


,%20graft%20after%20abutment.jpg)







|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
||||
Clearance between Immediate Implant and Partial Denture
It is acceptable practice to have occlusal clearance for immediate implant and immediate provisional. Without proper clearance, a partial denture may cause failure of an immediate implant and provisional. Putting on and taking off the denture and chewing with it may cause micro-movement of the implant.
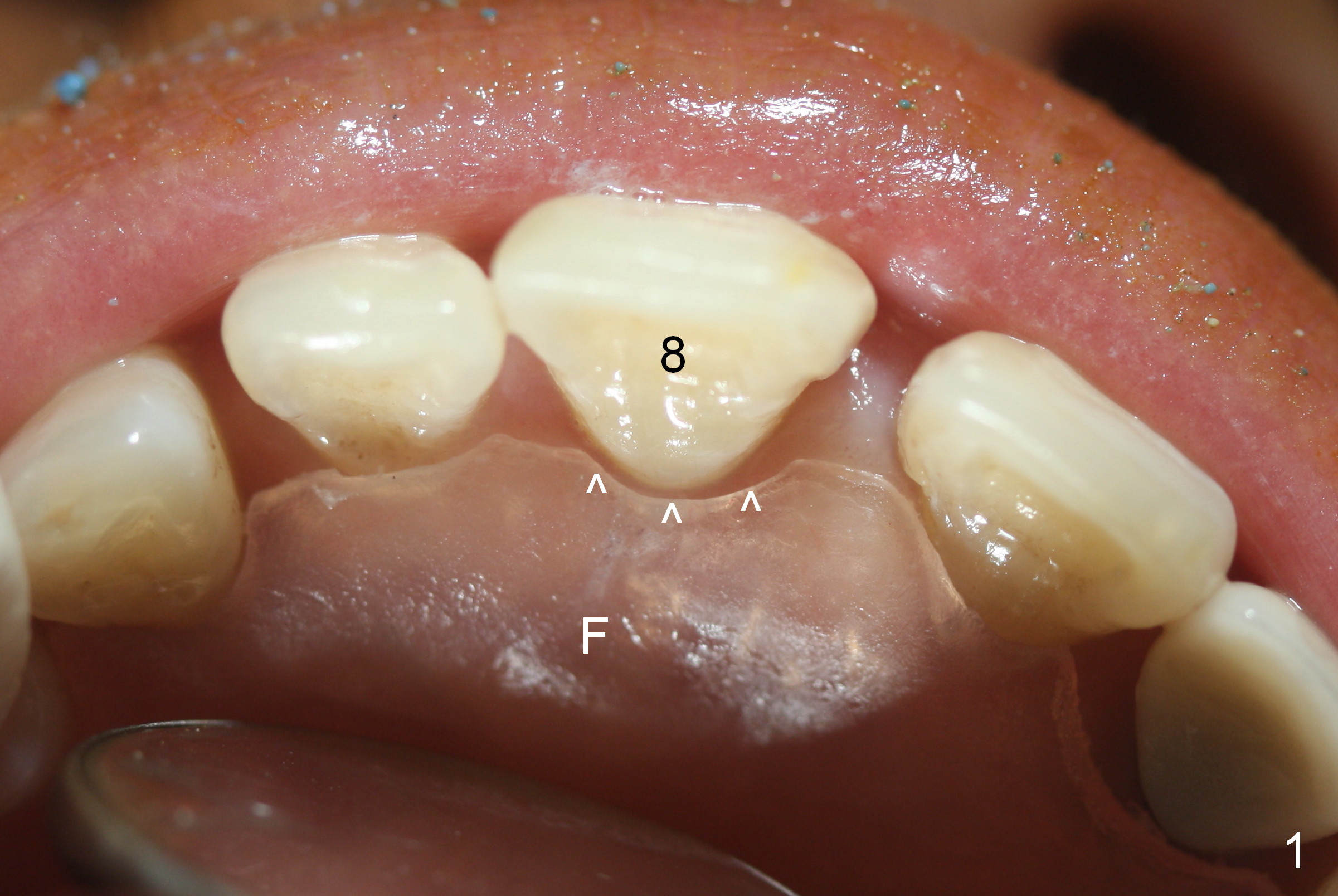
Mrs. Cheng has an upper flipper to replace four missing molars (Fig.1 F). Due to loss of posterior support, the tooth #8 has shifted distobuccally (Fig.2 arrow) as well as incisally. She requests implant treatment for cosmetics. When an immediate provisional is fabricated to correct shifting, it will most likely contact the flipper. Providing clearance (Fig.1,8 arrowheads) is critical.
