

,%20allograft,%20Osteogen.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
||||
Underprep for Immediate Implant
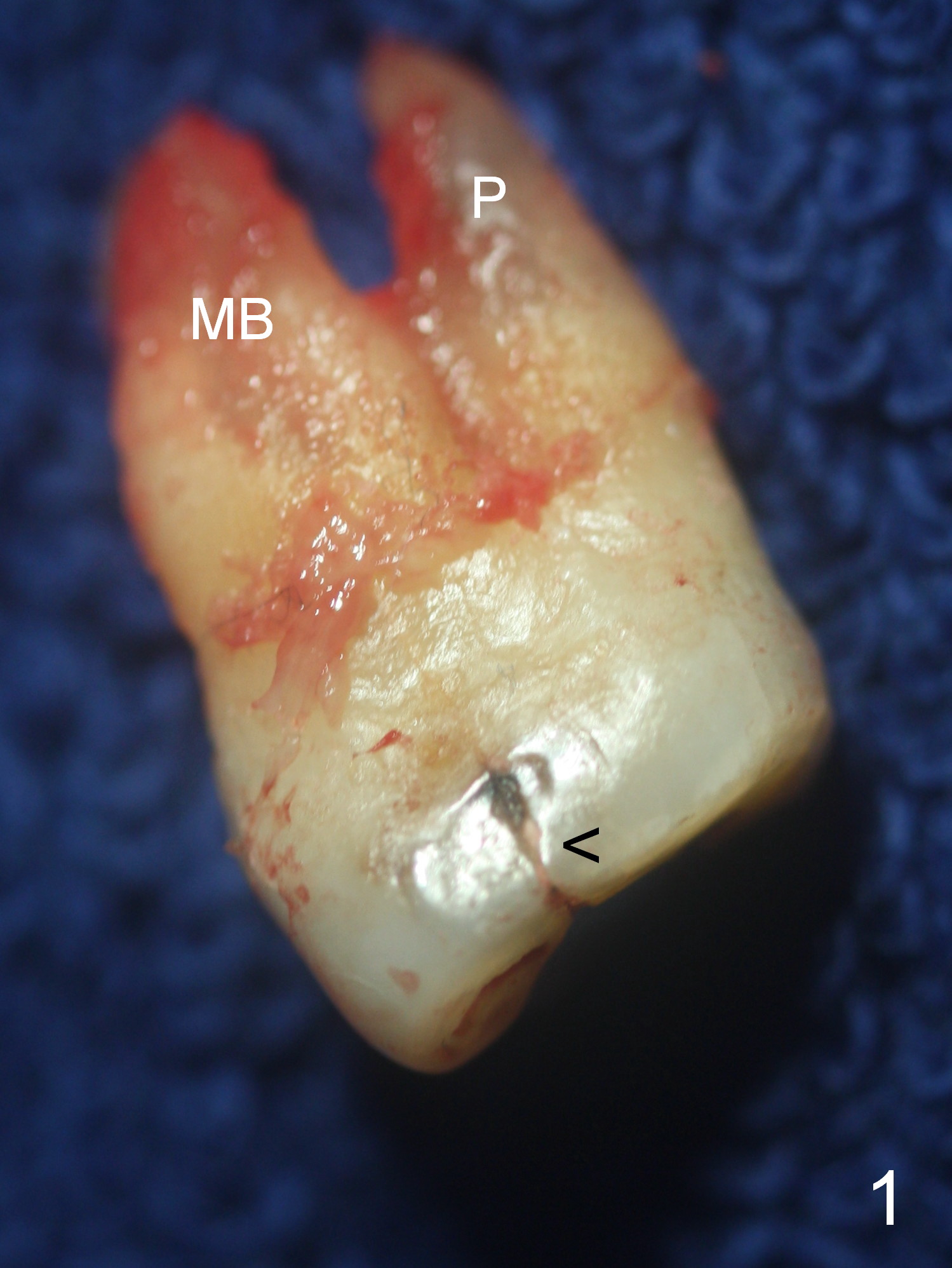
