

|
|
|
|
|
|
|
|
|
|
Sinus Floor is Too Hard for Sinus Lifter
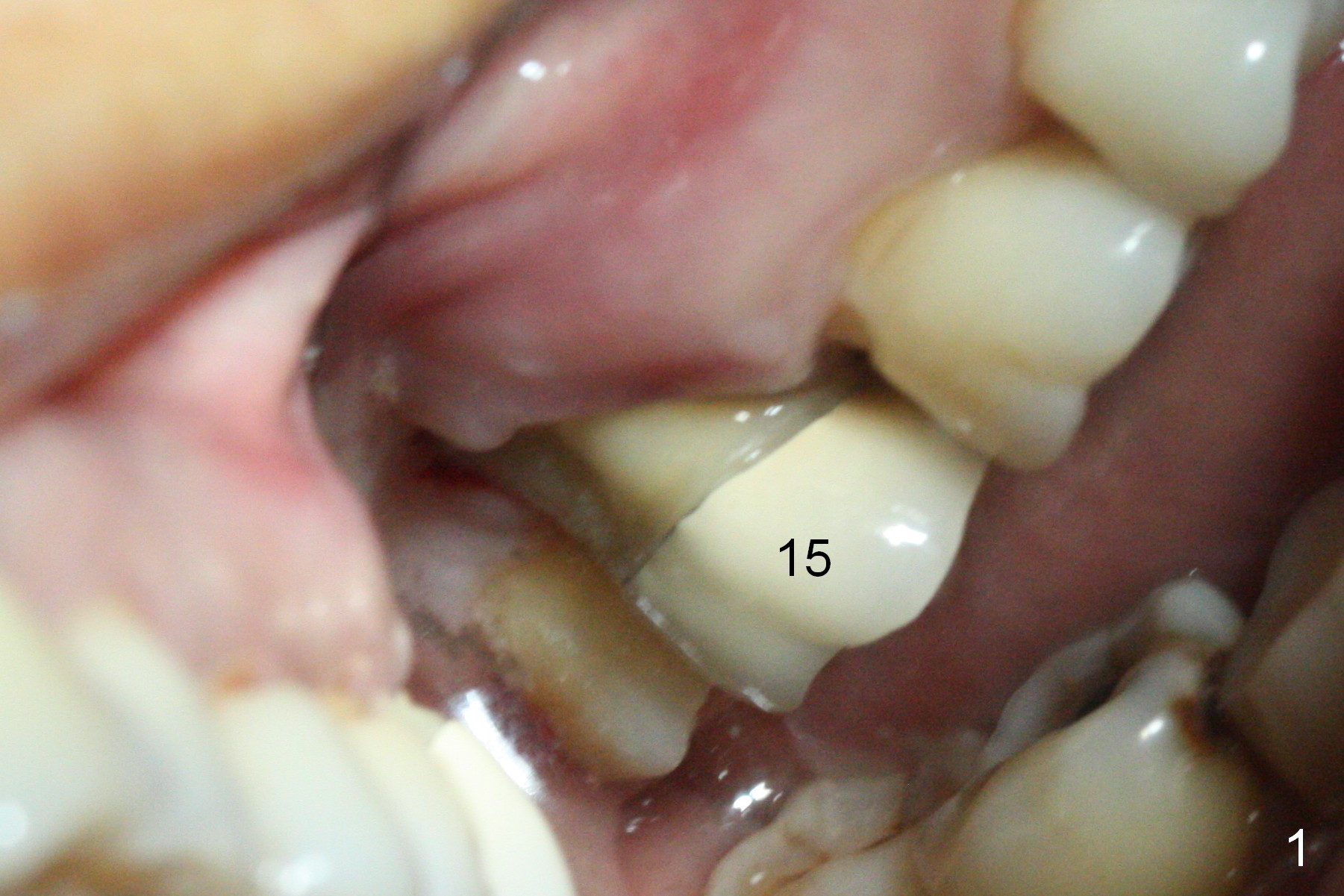
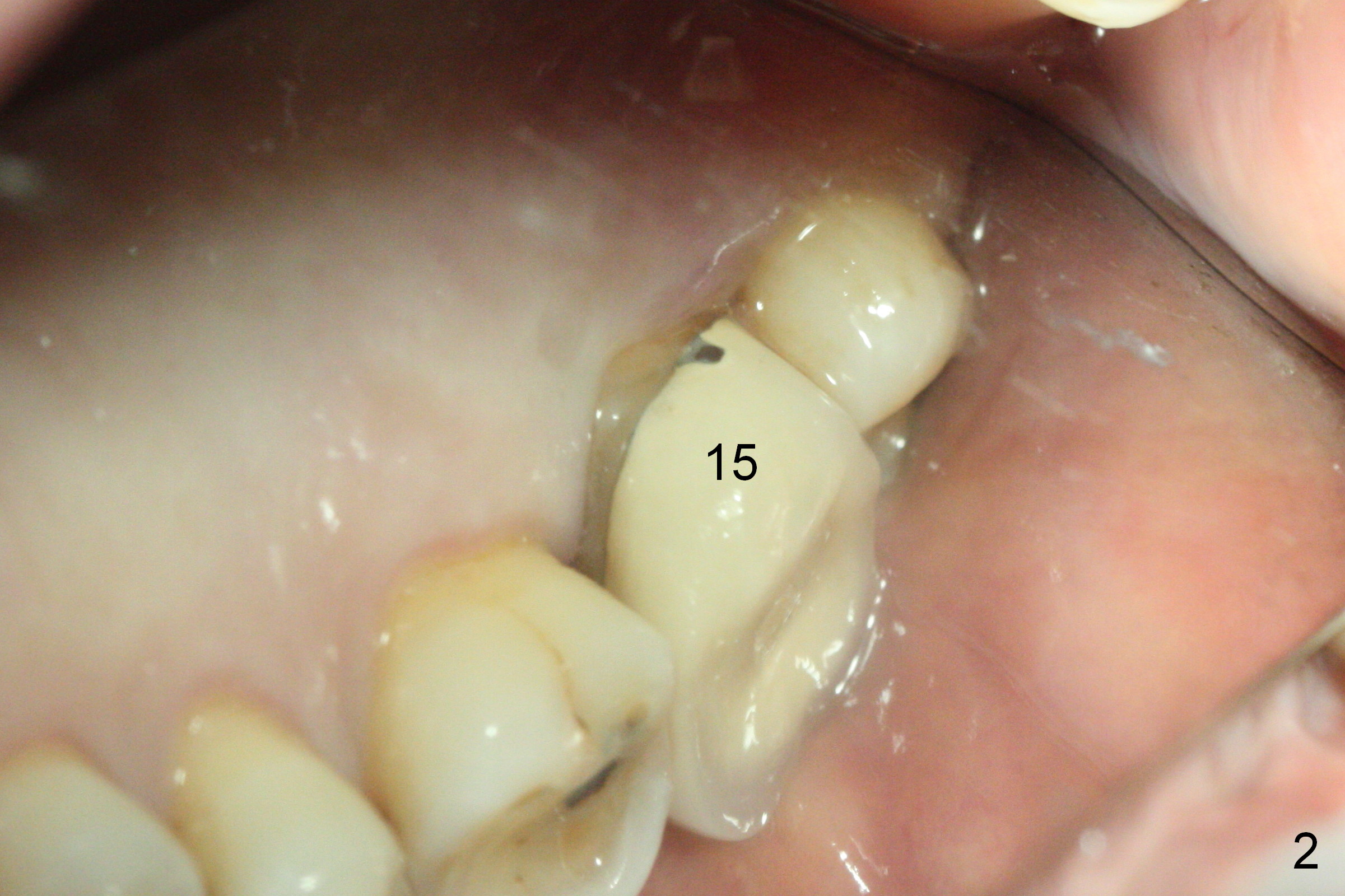
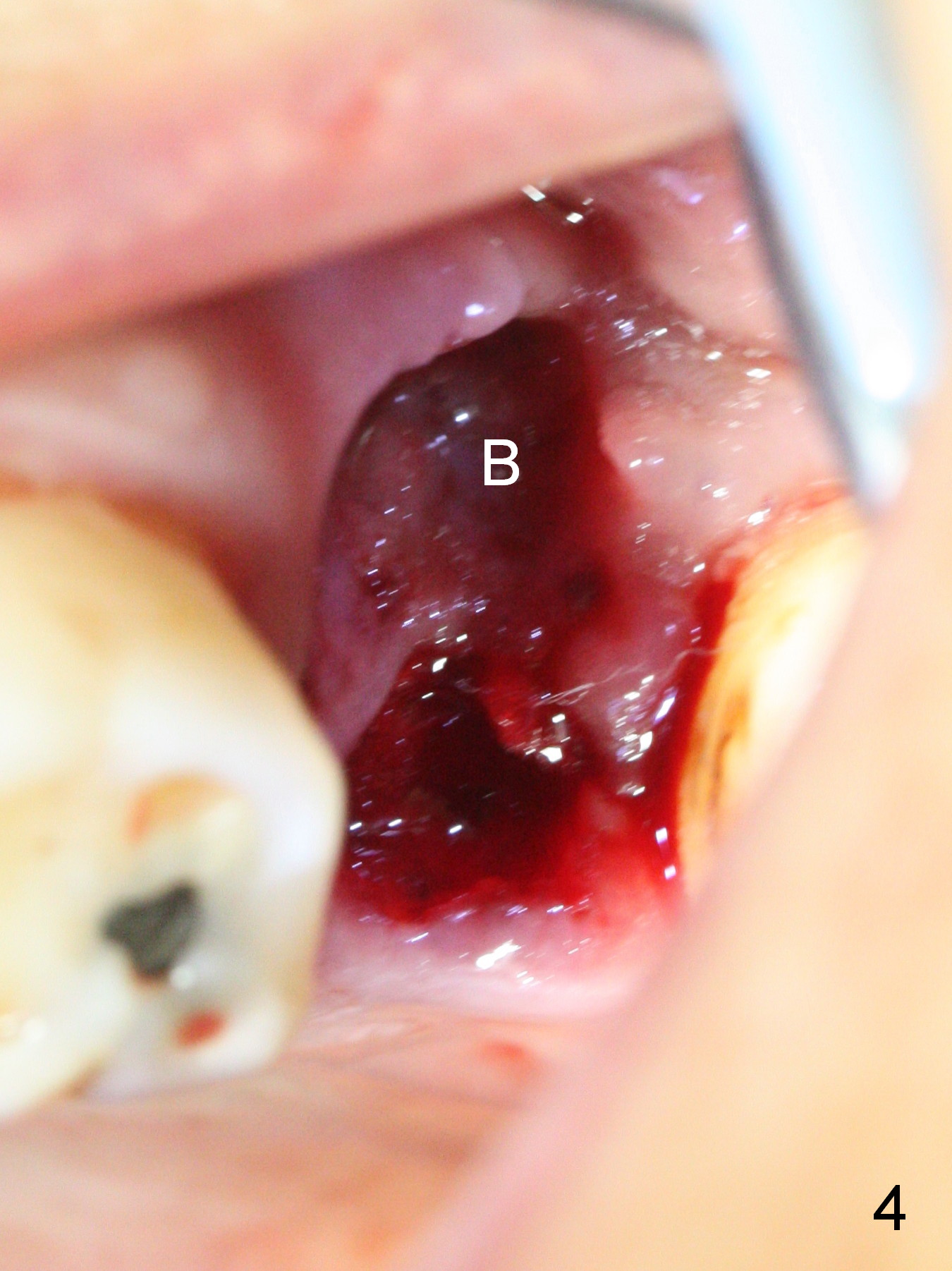
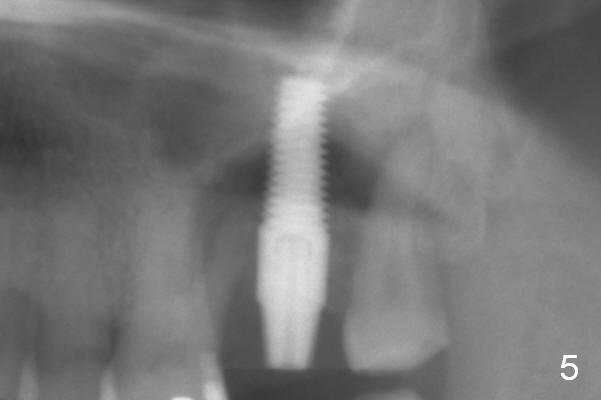
The mobile tooth #15 has severe buccal recession (Fig.1), whereas the palatal recession is moderate (Fig.2). More calculus appears to be found in the mesiobuccal (Fig.3 MB) and distobuccal (DB) roots than the palatal one. The shallow buccal (Fig.4 B) socket seems to be not a proper site of implantation, while the palatal one is chosen for osteotomy. The sinus floor is tough for the Sinus Lifter or Magic Expanders (ME). After use of 1.6 mm pilot drill and the smallest Magic Drill (2.8 mm), MEs (3.0 to 4.3 mm) are able to extend 3-4 mm without membrane perforation. Following application of 4.5 and 5x20 mm taps at 17 mm, a 5x17 mm gingiva-level implant is placed with ~45 Ncm, a 4.5x5 mm abutment placed for an immediate provisional (Fig.5).
The distobuccal wound exposes 6 days postop. A new layer of acrylic is added to the provisional for seal. The provisional has been dislodged 3 weeks postop (Fig.6). The implant is unstable. It causes pain to remove the abutment (A) from the implant (I) without local anesthesia. Since the abutment/implant does not interfere with oral function, no action is taken. The patient is advised to return in 1 month.
Return to Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
IBS
Xin Wei, DDS, PhD, MS 1st edition 10/04/2016, last revision 10/27/2016