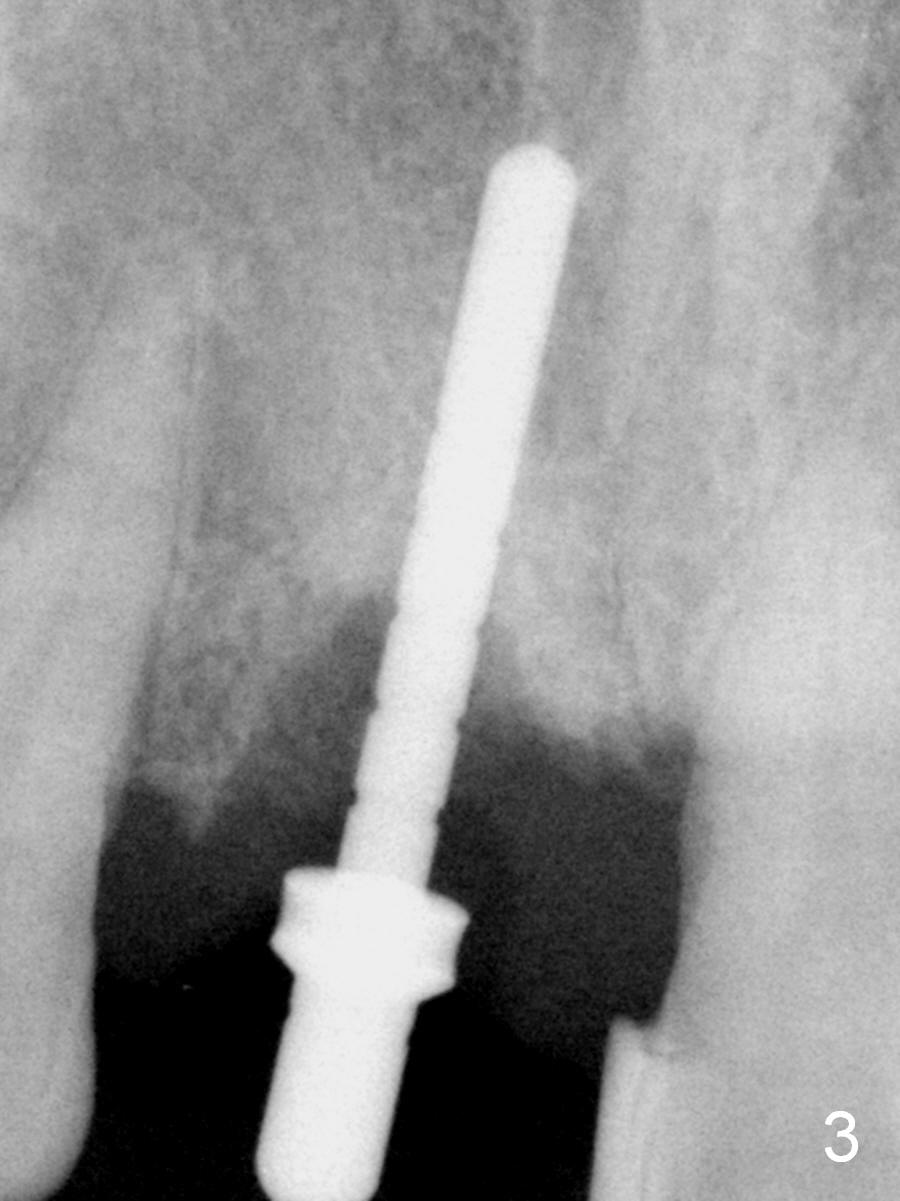
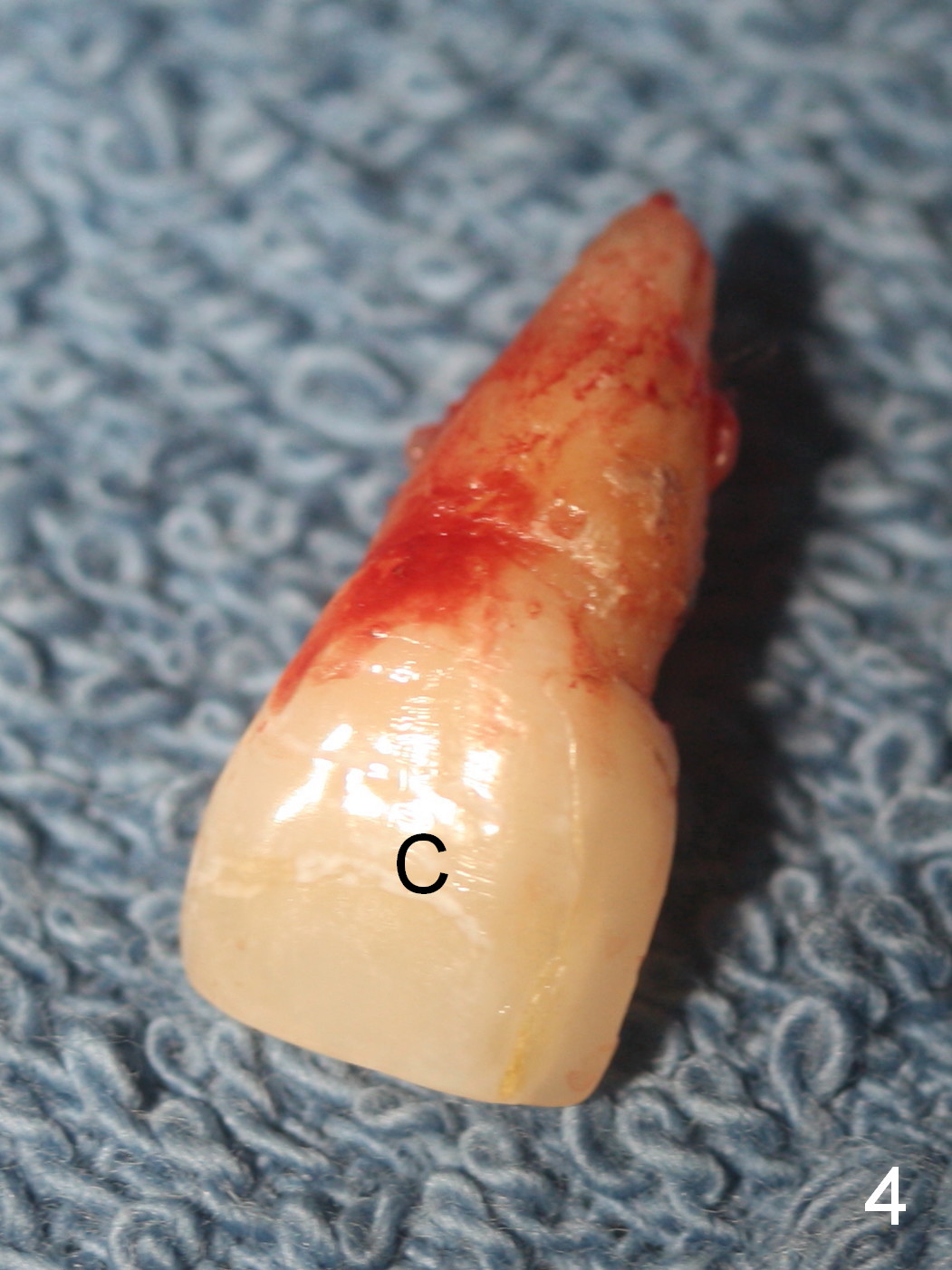
When the affected tooth is extracted (Fig.3), the palatal wall of the socket is found to be unexpectedly low and the buccopalatal width of the socket is seemingly limited. A narrow bone-level implant (3.8x13 mm) and a wide abutment (5.5x5.5(4) mm) are contemplated. In addition, the crown of the extracted tooth will be shelled as an immediate provisional (Fig.4 C).
