





|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Palatally Placed Tapered Implant in Upper 2nd Premolar
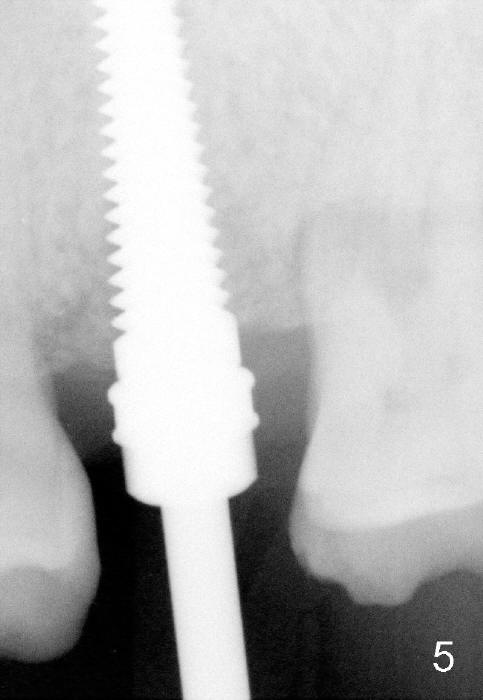
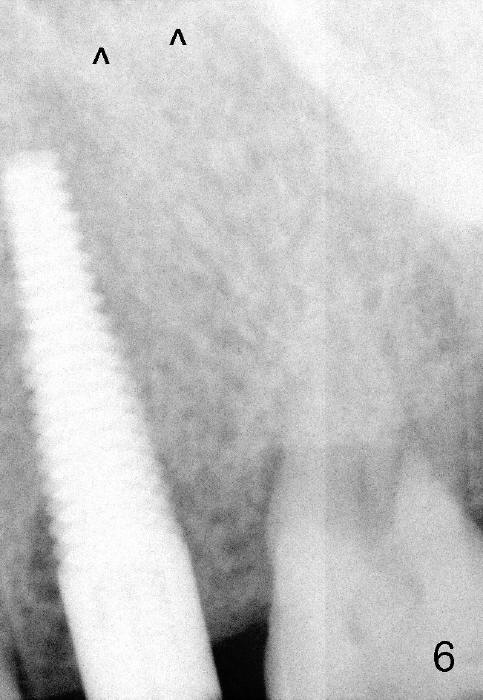
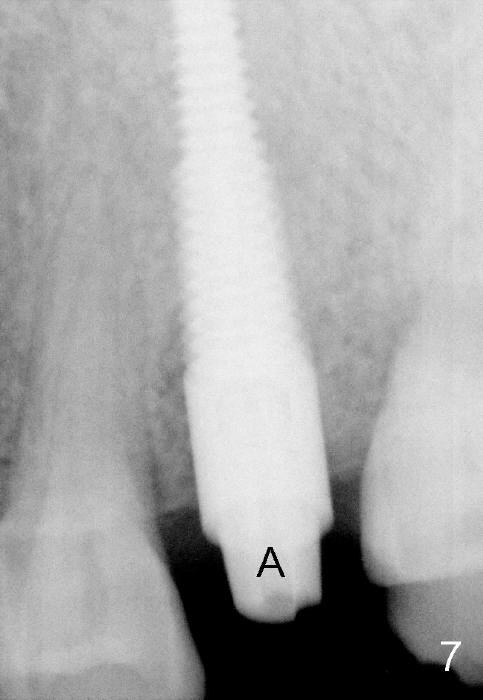
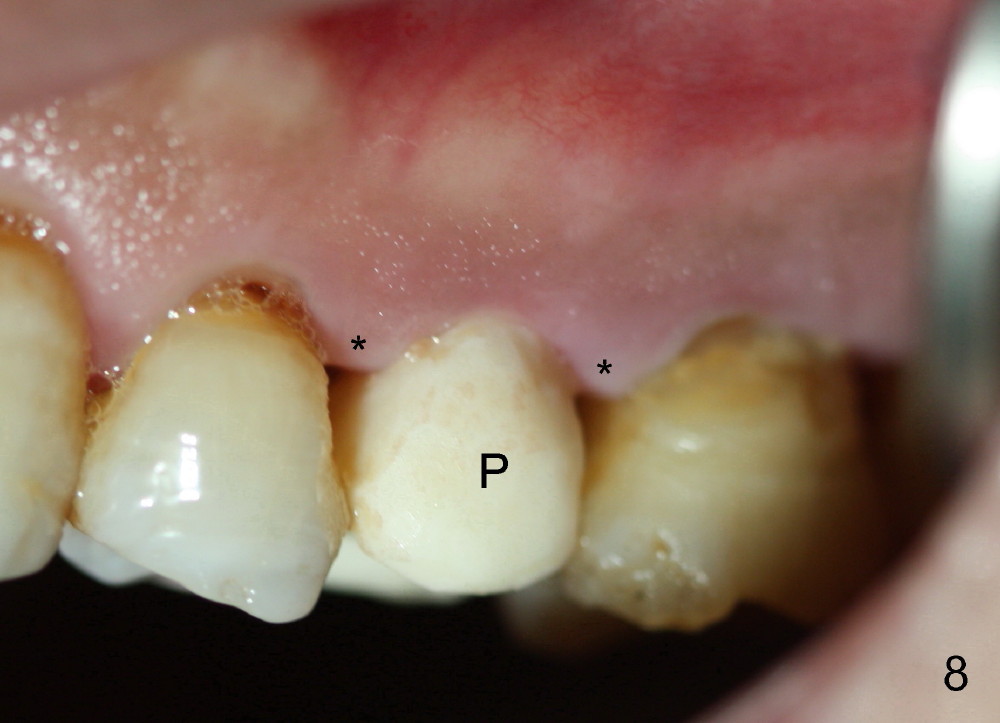
The patient returns for extraction and immediate implant 8 months after #13 palatal cusp fracture (Fig.1). He reports occasional discomfort and mild mobility. Preop PA shows periapical (Fig.2 <) and periradicular (*) radiolucency. When the tooth is extracted (Fig.3), the root does not resemble the shape of D implants. A tapered implant appears to be more appropriate for the site. Osteotomy is initiated in the palatal plateau of the socket with 2 mm pilot drill, followed by 2.5 and 3 mm reamers at the depth of 20 mm. A 4.5x20 mm tap, when placed (Fig.5), remains palatal (Fig.4). The corresponding implant achieves insertion torque > 60 Ncm (Fig.6,7). An abutment is immediately placed (A in Fig.8) to support an immediate provisional. Before cementation of the latter, autogenous bone and Osteogen is placed in the buccal gap (Fig.4 *). The latter is expected to heal normally.
There is no postop discomfort. The immediate provisional (Fig.8 P) is stable 10 days postop. The buccal gingival margin is normal, while the papillae are minimally receded (*).
