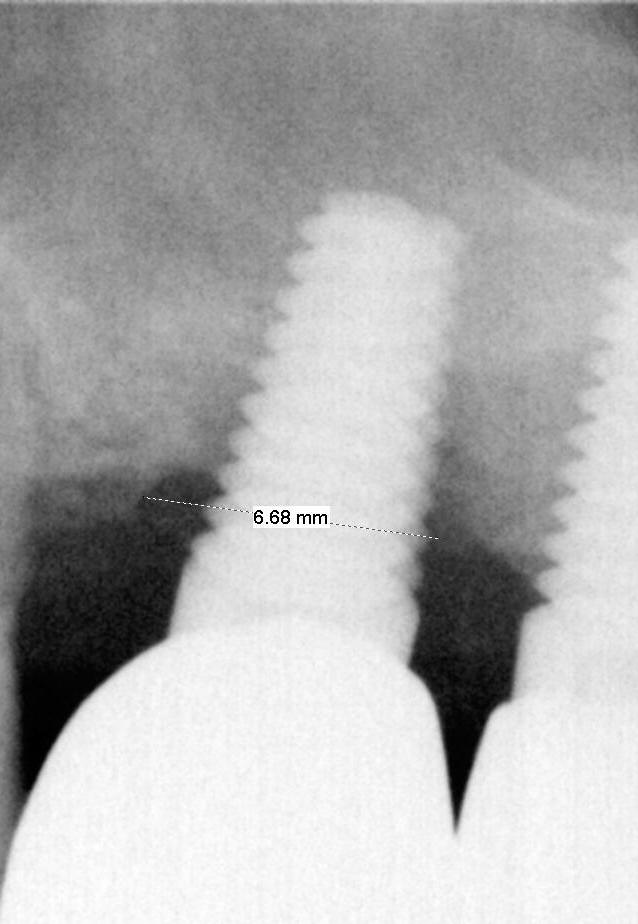
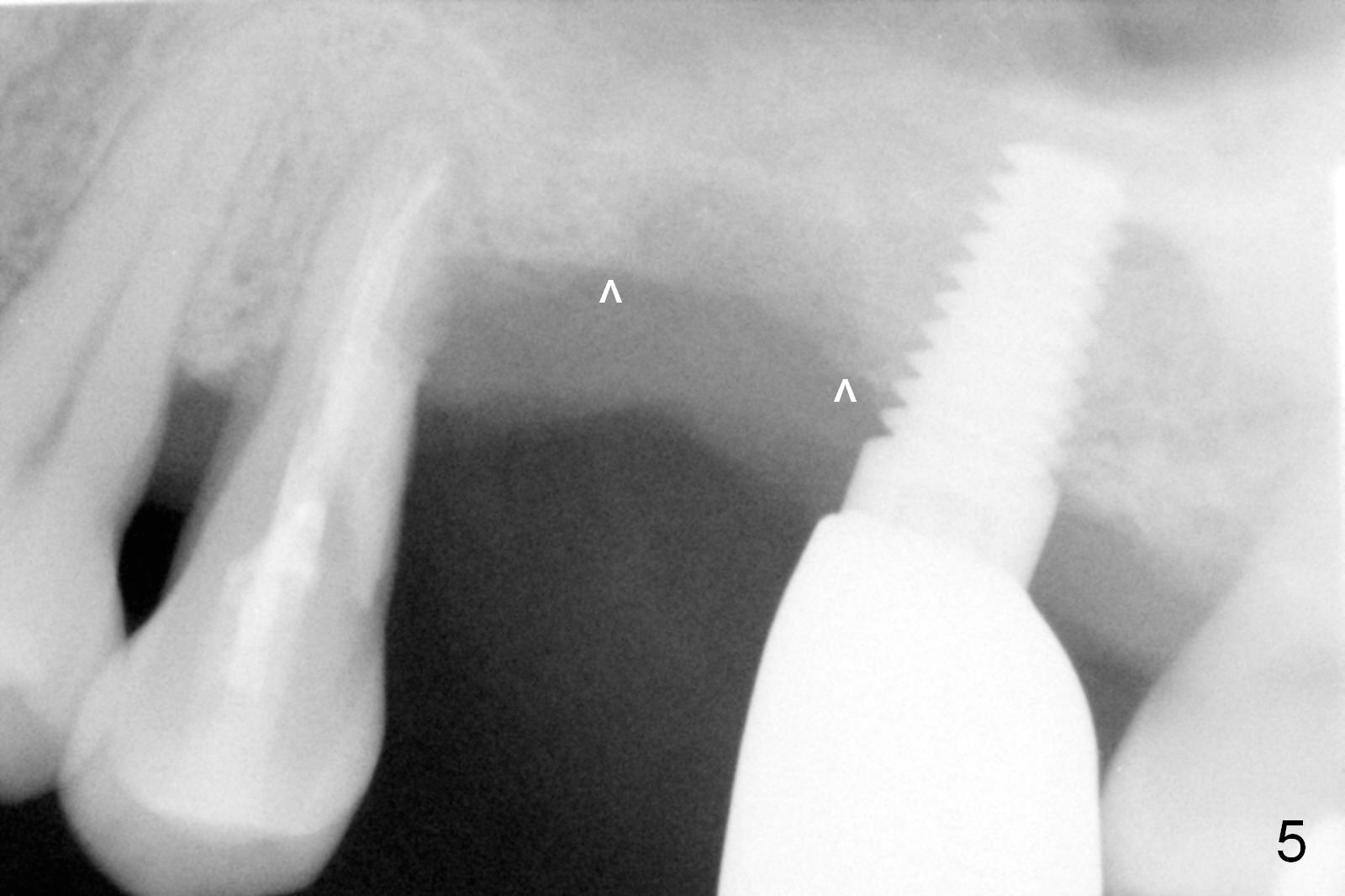
Three months post cementation, the crown at #14 is found to have mobility I with mild tenderness and bone loss (Fig.1,2 ^). The crown/implant ratio is unfavorable (Fig.1). The 1st option of treatment is to remove the crown and the unipost and place a healing screw if the gingiva is healthy. If the implant is fatally loose, remove it, explorer the osteotomy for wall integrity. If it is solid, place 5.5 or 6.0 mm tap (Fig.3) before placing an appropriate implant (e.g., 6x6 mm; allograft for internal sinus lift and coronally) and healing abutment for more than 6 months (vs. 4 months previously). When the implant seems to have osteointegrated, place a provisional from infraocclusion to ortho-occlusion over time (6 months, progressive loading). When the implant appears to withstand normal loading, fabricate a single-unit crown. If not, remove #15 crown and splint #14 and 15 crowns or #13 and 14 in case the tooth #13 fails (Fig.2 limited bone height).
In fact the implant and crown has been dislodged. Prepare PRF membrane to be inserted into sinus prior to bone graft.
