



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
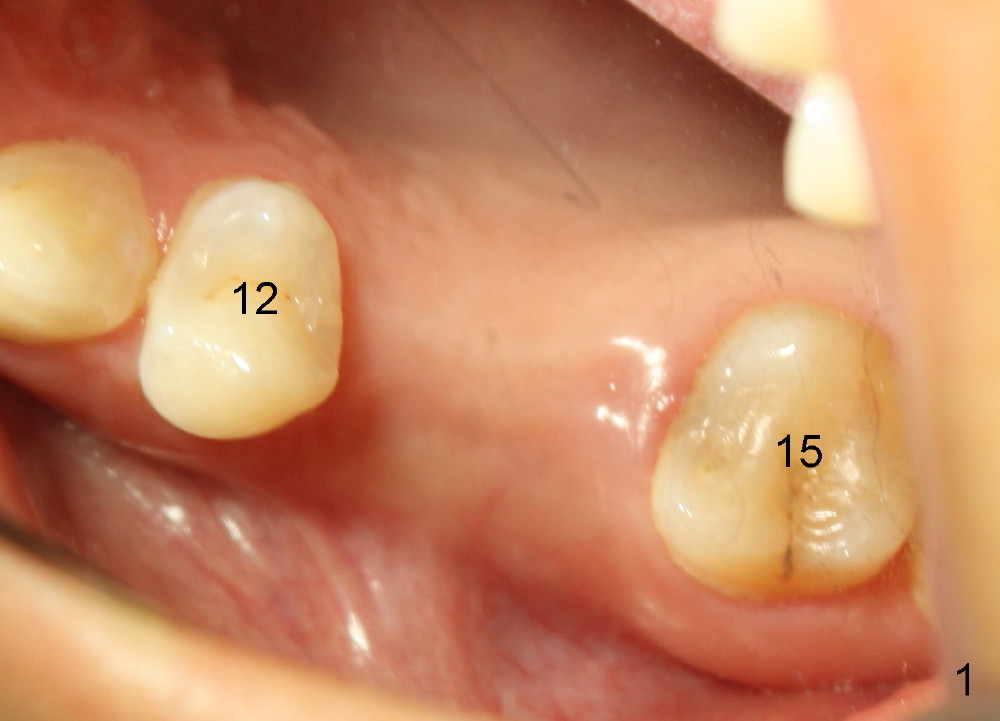
One Piece Implant for Sinus Lift
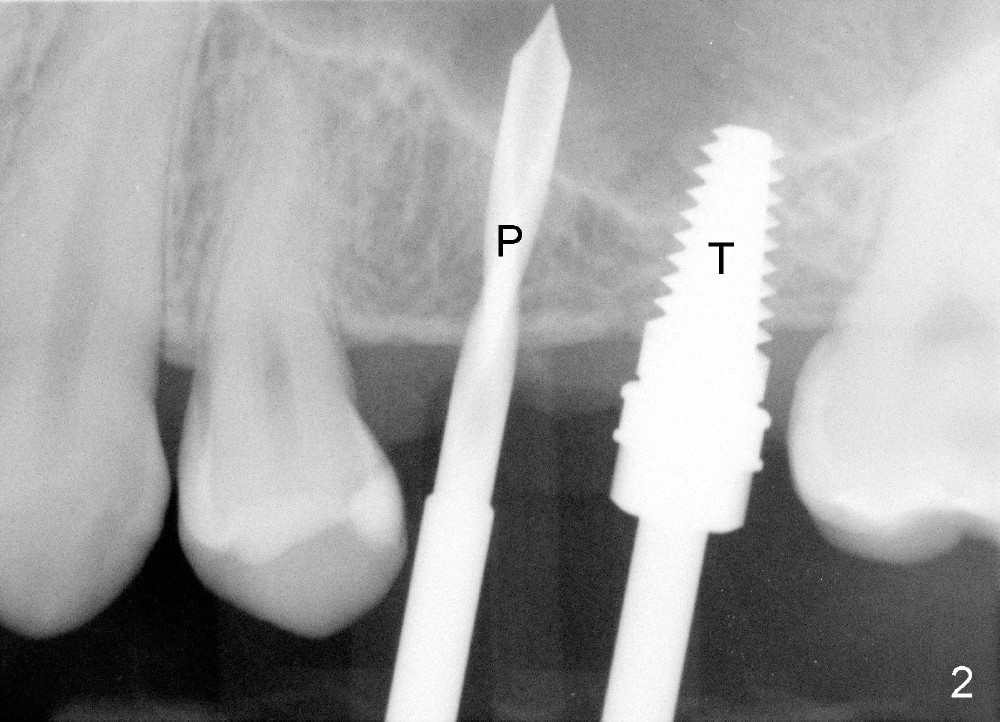
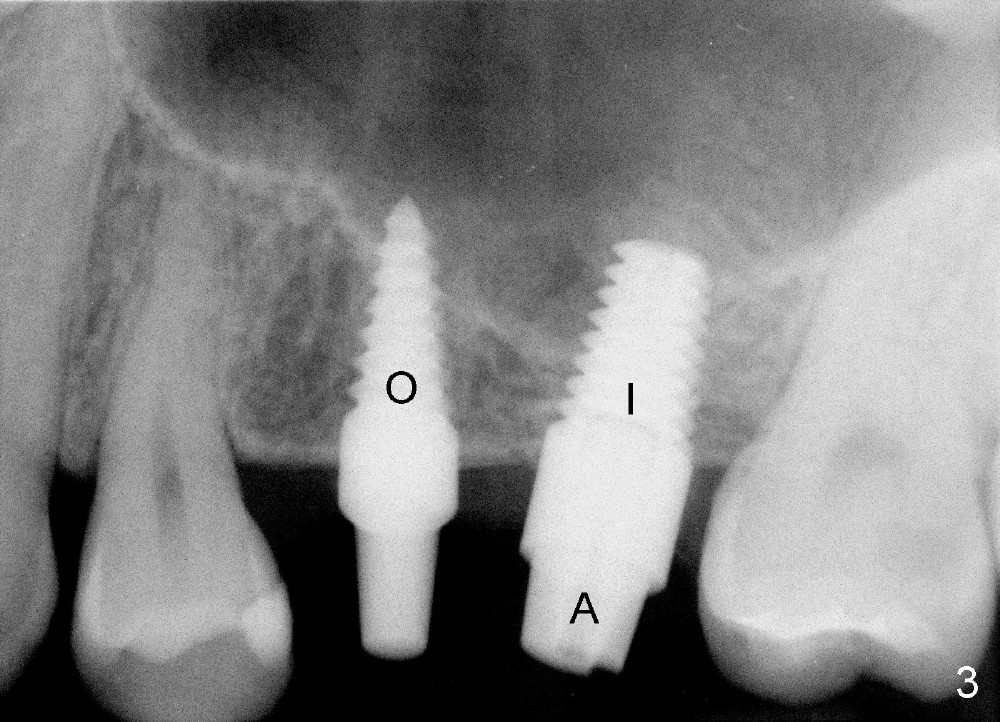
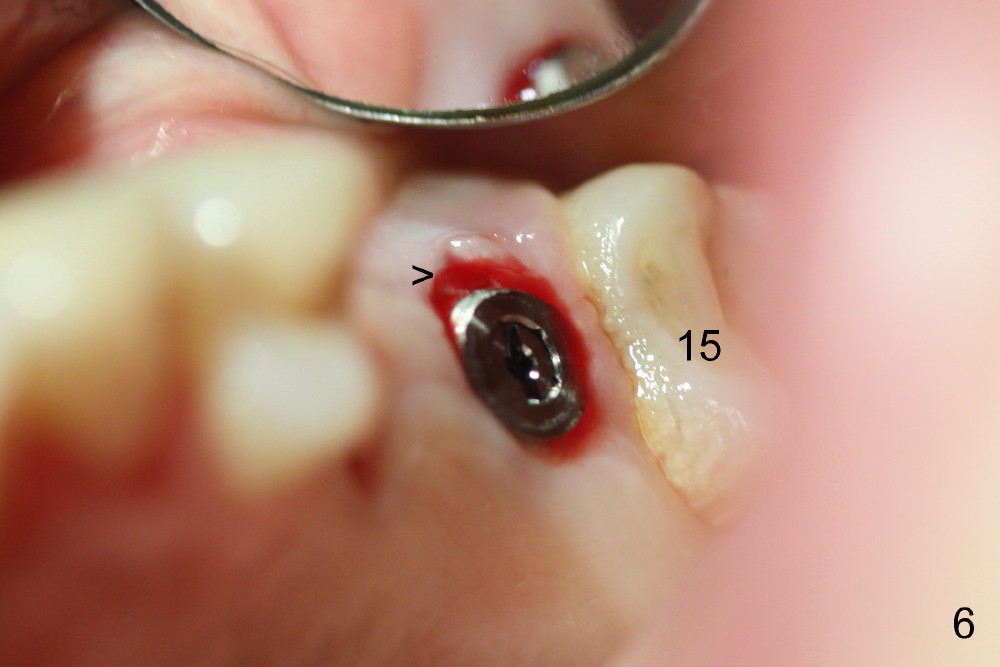
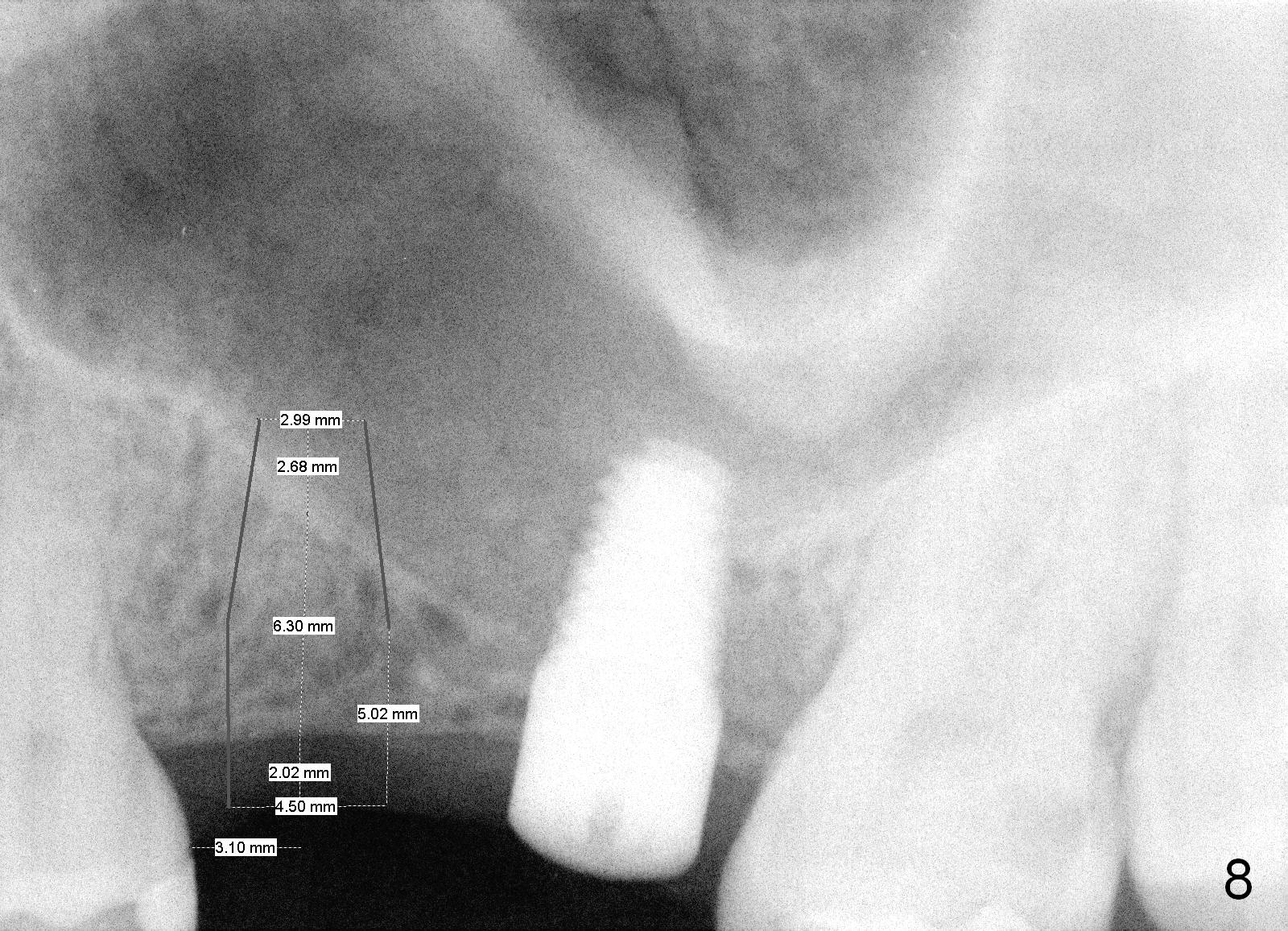
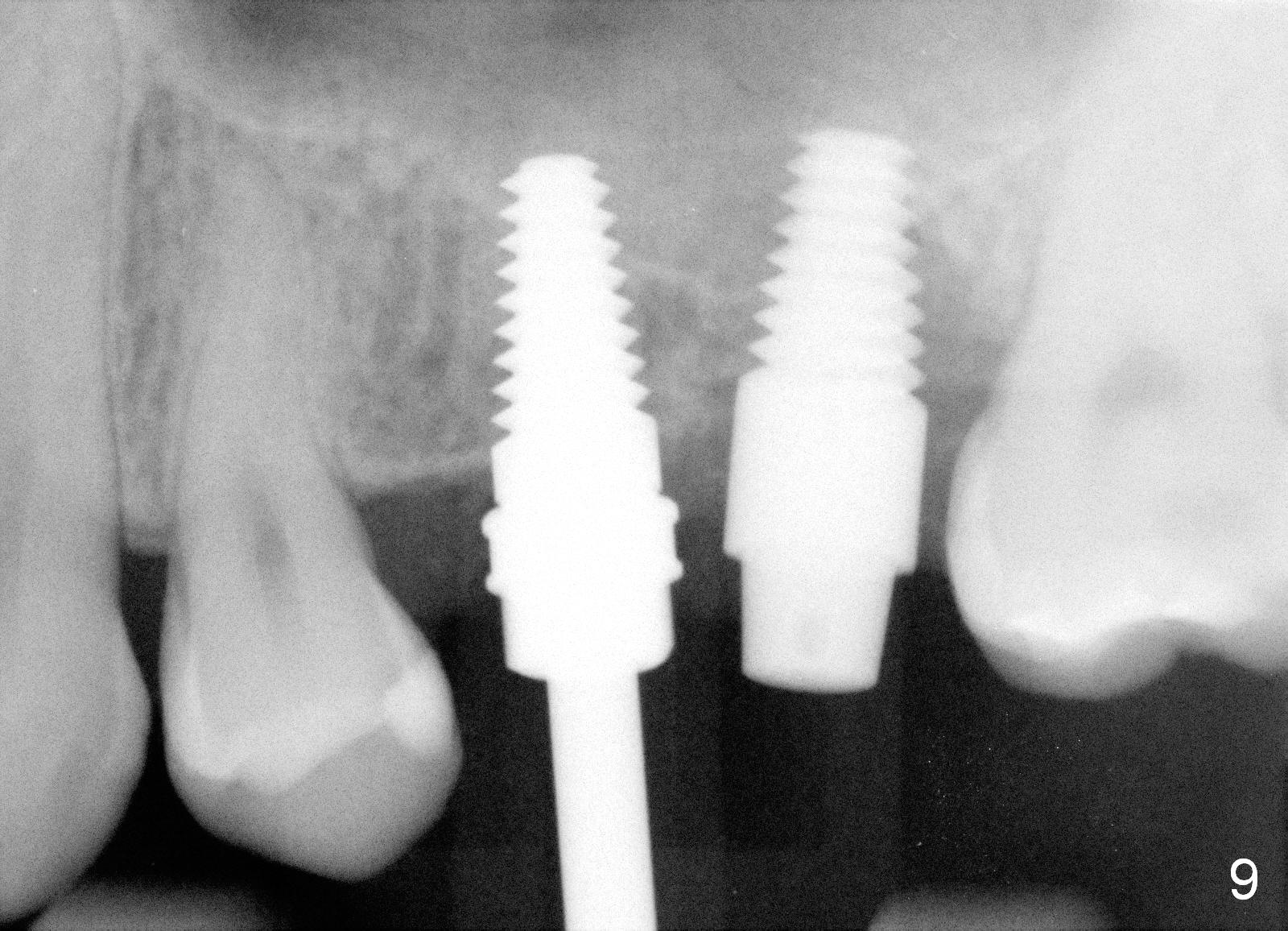
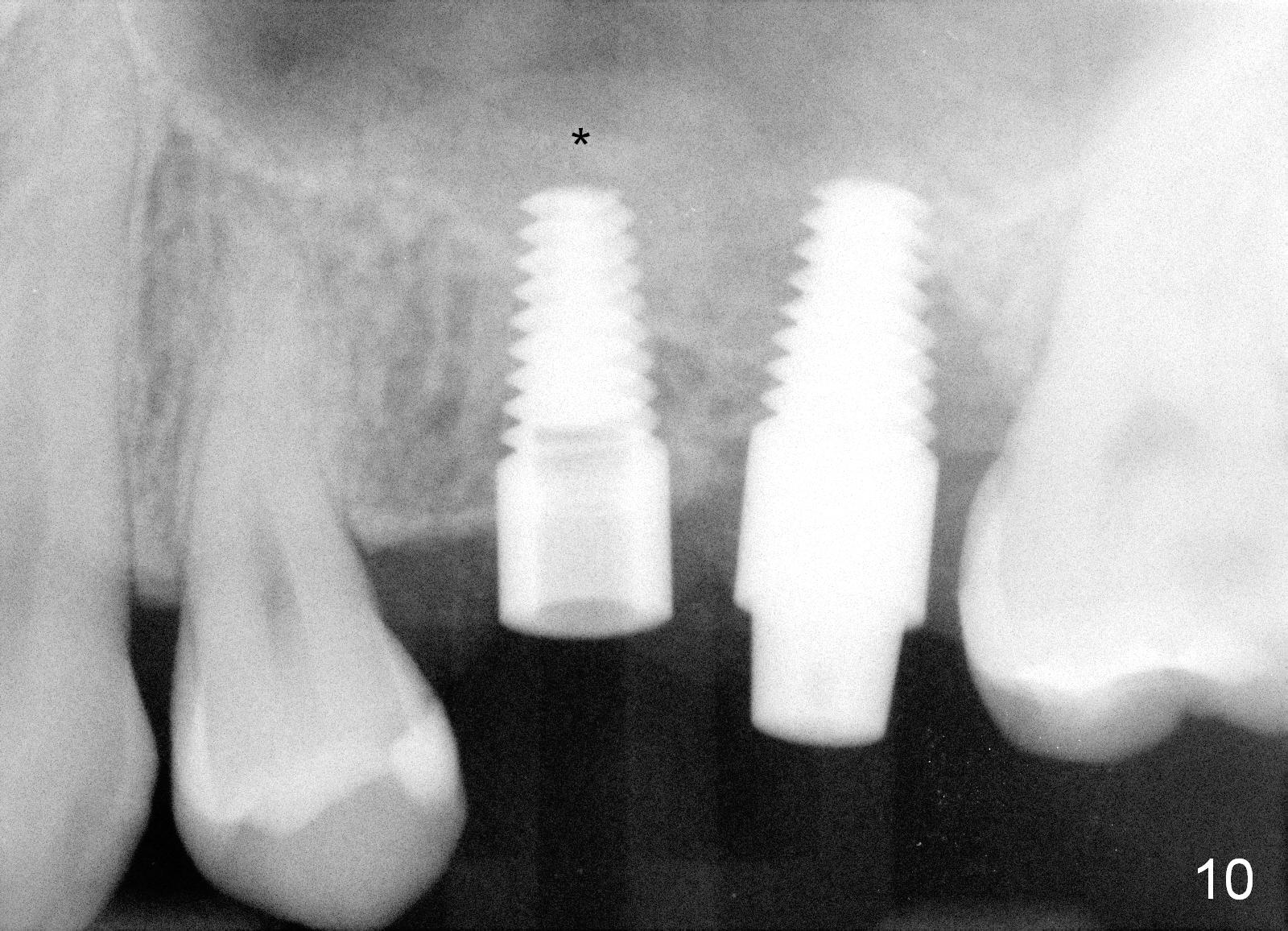
The patient returns for #13,14 implant placement. The ridge appears to be wide buccolingually (Fig.1 mirror view). A 4 mm tissue punch is used for access at