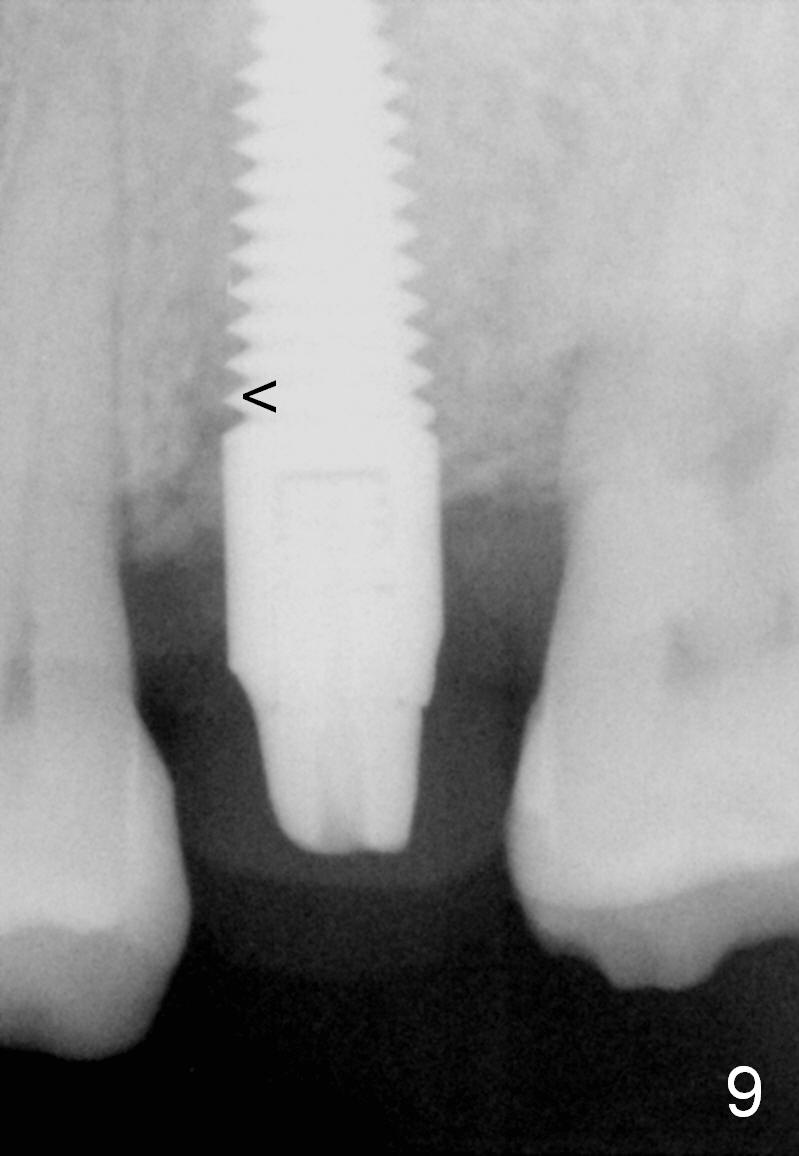
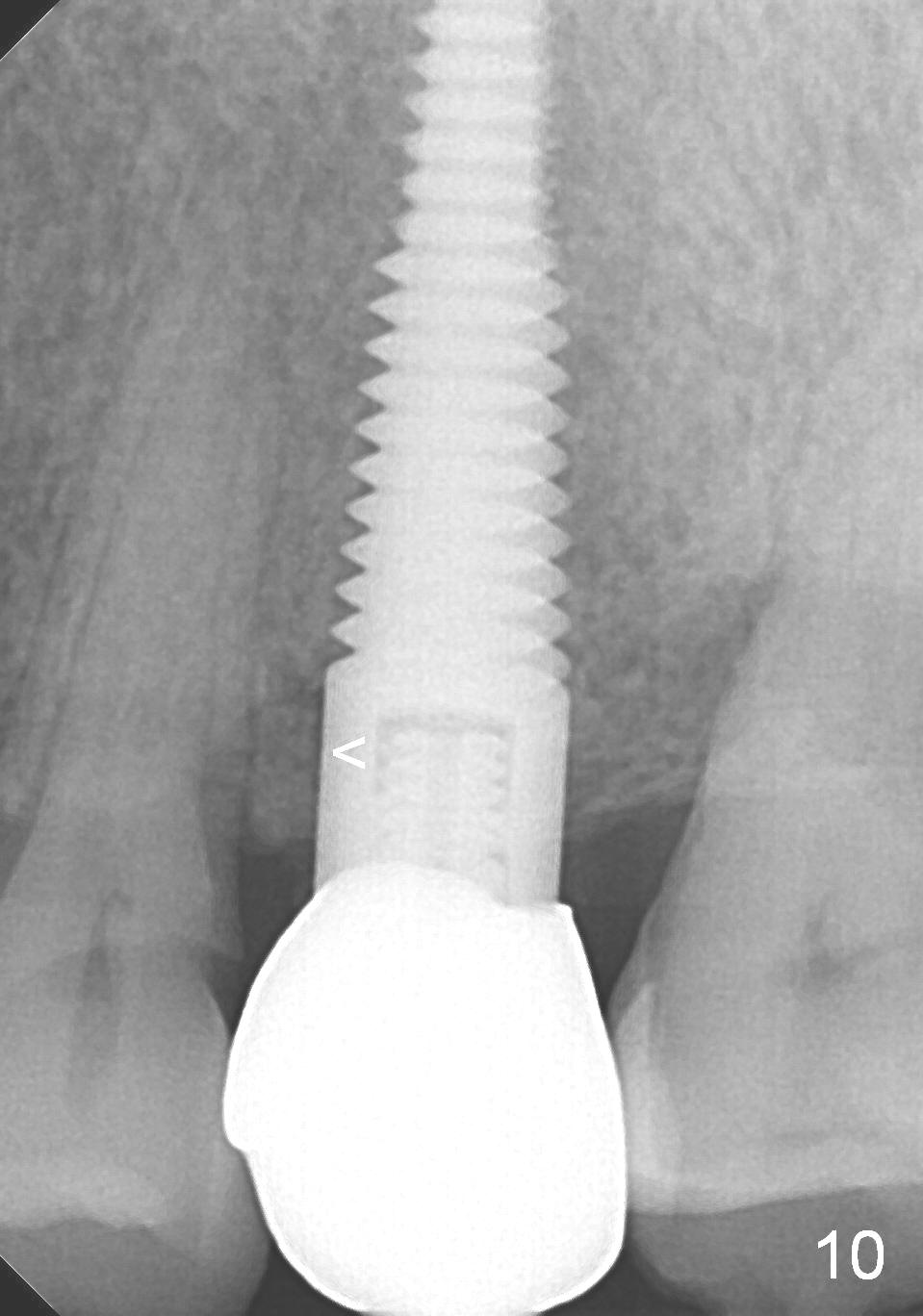
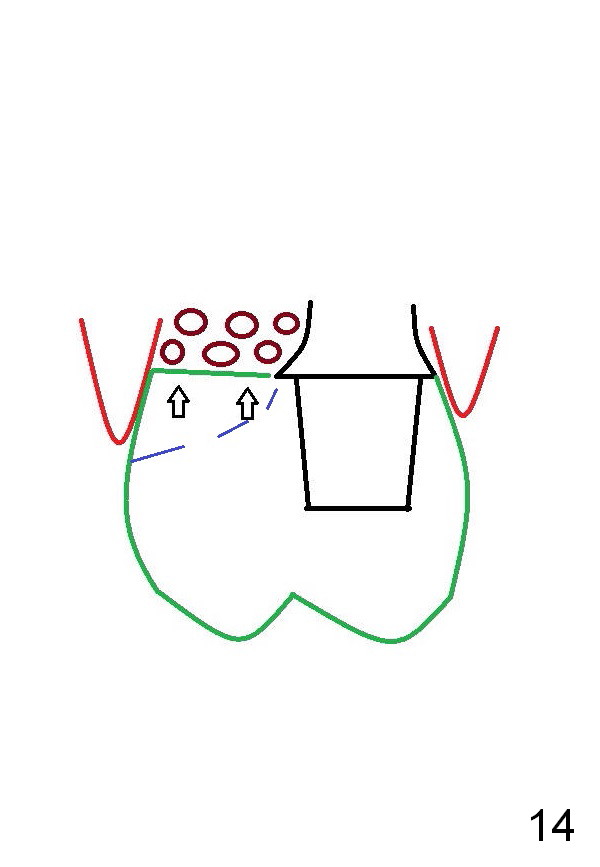
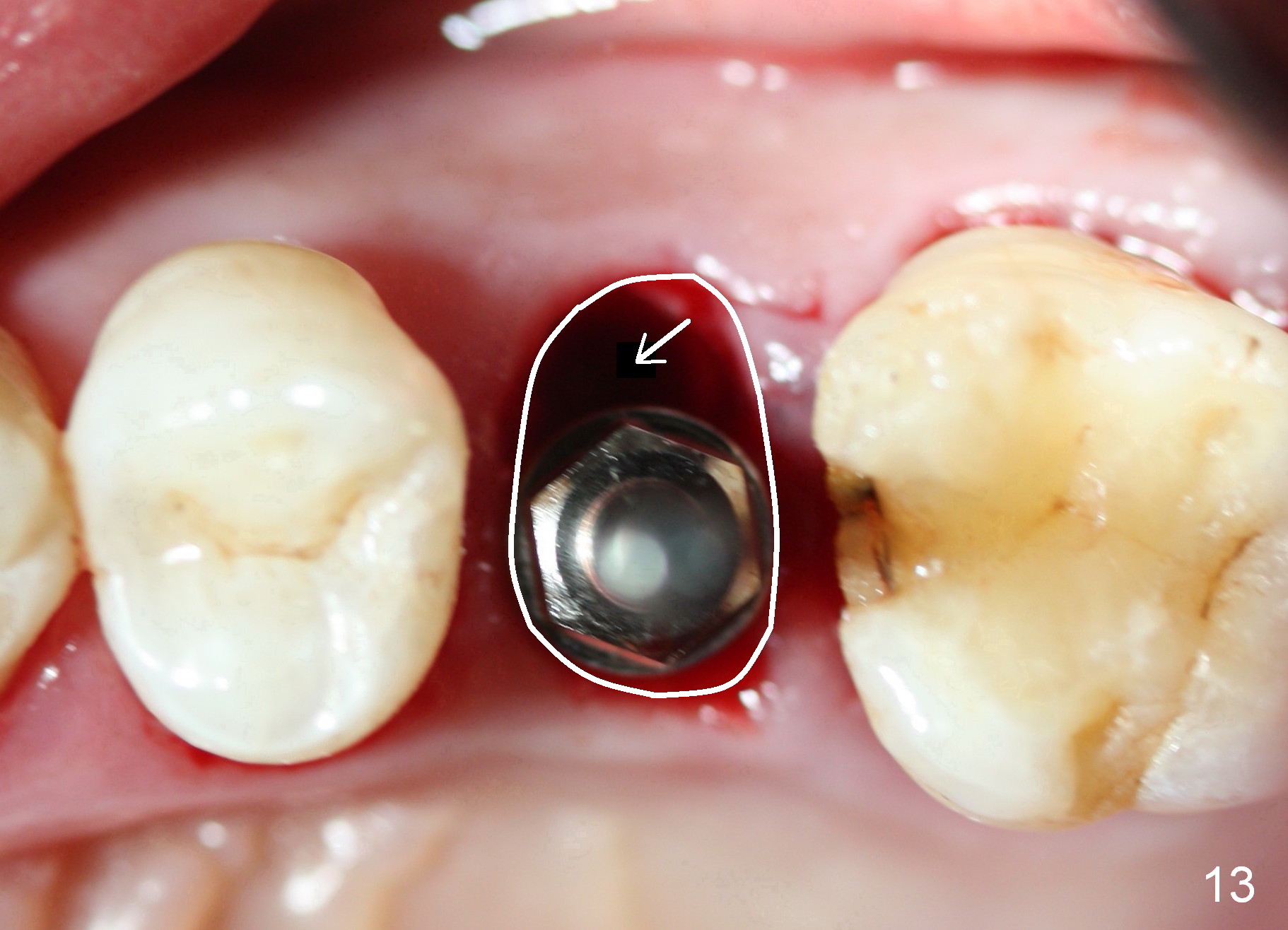
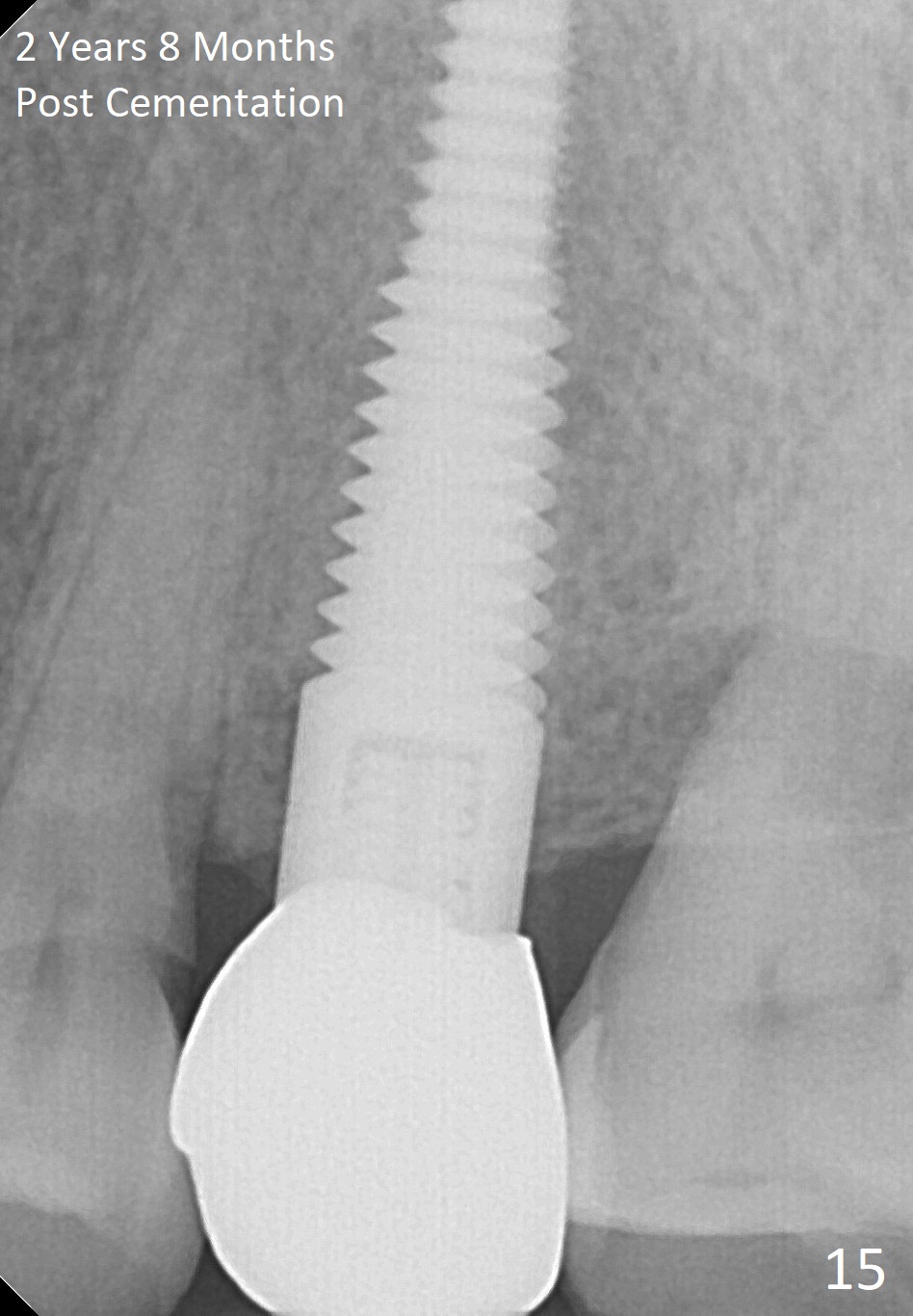