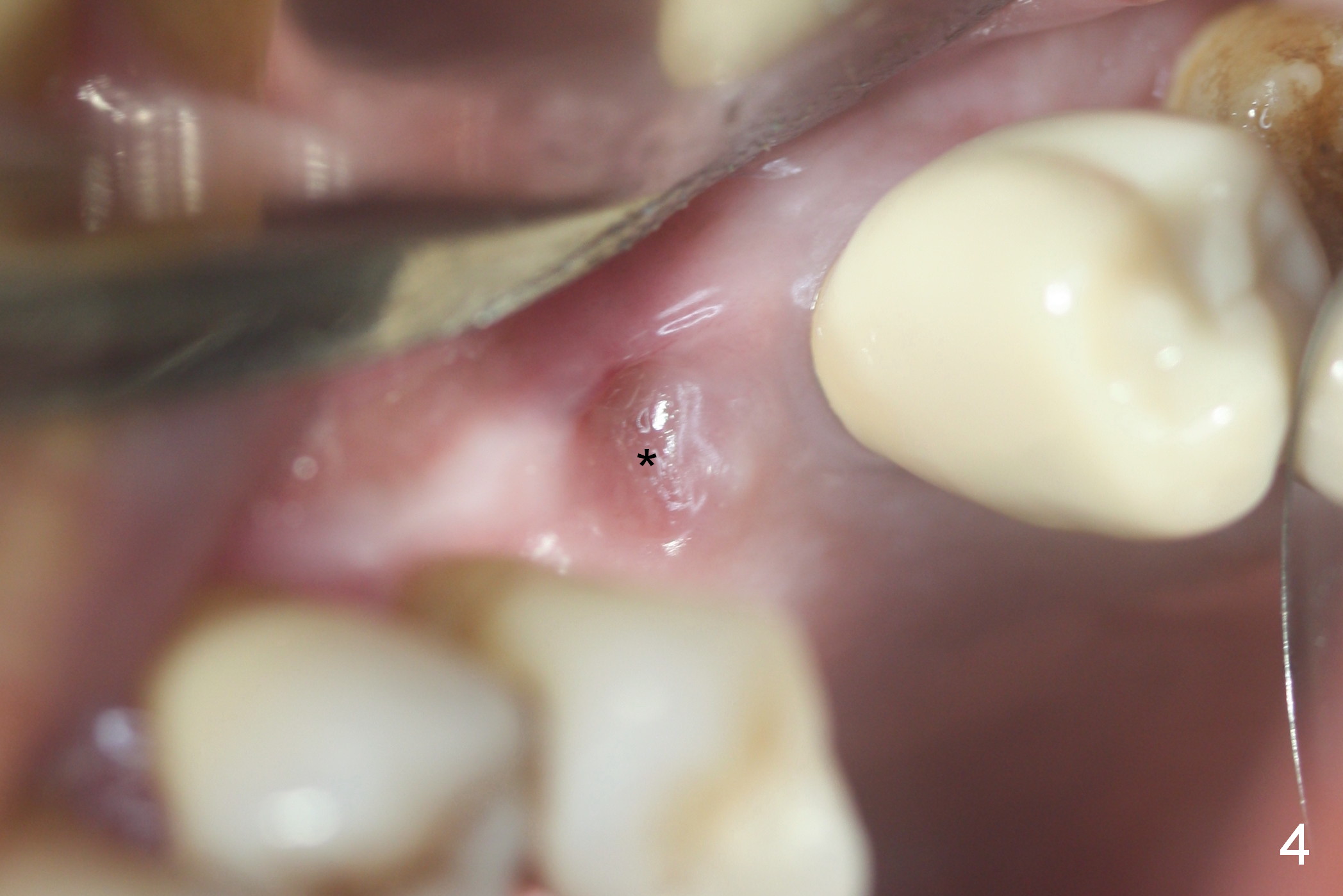
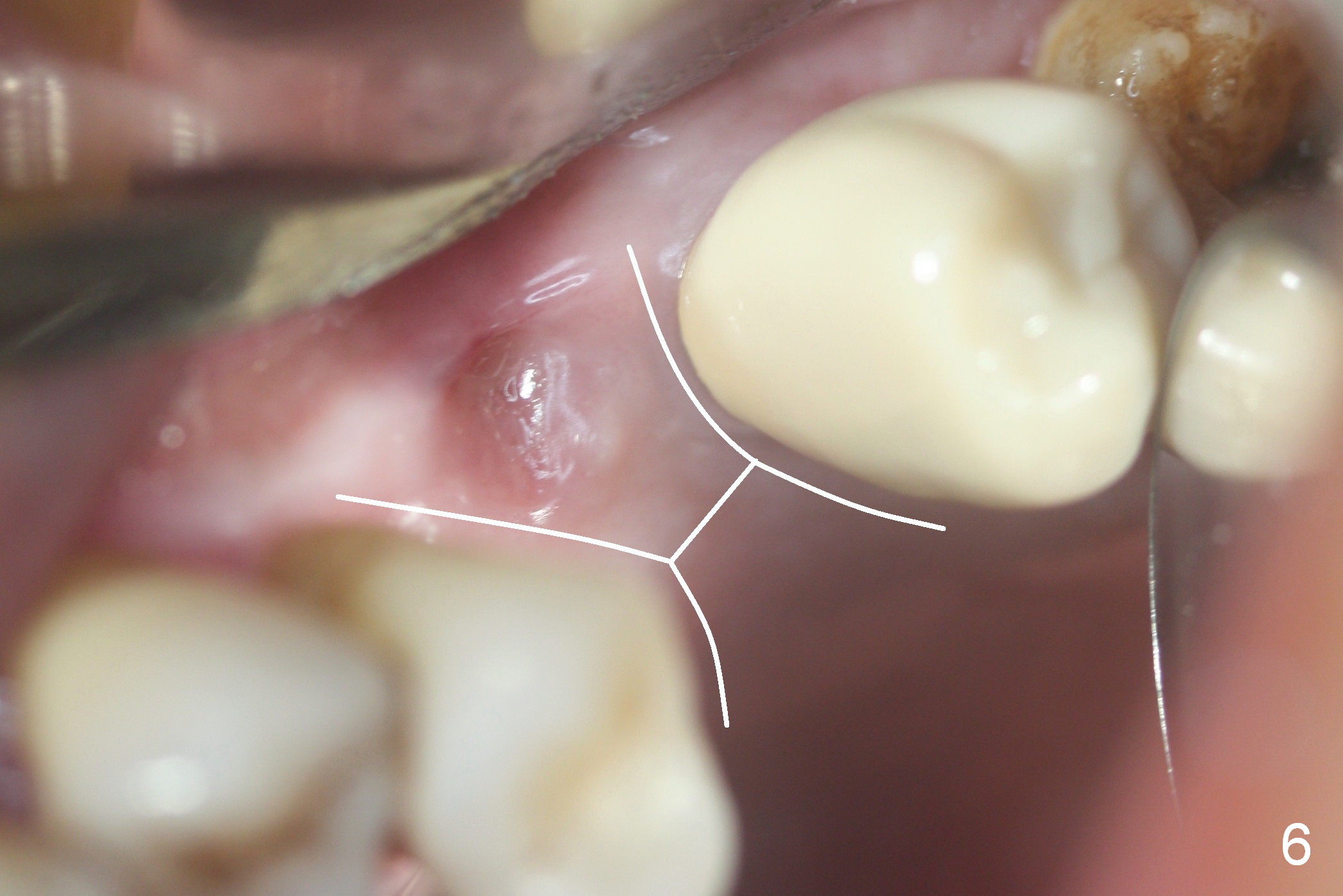
The implant site is healing a few days after loss (Fig.4 *) with a bony defect (Fig.5 ^). It appears that the implant at #14 was placed buccally. An incision is made palatally because of the presence of more keratinized gingiva (Fig.6). The buccal bone height is limited. The soft tissue in the bony defect is lifted into the sinus before bone graft (Fig.7 *).
Six months later, an implant will be placed as palatal as possible. Good news is that the patient agrees to receive orthodontic treatment. His concern is deviation of the upper dental midline to the right. It would be nice to move the tooth #13 distally. At least the mesiodistal dimension of the edentulous area will be reduced. Severe bone loss distal to the tooth #13 is concern for orthodontic movement.
Study of the dislodged implant/crown reveals that the latter covers the rough surface of the former (Fig.8-10, unfavorable crown/implant ratio). If orthodontics is not to be done, block graft should be done on the oral side of the alveolar bone to improve the crown/implant ratio. Or loading should be delayed, 7 months postop. Magic sinus kit will be used. On the right side, sinus lift is successful 2 years post cementation, where bone height is 5.8 mm.
Return to Sinus Graft Course 2 Xin Wei, DDS, PhD, MS 1st edition 06/25/2016, last revision 06/03/2018