


|
|
|
|
|
|
|
|
|
|
|
|
||
When to Trim Immediate Provisional Margin?
There are 2 questions to be discussed with the present case: 1st as the title; 2nd: does upper posterior immediate implant have to engage into the sinus floor to have primary stability?
An immediate implant should be as long as possible to achieve primary stability. It may create hazard in the mandibular posterior region. Although there has been no problem placing an immediate implant into the sinus, it will be interesting to test whether a shorter implant is able to obtain enough stability.
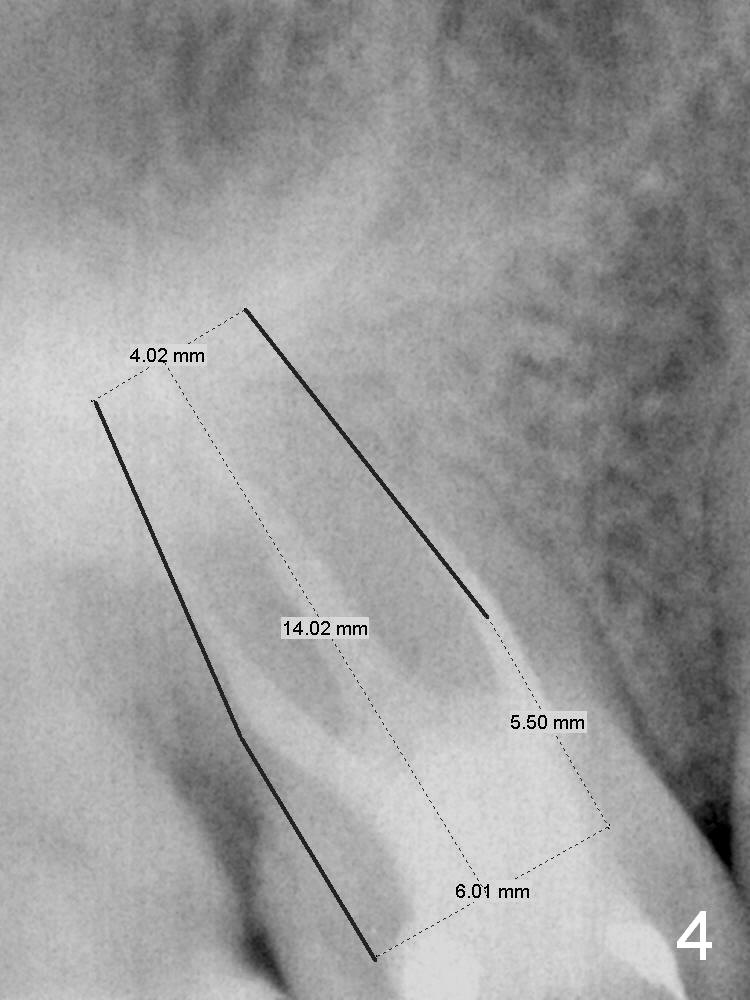
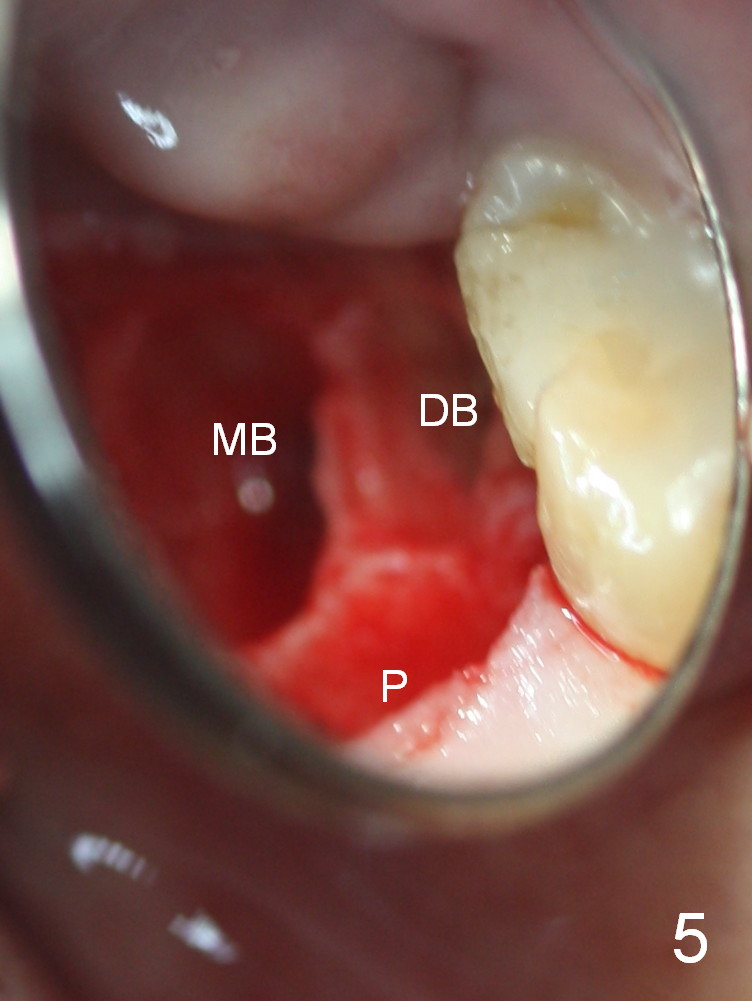
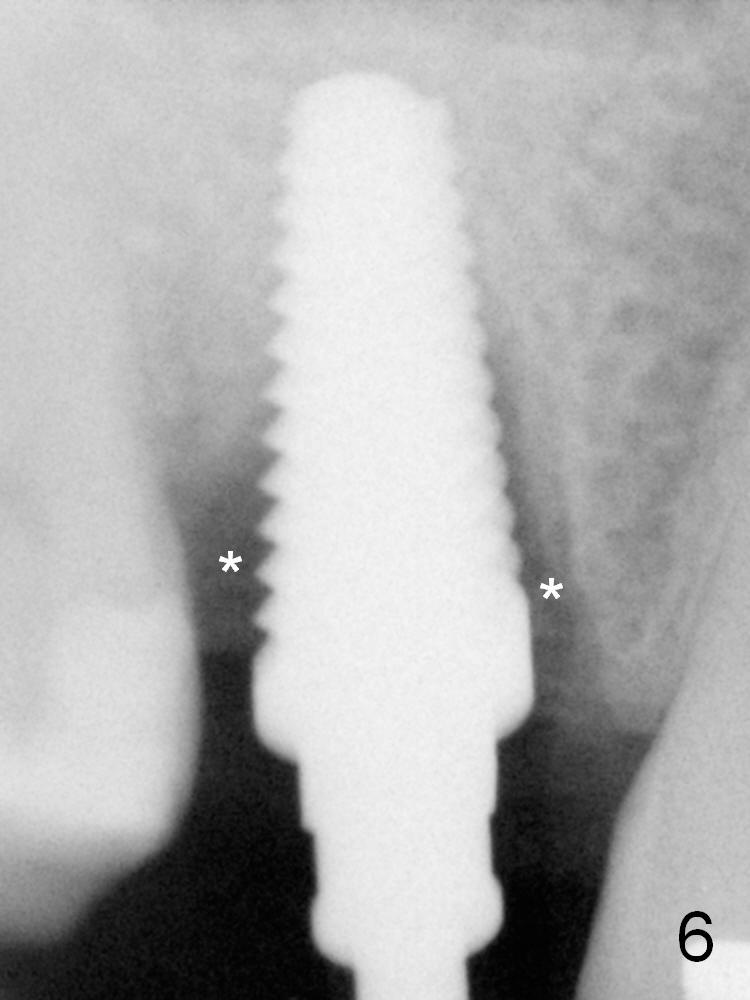
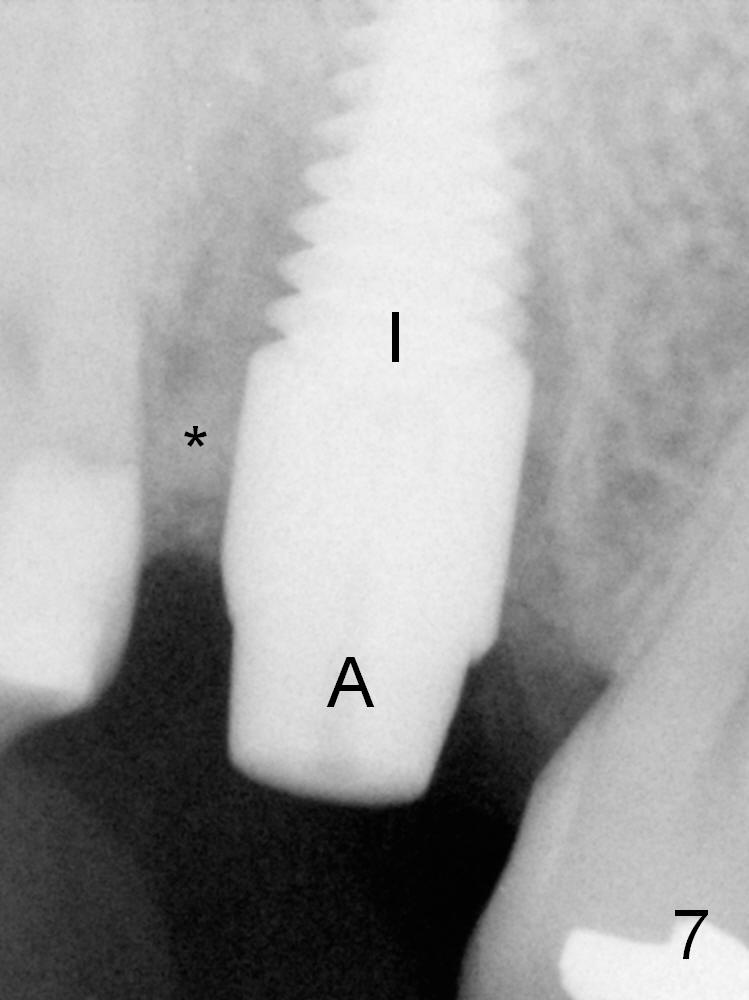
A 46-year-old lady has had root canal therapy for the tooth #3 without a crown for 6 years (Fig.1,3). The mesiolingual cusp fractures subgingivally (Fig.3). The new PA is used for design of a 6x14 mm tissue-level implant (Fig.4), but the old PA (Fig.2) is used to measure the height of the septum. After extraction, osteotomy is initiated in the middle of the septum (Fig.5) and underprepared. The height is tightly controlled. When a 6x14 mm tap is inserted, the stability is high, while the sinus floor has yet to be reached (Fig.6). The insertion torque of the same sized implant is >60 Ncm (Fig.7 I); a 5x3 mm abutment is placed immediately (A); the peri-implant space is filled with mixture of autogenous bone (harvested from osteotomy with reamers), allograft and Osteogen (compare Fig.6,7 *). An immediate provisional is fabricated to cover the socket opening.