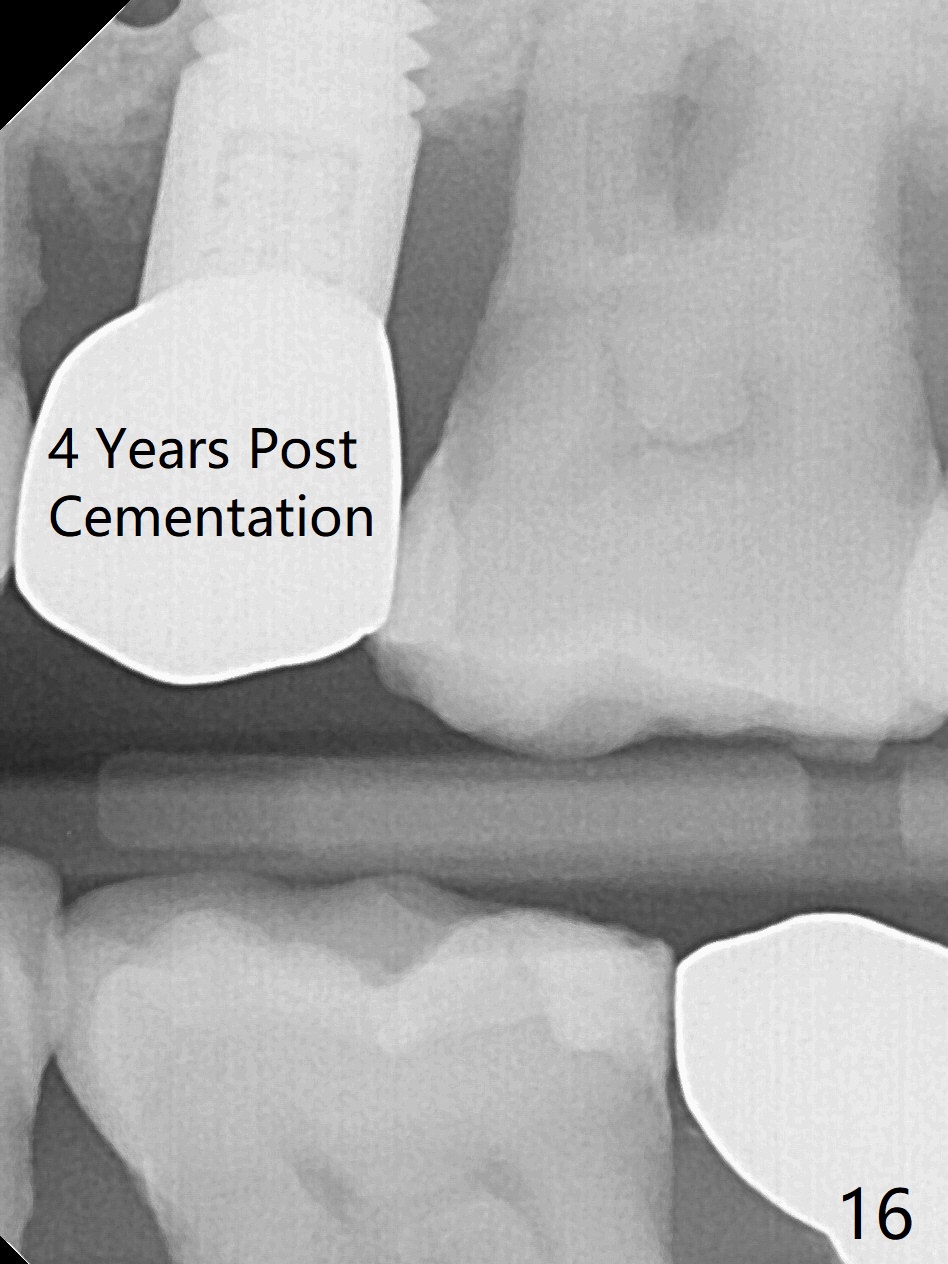
The mesial gap appears to shorten 3 months postop (Fig.9). The gap disappears at the 1st thread of the implant 1 year 8 months post cementation (Fig.10). The patient is pleased with mastication, although the crown looks short (Fig.11). In addition there is concavity at the cervical region (Fig.12 *), which could be prevented by fabrication of a buccal extension of the provisional and definitive restorations into the buccal gap (Fig.13,14 arrow(s)). There is no bone loss 2 years 8 months post cementation (Fig.15). Bitewing shows no bone loss 4 years post cementation (Fig.16). Panoramic X-ray is taken 4 years 6 months post cementation.
Return to
Upper Bicuspid Immediate Implant
Trajectory II
#18,
31,4
Xin Wei, DDS, PhD, MS 1st edition 12/17/2014, last revision 10/19/2019