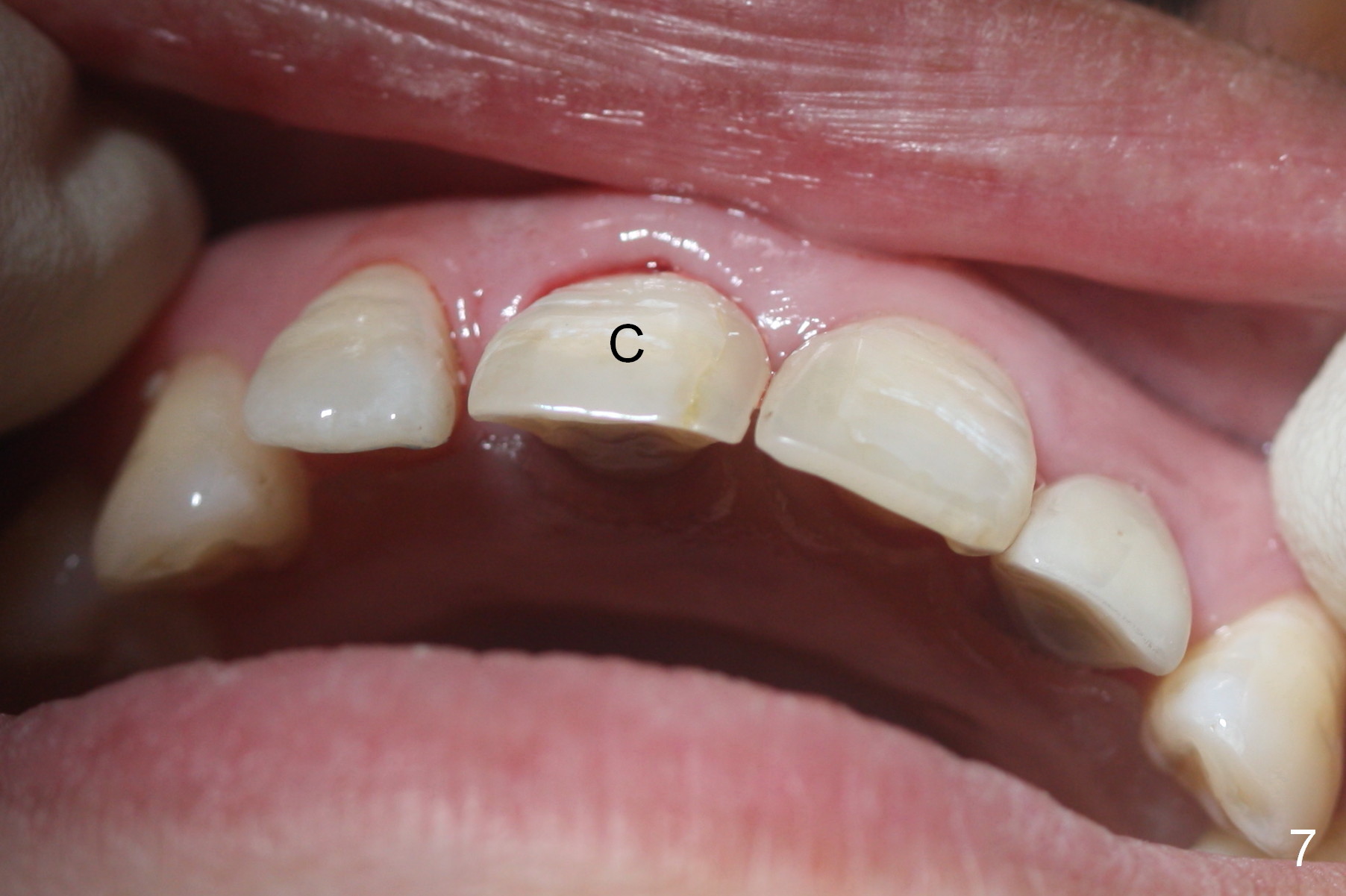
After the abutment is placed (Fig.5) and modified, the crown is tried in, relined with Jet acrylic and cemented (Fig.6,7). The latter maintains the gingival architecture (Fig.6) and restores the normal arch form (Fig.7). Most importantly, the flipper has been adjusted so that there is clearance (Fig.8 arrowheads). Immediately postop PA shows mineralized cancellous and cortical allograft (.5-1 mm) apical to the abutment (Fig.9 *).