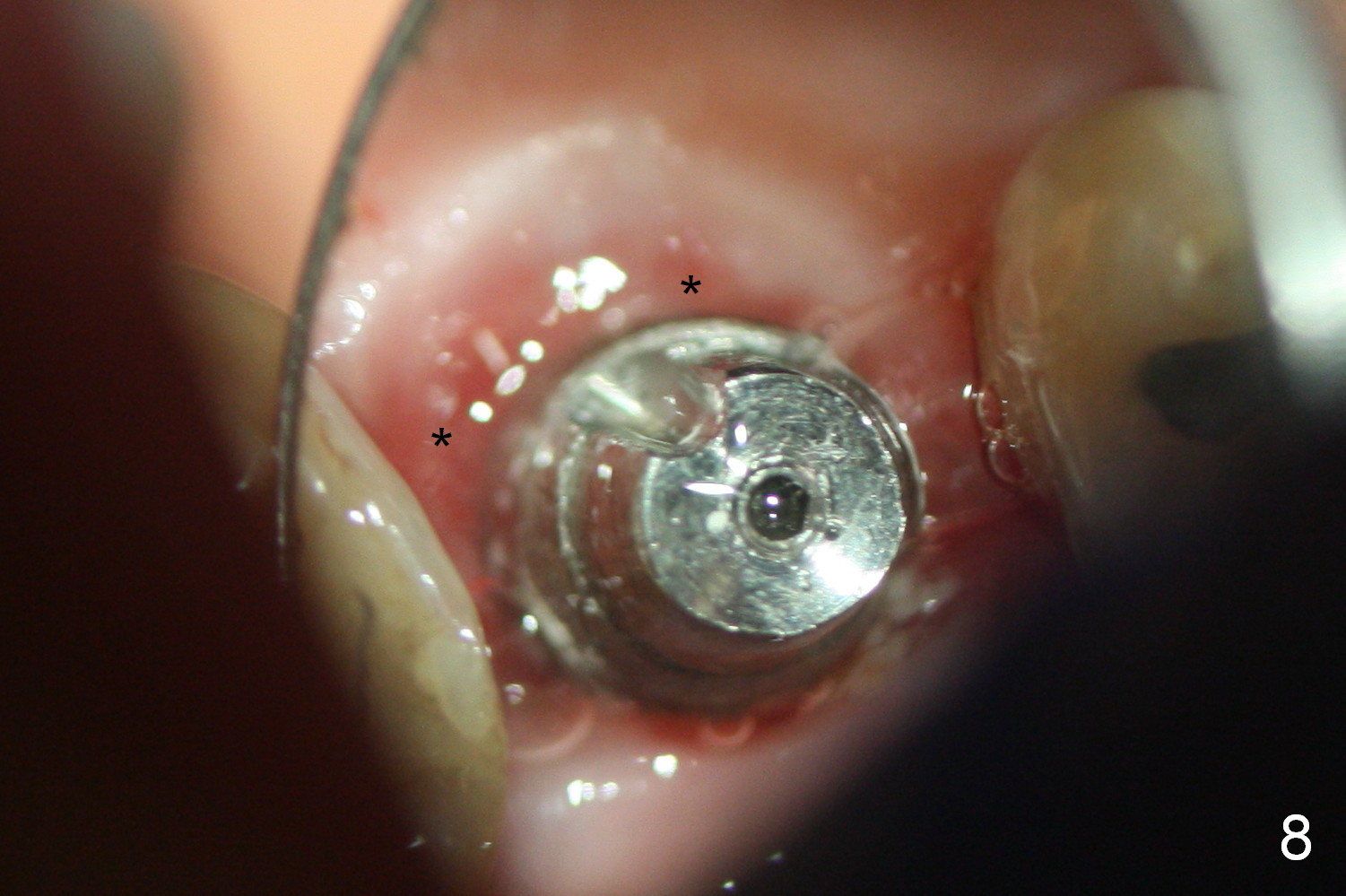
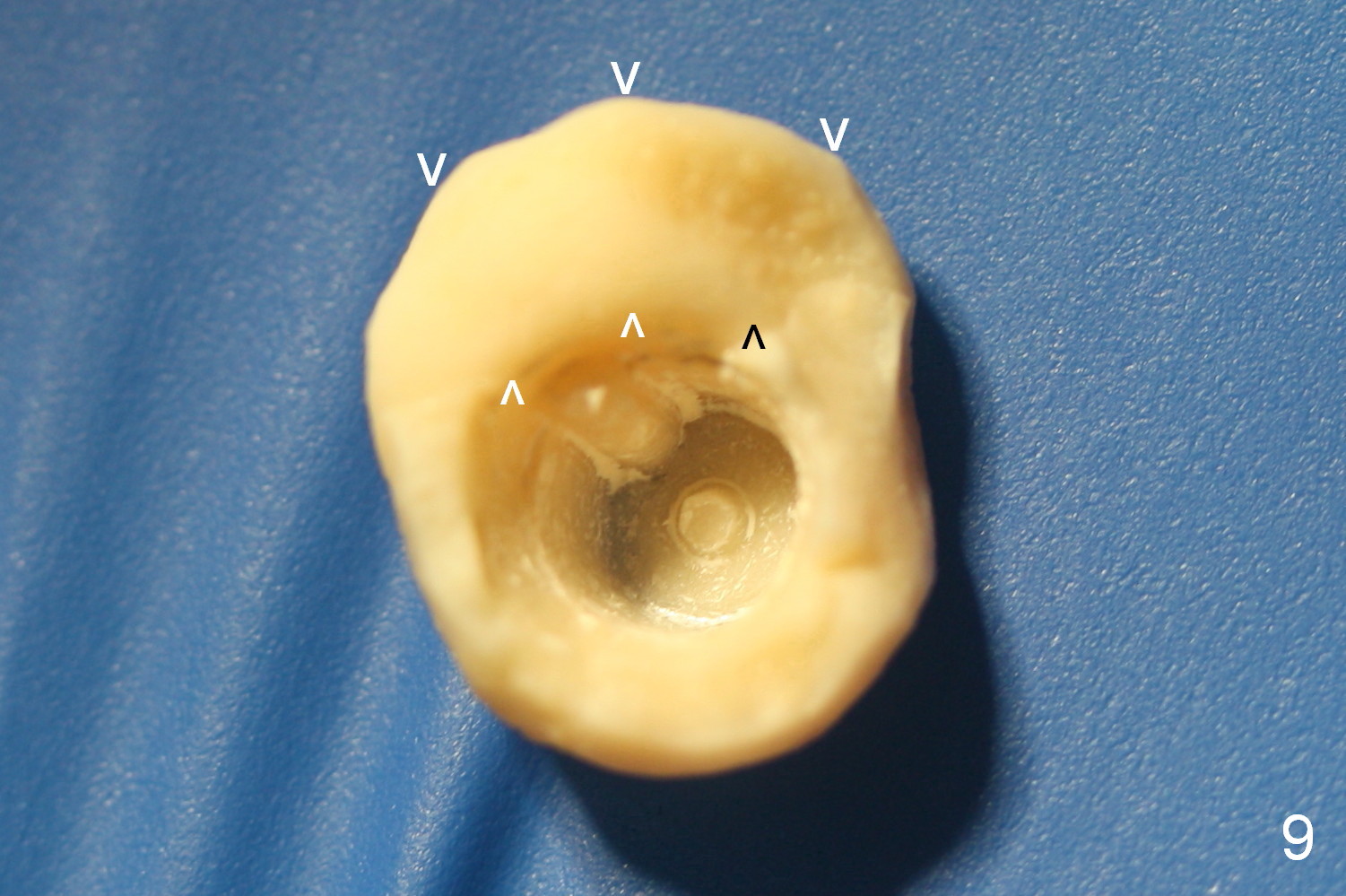
One month postop, the patient returns with complaint of discomfort associated with the implant. Exam reveals no abnormality. When the provisional is removed, fresh granulation tissue is found at the entrance to the socket (Fig.8 *). It appears that the excess margin of the provisional (between arrowheads in Fig.9) should be trimmed for better oral hygiene maintenance.
An immediate provisional can be modified once the socket heals. A short implant without reaching the sinus floor can obtain primary stability as long as the osteotomy is underprepared.
Return to Upper Molar Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 07/04/2015, last revision 07/04/2015