

|
|
|
|
|
|
|
|
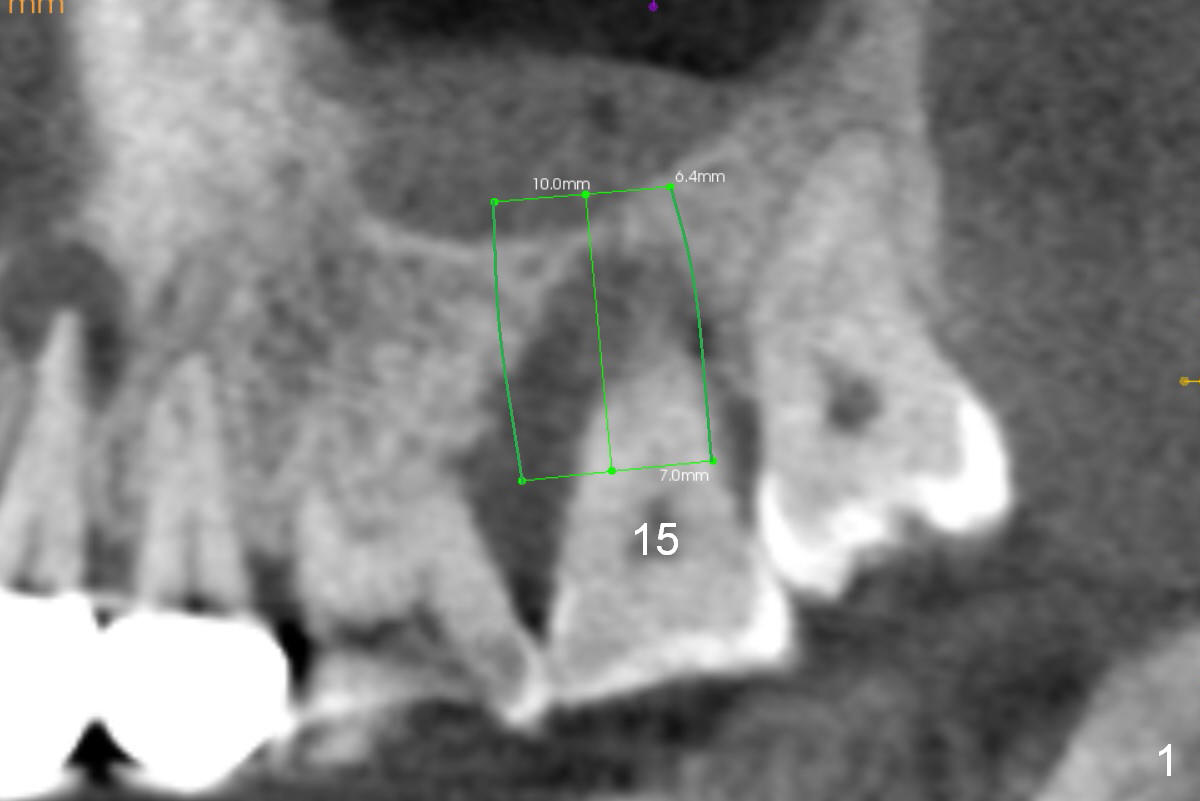
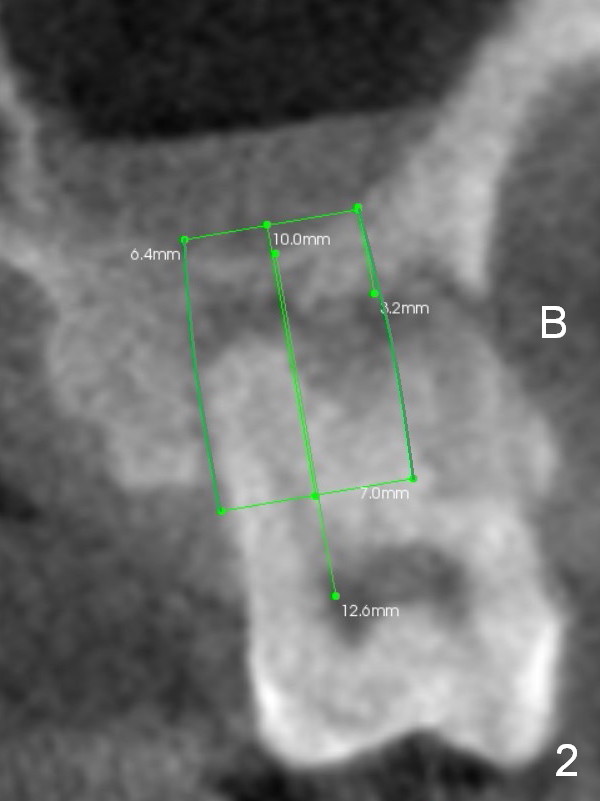
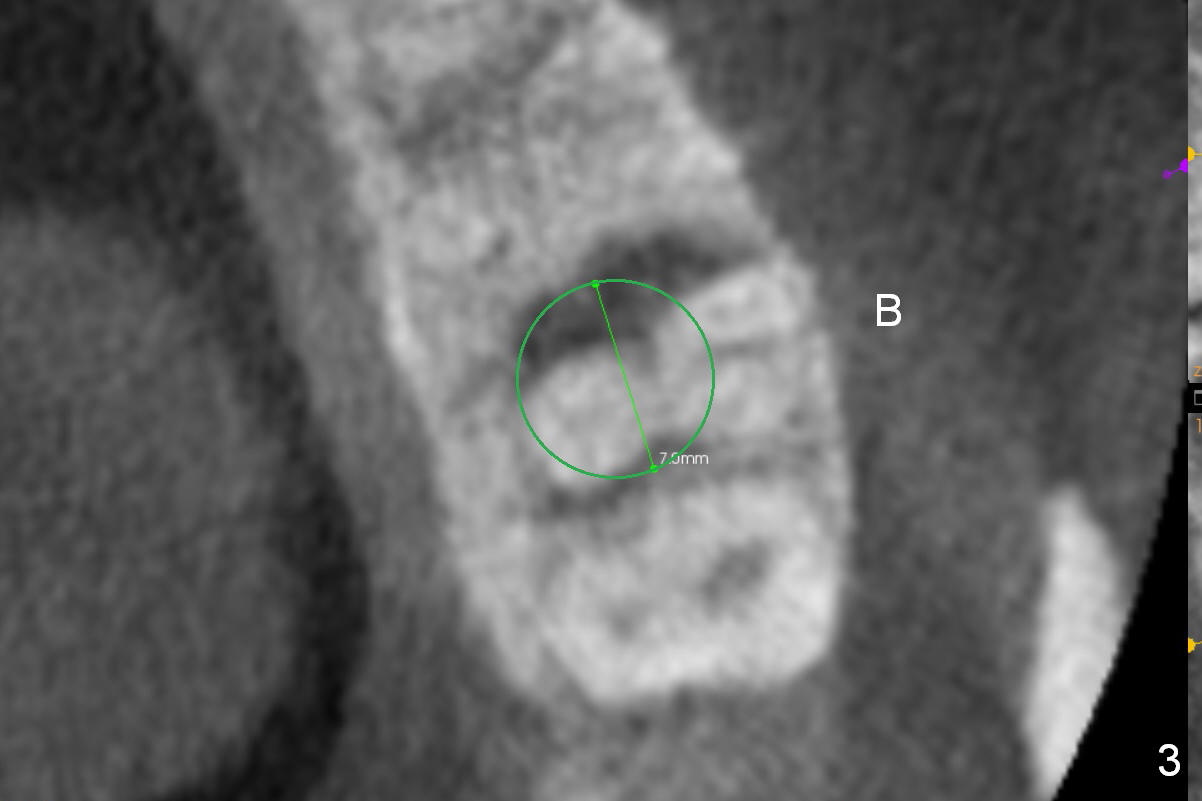
Immediate Implant Engages into 3 Walls of the Socket
A 42-year-old lady (HJ) has advanced periodontitis at #15 (Fig.1 (CBCT sagittal section)). The buccal (B) plate is thin (Fig. 2 (coronal section), 3 (axial section)). The apical bone is also thin (Fig.1,2). A 7x10 mm implant is placed in a position so that the implant contacts the mesial, palatal and distal walls of the socket (treated with 2% Xylocaine with 1:50,000 Epinephrine) for primary stability (Fig.3). The buccal gap will be filled with Osteogen Plug apically (Fig.4 purple rectangles) and bone graft coronally (red circles). SM implant (Fig.4) is more tapered than UF one (Fig.2), easier to insert.
Open Sinus Master Kit and use 2.8 and 3.6 mm round burs at 2 mm depth to start osteotomy, followed by 4.5-6x14 mm Tatum tapered taps at 11 mm and SM or UF 6.5 mm tap. If stability of the last tap is low, insert a 7 mm implant. If the Sinus Master Kit does not work, try RT2-4. Draw blood after extraction confirms buccal wall defect. Place PRF before Osteogen Plug and bone graft (Fig.4' yellow curved line).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/31/2015, last revision 04/18/2016