
|
|
|
|
|
|
|
|
|
|
|
|
Modified Palatal Placement
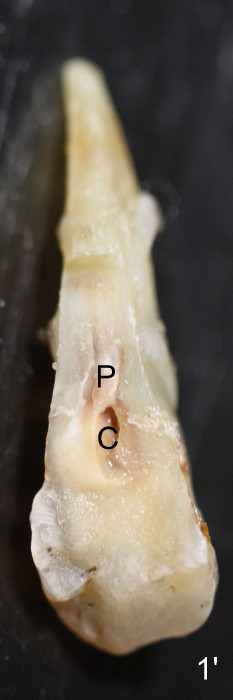
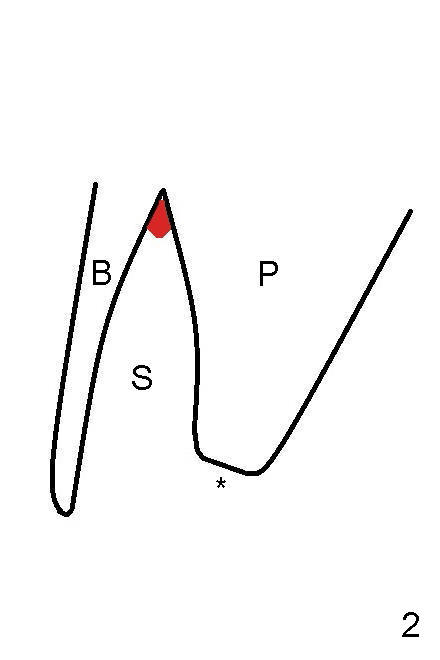
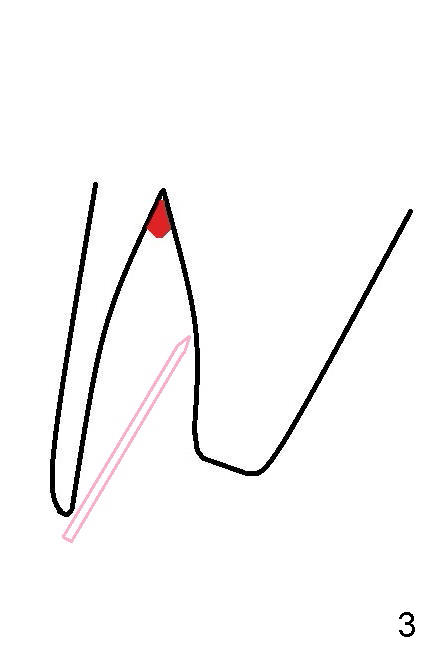
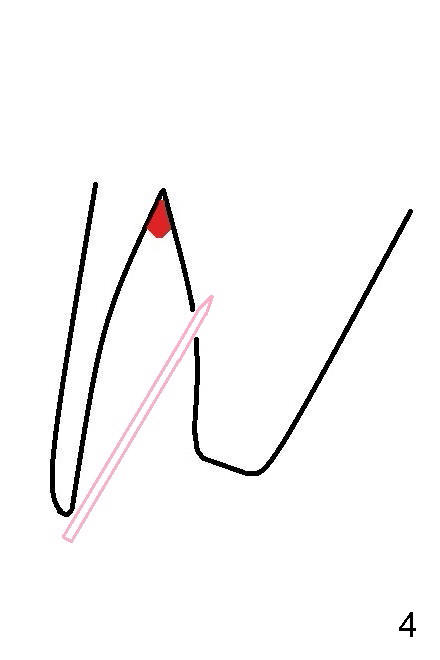
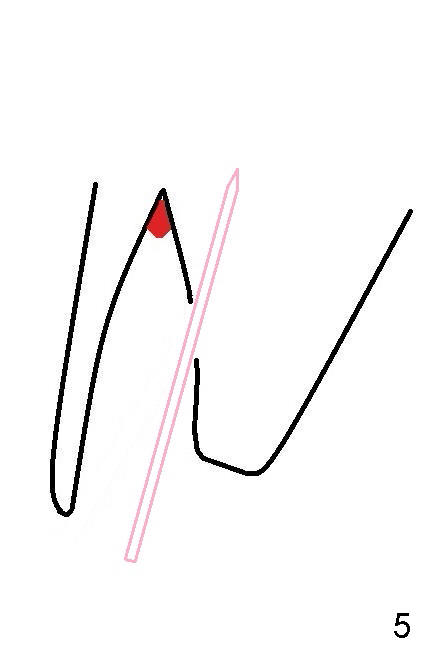
The extracted root is cone-shaped (Fig.1 (distal view),1' (lingual view)). The socket (Fig.2 S) is narrow bucco (B) -palatally (P). Osteotomy is planned in the middle palatal wall of the socket (Fig.3 pink). Once the smallest pilot drill penetrates the cortex of the palatal wall (Fig.4), the trajectory is changed while the depth of the osteotomy is increasing (Fig.5).