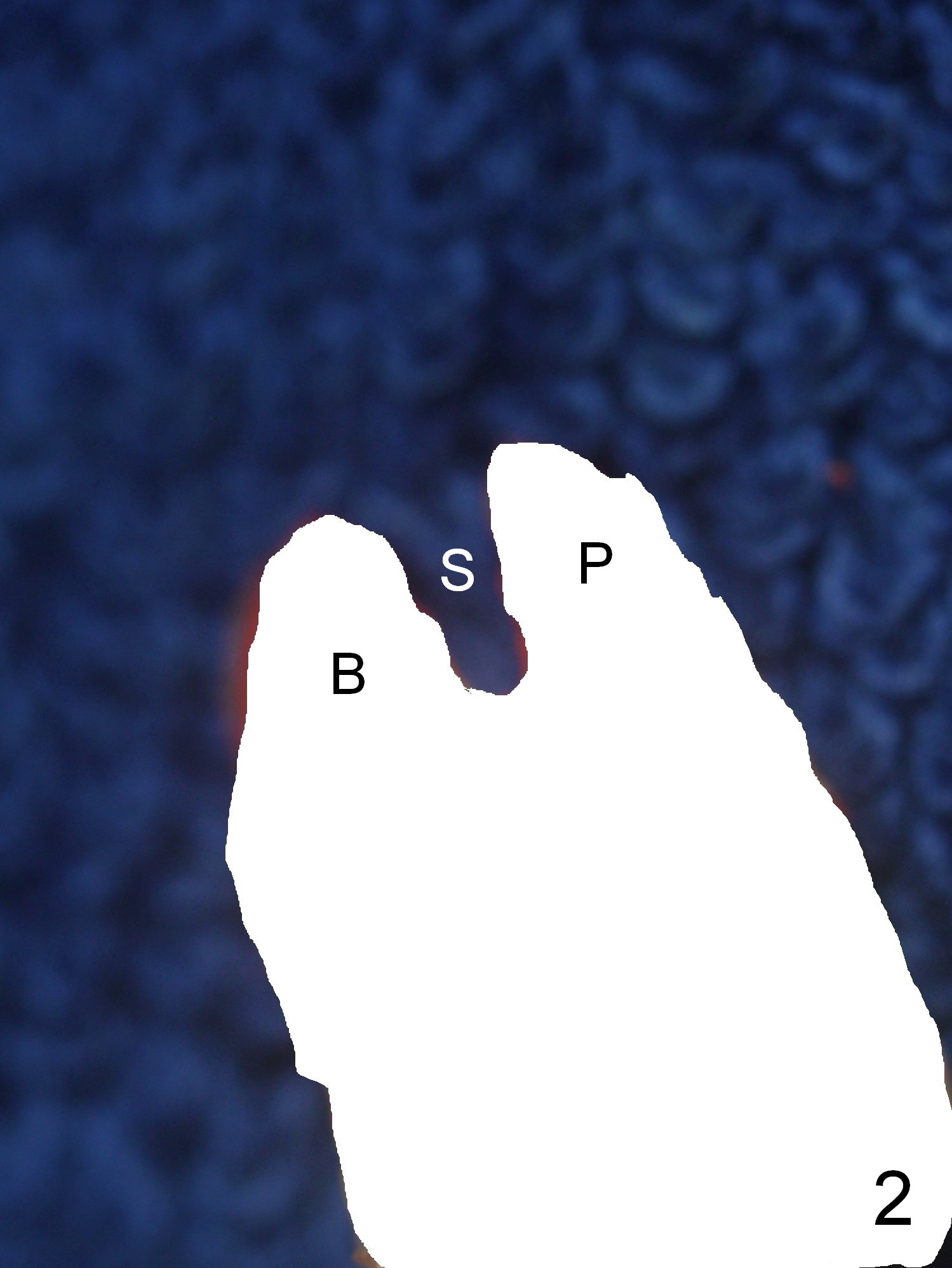