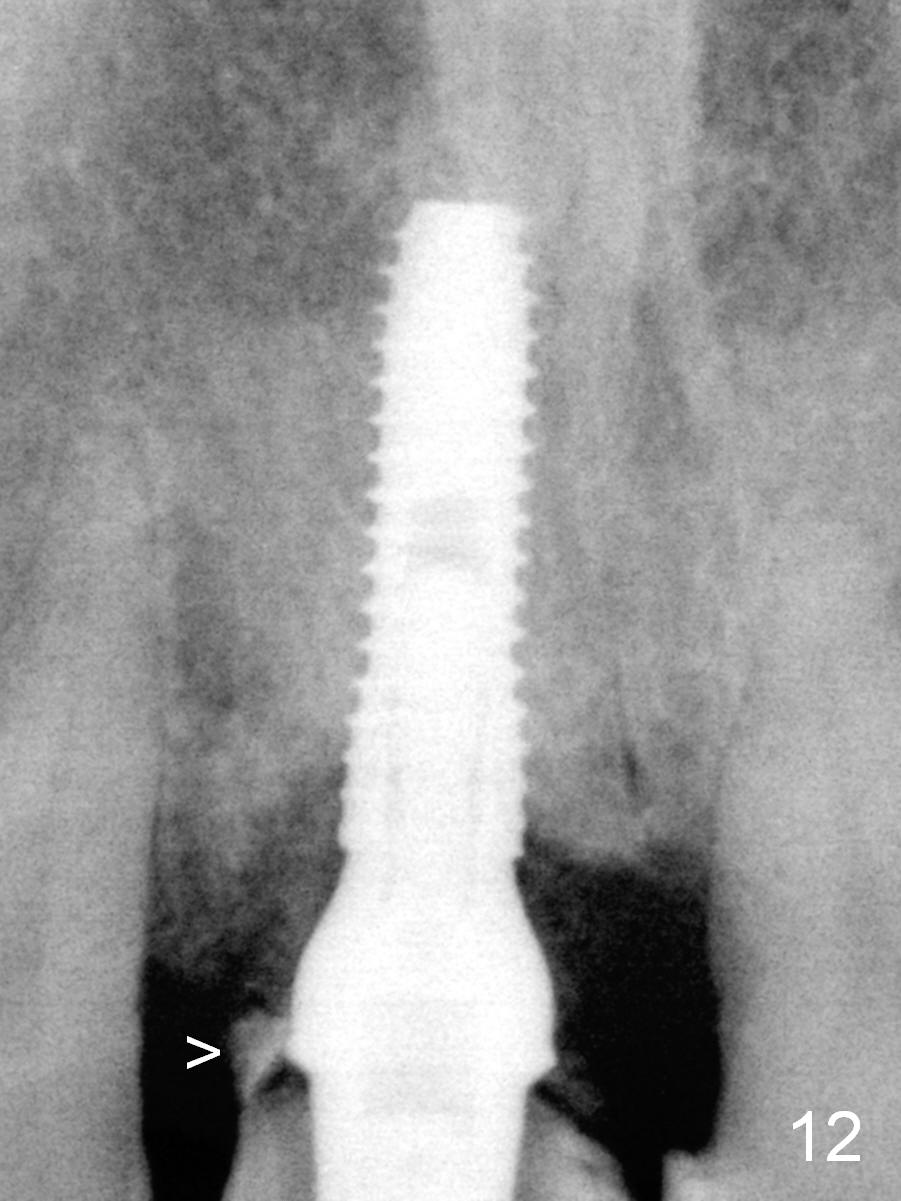
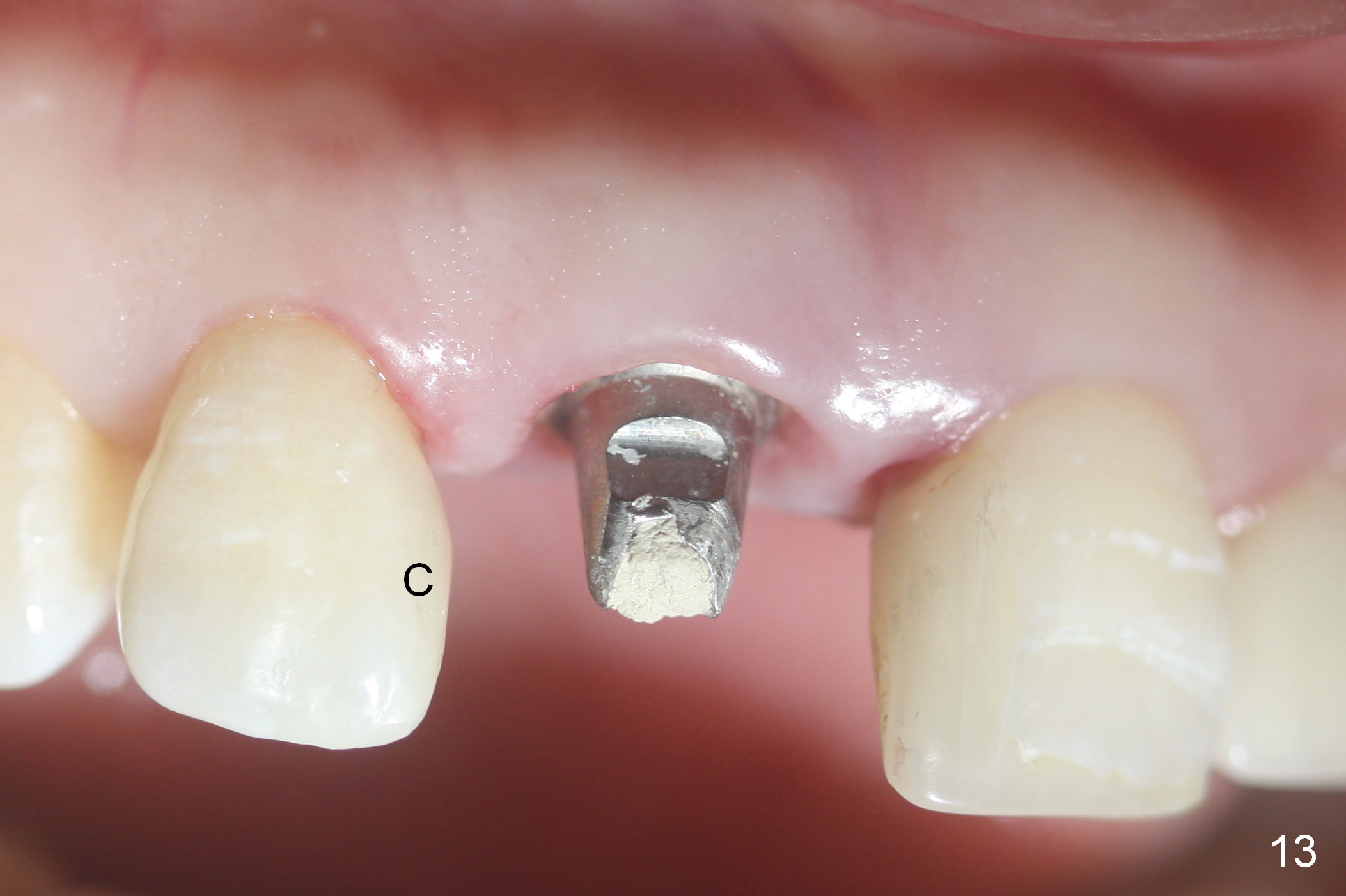
Eight days postop, the gingiva reacts to the natural crown normally (Fig.10,11). The crown shell remains in place, although fractured in the mesial margin (Fig.12 >) 2.5 months postop. Three months postop, composite is added to the mesial surface of the tooth #7 before impression for #8 (Fig.13 C; Fig.14 (illustration) brown line). Please increase the distal cervical width of the new crown at fabrication (Fig.14 blue line) to close the diastema between #7 and 8 as much as possible. Fig.15 shows A3, although the patient prefers B2 (the same shade for #10, Fig.14).
The patient is pleased with the closure of the diastema between the right central and lateral incisors when a crown is cemented for the former (Fig.16-18, as compared to Fig.2), although metal (Fig.13) shows through the Zirconia crowns at #8 and 10 (cervical area, Fig.16). It appears that a gold coated cemented abutment is required for upper anterior restoration (as posterior as the 1st bicuspid).
Return to Upper Incisor Immediate Implant,
Technicians
Xin Wei, DDS, PhD, MS 1st edition 03/10/2016, last revision 11/14/2018