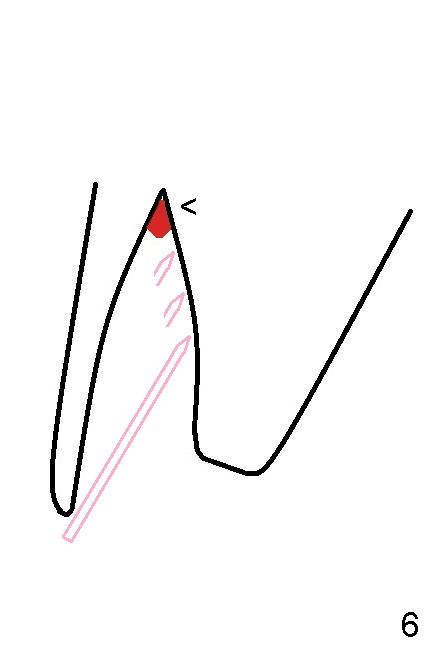
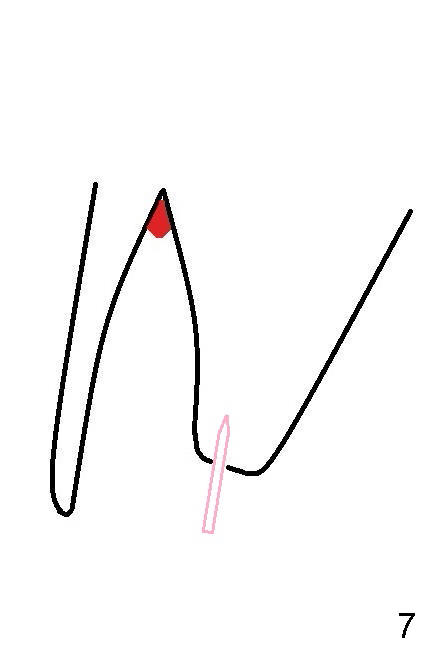
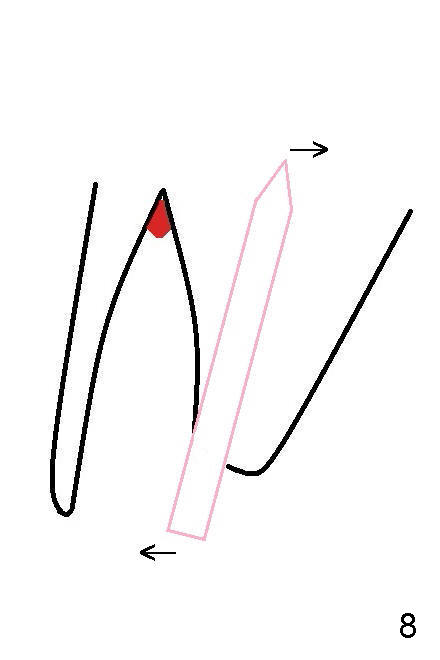
However, the plan does not work in this case. The pilot drill keeps slipping along the sloped palatal wall (Fig.6 pink drill bit tips) toward the infected apex (red), causing severe pain in spite of addition of anesthetics. The osteotomy has to be changed to the palatal plateau (Fig.2 *). The plateau is supposedly formed apical to the palatal crest. Since the plateau is relatively flat, penetration is easy (Fig.7). The drawback is that it is palatal. As drills increase in diameter and go deep, the coronal end of the drills is pushed buccally, while the apical end palatally. The final osteotomy is more or less in the center of the socket with 2-3 mm buccal gap.
Return to Upper Bicuspid Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/21/2014, last revision 01/19/2018