|
|
|
|
|
Palatal Entry, Oblique Trajectory for Anterior Delayed Implants
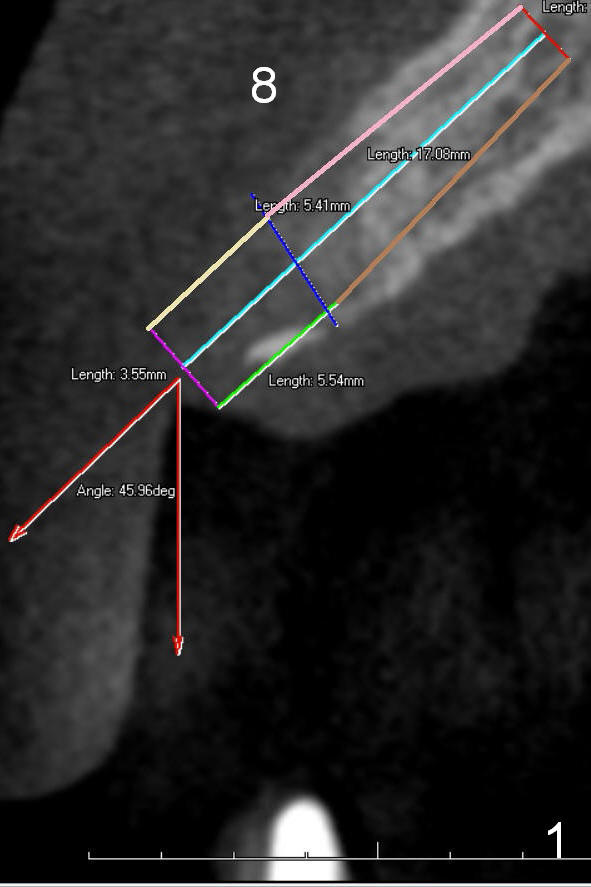
A 74-year-old man has chronic periodontitis. The teeth #8 and 9 were extracted ~ 6 months ago. The edentulous area is replaced by a flipper. The ridge is 5-6 mm wide. The smallest 2 piece tissue-level implant is 3.5 mm. When a 3.5x17 implant is placed, it has to be placed along the long axis of the ridge (Fig.1, CT coronal section at the site of #8). It causes the abutment to be too labial; angle of the abutment has to be 45°. The maximum angle of 3 mm abutment is 20°.
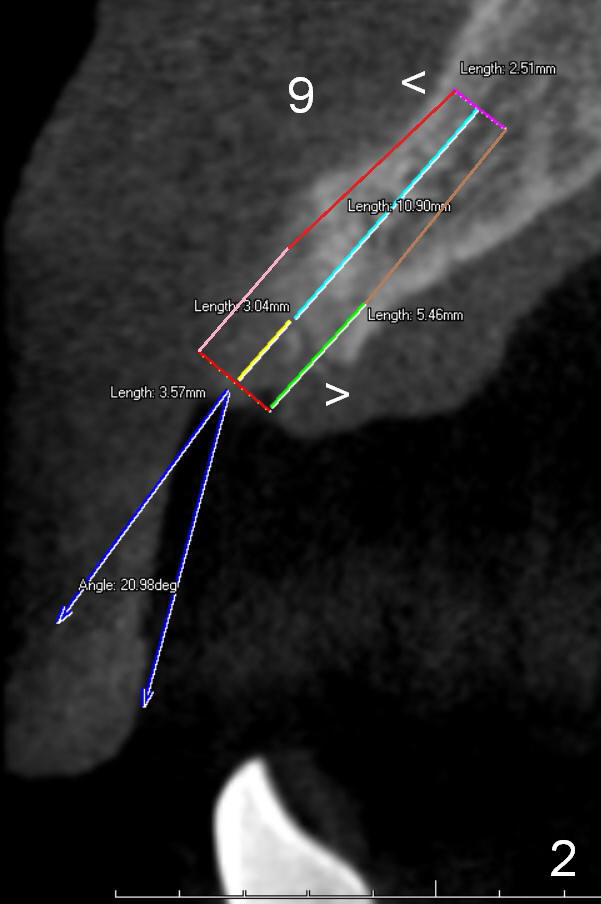
If a shorter implant is placed (3.5x14 mm, Fig.2 at the site of #9), the trajectory could be oblique. That is, the apical end of the implant is close to the labial plate (upper arrowhead: <), whereas the coronal end close to the palatal plate (lower arrowhead: >). The end result is that the angled abutment could be 20°.
