|
|
|
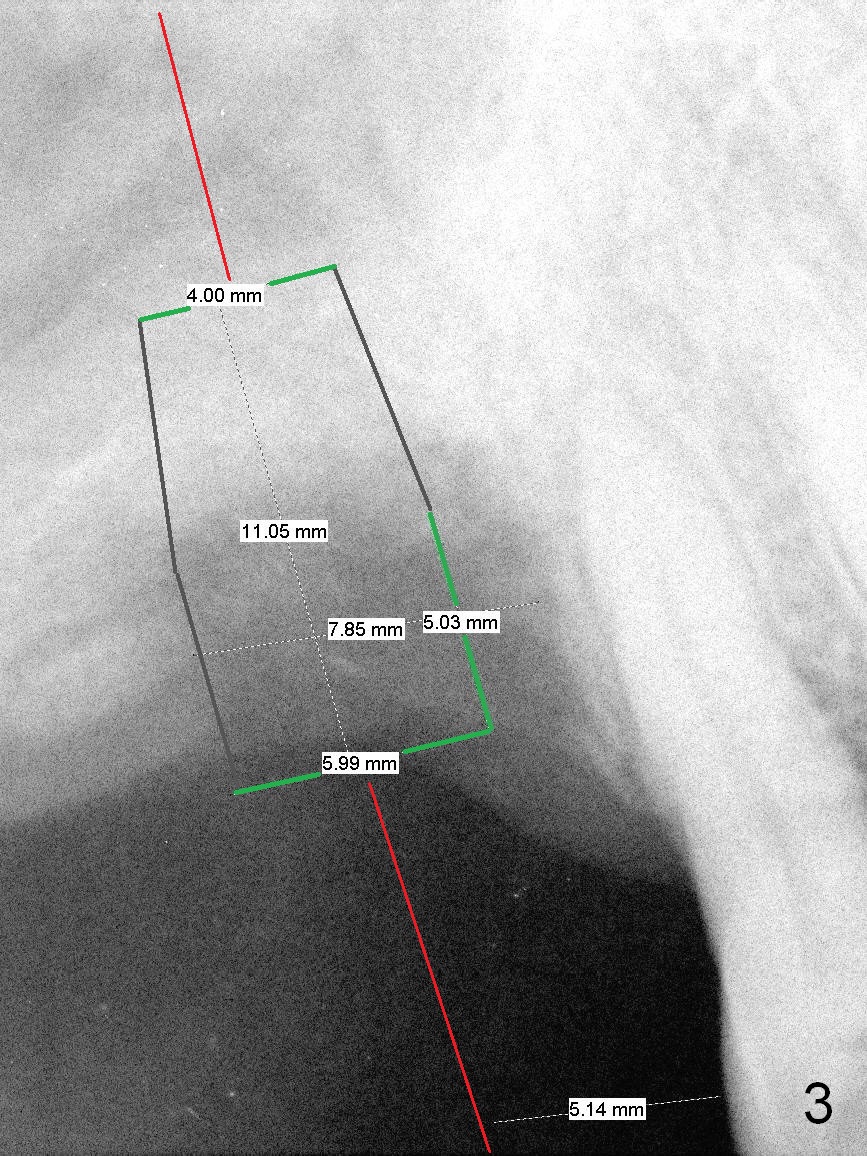
Clinically the buccal plate remains low. Use #15 blade to start bone expansion, followed by 1 and 1.5 mm microosteotomes, RT2,3 and taps (4.5 and 5). The incision should be as palatal as possible. The implant does not need to be large. Primary stability is priority. Use 4.5 mm implant spacer when 1 mm microosteotome is used; 4 for RT2 (rounded tapered osteotome); 3.5 for RT3. If the RT2 feels stable, insert a parallel pin to make sure that the axis of the osteotomy is parallel to that of the neighboring teeth (Fig.3 red line). Also make certain that the coronal end of osteotomes and taps is in the center of the occlusal table.
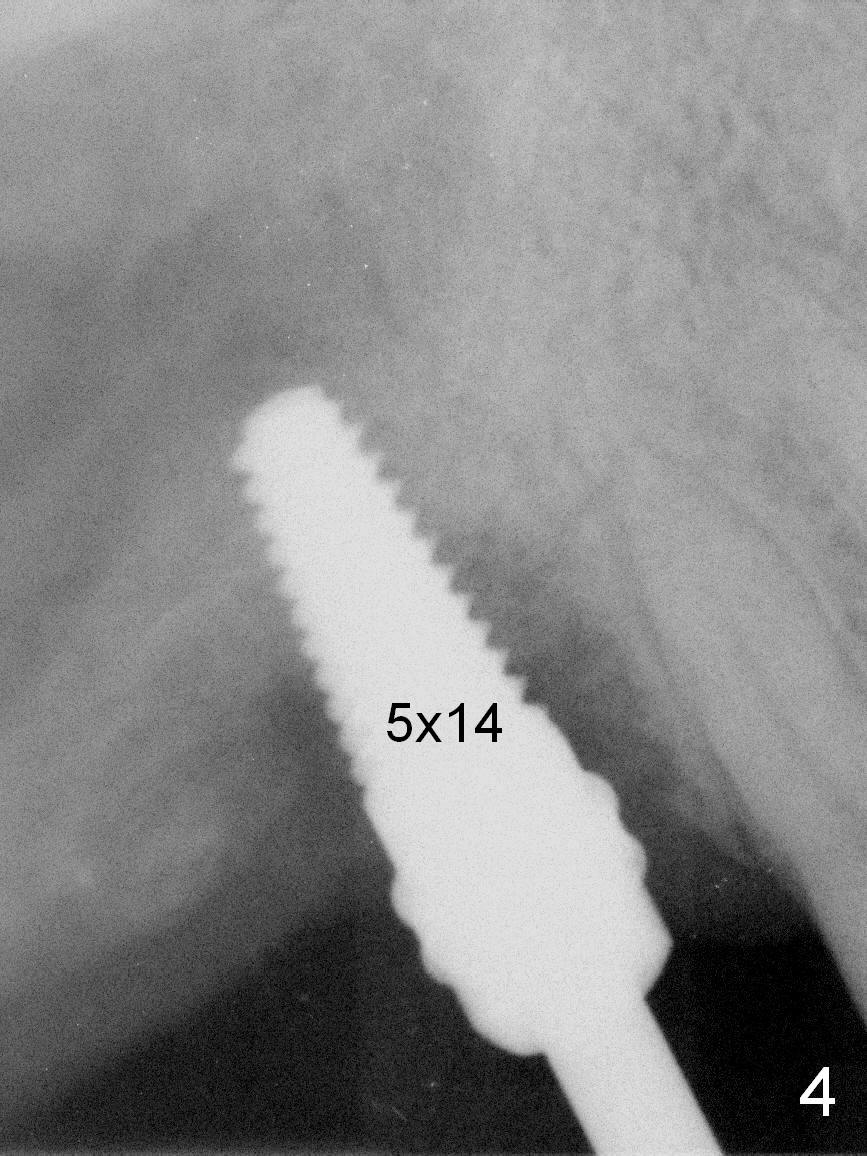
Surgery proceeds as planned above except that RT4 has to be used prior to insertion of taps (Fig.4).
Xin Wei, DDS, PhD, MS 1st edition 03/09/2016, last revision 02/05/2019