the sites of #13 and 14. Osteotomy is initiated by using 3 mm trephine bur at the depth of 4 mm at both sites; 2 mm pilot drill is used to continue osteotomy at 8 mm deep at the site of #13. Sinus lift is accomplished by using tapered osteotomes 2,3 mm 6 mm deep, followed by 4.5x11 mm tap (Fig.2 T); 2 mm pilot drill (P) is reinserted into #13 osteotomy site with inadvertently penetrating the sinus floor. When the tap is removed from the site of #14, the sinus membrane is also found to be perforated. The sinus membrane at both sites is repaired by insertion of collagen dressing before bone graft. A 4x11 mm one-piece implant is placed at the site of #13 slowly hoping that it does not re-perforate the sinus membrane (Fig.3 O). Due to limited restorative height, the abutment portion of the one-piece is expected to be trimmed (Fig.4 O). In case of implant complication or failure, the implant may be difficult to be removed. Therefore the implant at the site of #14 is two piece one (Fig.4,5 I/A, 5x11 and 4x3 mm, respectively). The insertion torques for #13 and 14 are 35/40 and >60 Ncm. Immediate provisionals are canceled mainly because of patient's inability to open wide for long. Perio dressing is placed instead after adjustment of the height of the abutments. The patient experiences one episode of light nasal hemorrhage a few hours postop. Although the patient takes Amoxicillin for 1 week periop, the implant at the site of #13 dislodges 1 months postop (Fig.5). Immediate re-placement with a larger 2 piece one is canceled because of mild infection mesiobuccal to the implant at the site of #14 (Fig.6 >). Exploration around the latter implant reveals possible thread exposure in a small area. After copious irrigation with normal saline, Arestin is placed. Two months post exfoliation, the site is re-entered (Fig.7,8). There is a lingual defect. Osteotomy is initiated as buccal as possible. A 4.5x11 mm tapered tap penetrates the sinus floor without tearing the membrane (Fig.9). The same-sized implant is placed (25/30 Ncm) with sinus lift (Fig.10 *). The lingual defect is bone grafted. There is dehiscence lingually 7 days postop (Fig.11). Impression for final restoration is taken 1.5 months postop because of pending wedding. The crown has been in function for 2.5 months.
It appears that there is no problem for the pointed end of 1 piece implant to stick to the sinus. A critical step is to place the implant inside the alveolus with primary stability. Tissue punch does not provide good surgical exposure to the ridge.
Return to Preparation for
Sinus Lift,
Instrument,
Implant Fails
Xin Wei, DDS, PhD, MS 1st edition 11/16/2014, last revision 06/22/2015