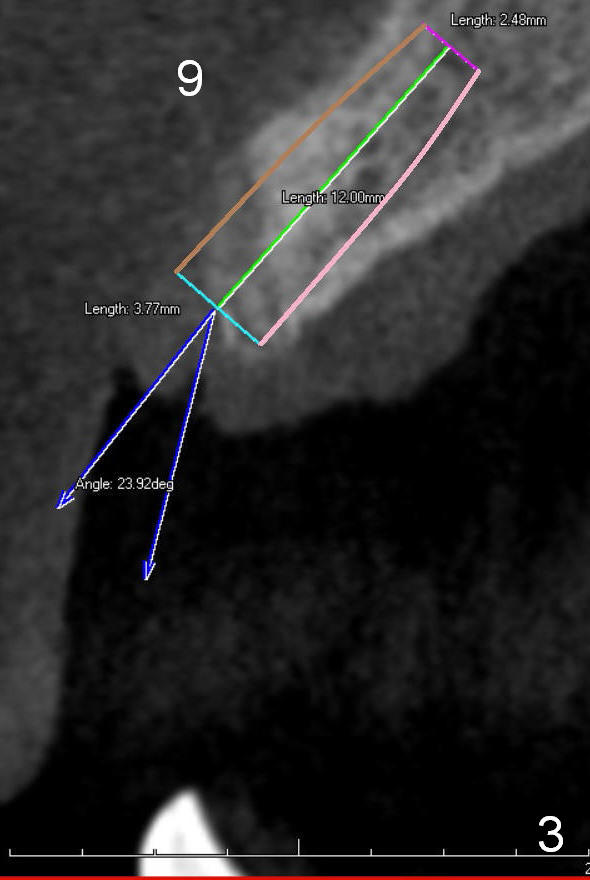
The smallest 2 piece bone-level implant available is 3.8 mm. It may be too wide for the ridge (Fig.3). The advantage of it is that there are two types of angled abutments: 15 and 25°.
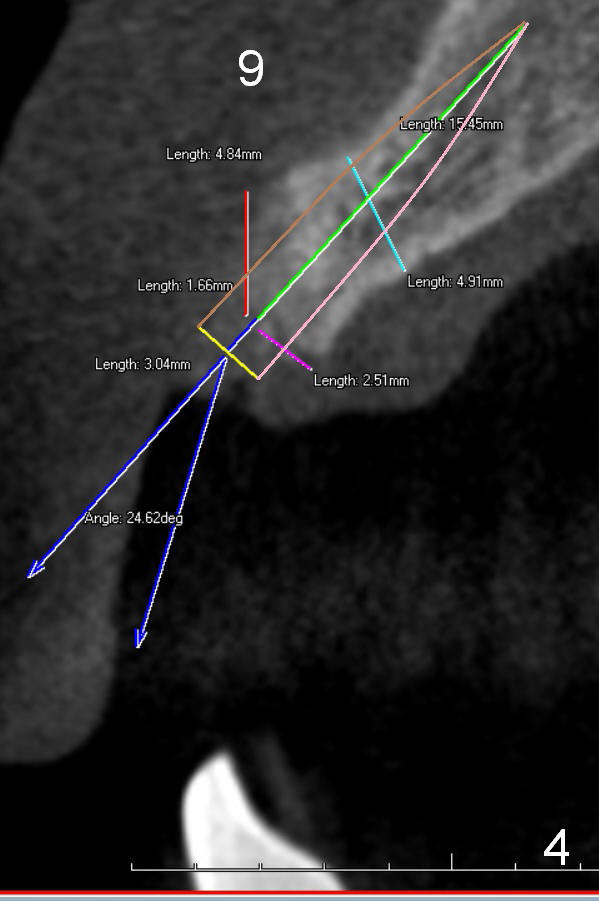
One piece angled implant (3x14 or x17, 15°) appears to be the best option (Fig.4). For the better vision, an incision will be made, preferably palatally. Osteotomy is also initiated palatally (2:1 ratio). The starting pilot drill will be 1.2 or 1.5 the whole length 17 mm. If perforation of the labial apical plate occurs or is anticipated, a shorter length is used (14 mm). The 2nd pilot drill is 2 mm, half of the length. A 3 mm drill is used to open up the crest so that when a 1 piece implant is placed, it will not cause crestal bone crack and reduce the chance of postop bone resorption.
Take Alginate impression prior to #8,9 implant placement for #30 and 31 surgical stent.
Return to Upper Incisor Immediate
Implant
Xin Wei, DDS, PhD, MS 1st edition 02/22/2015, last revision 02/22/2015