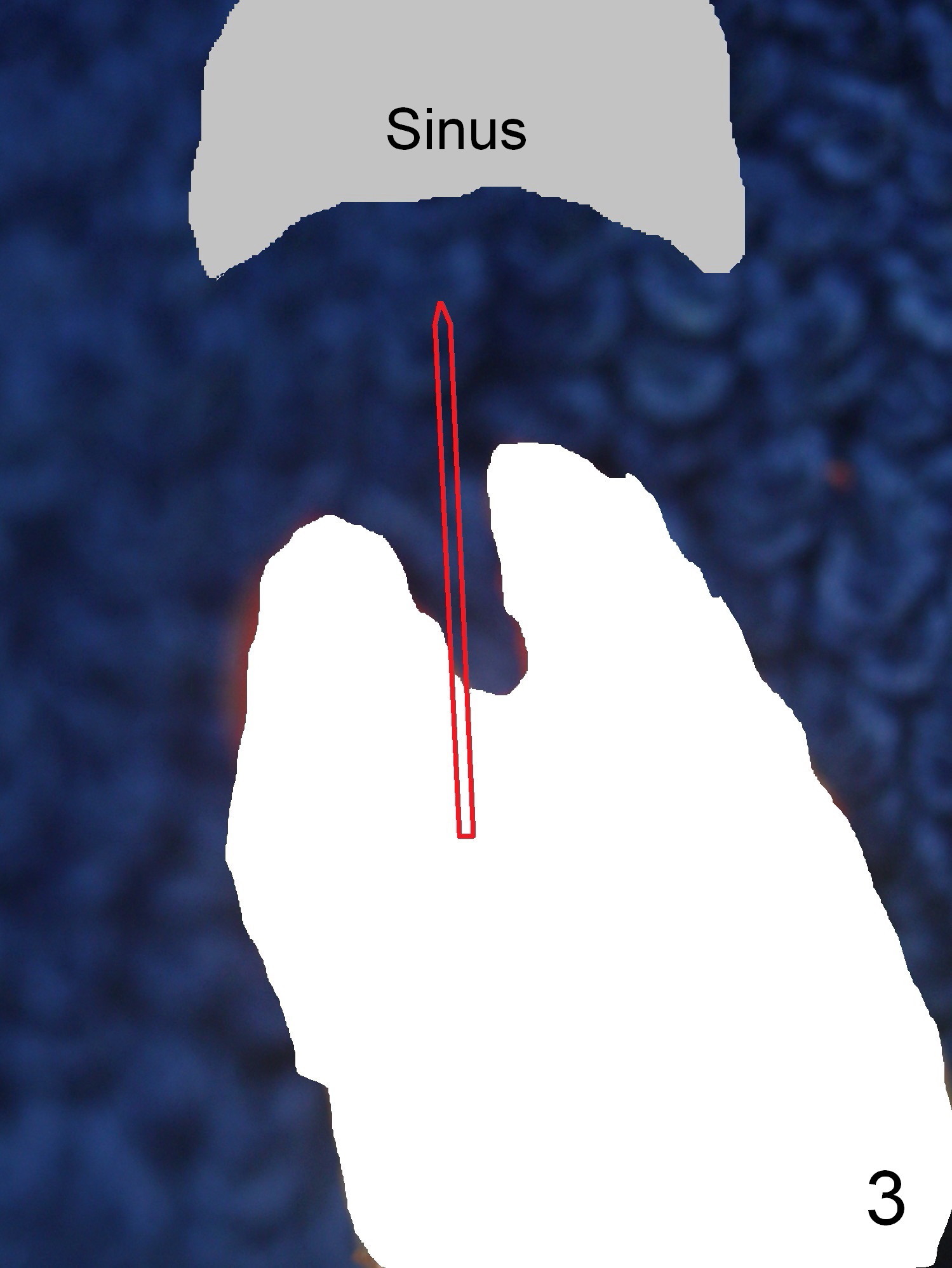
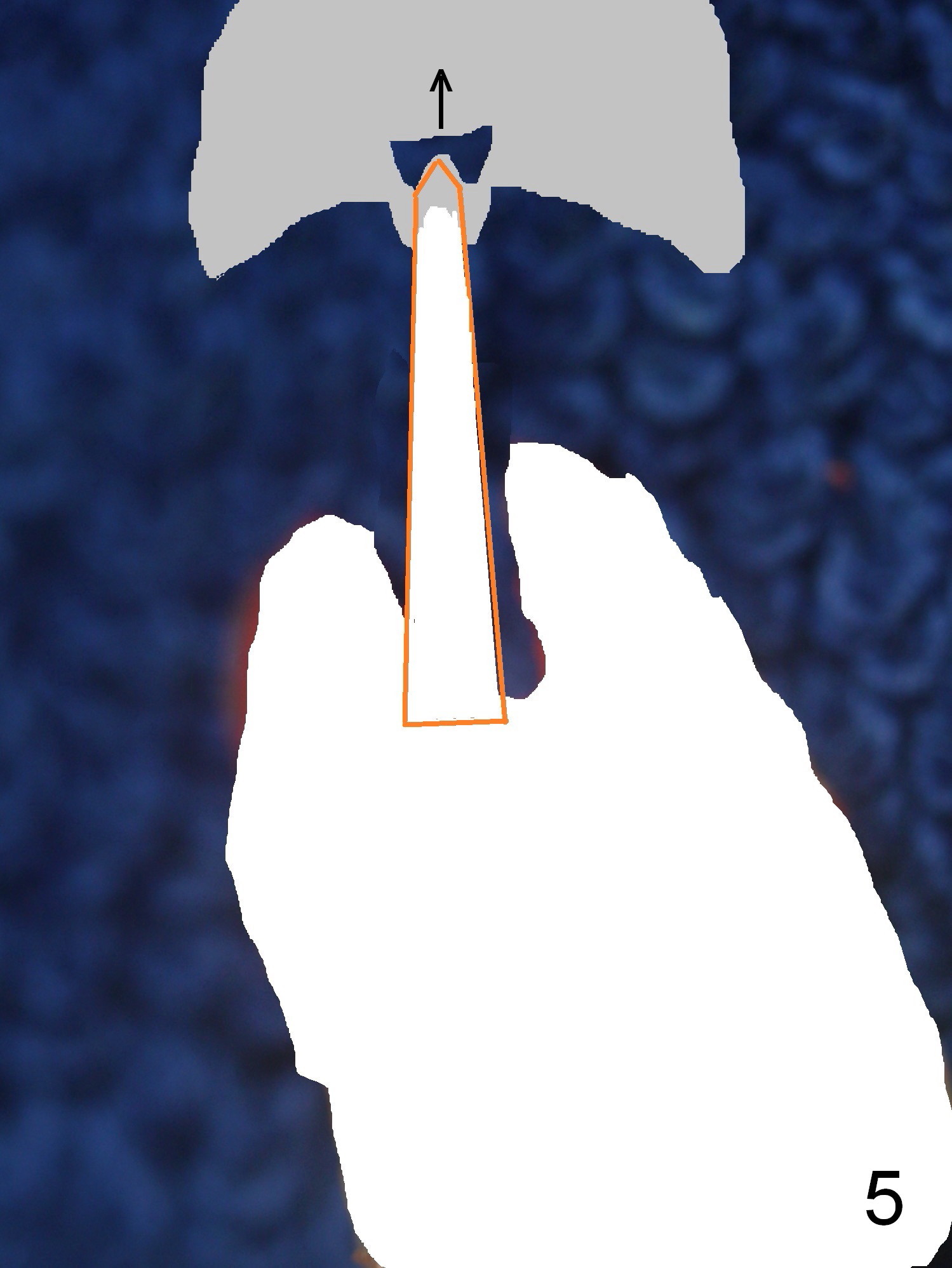
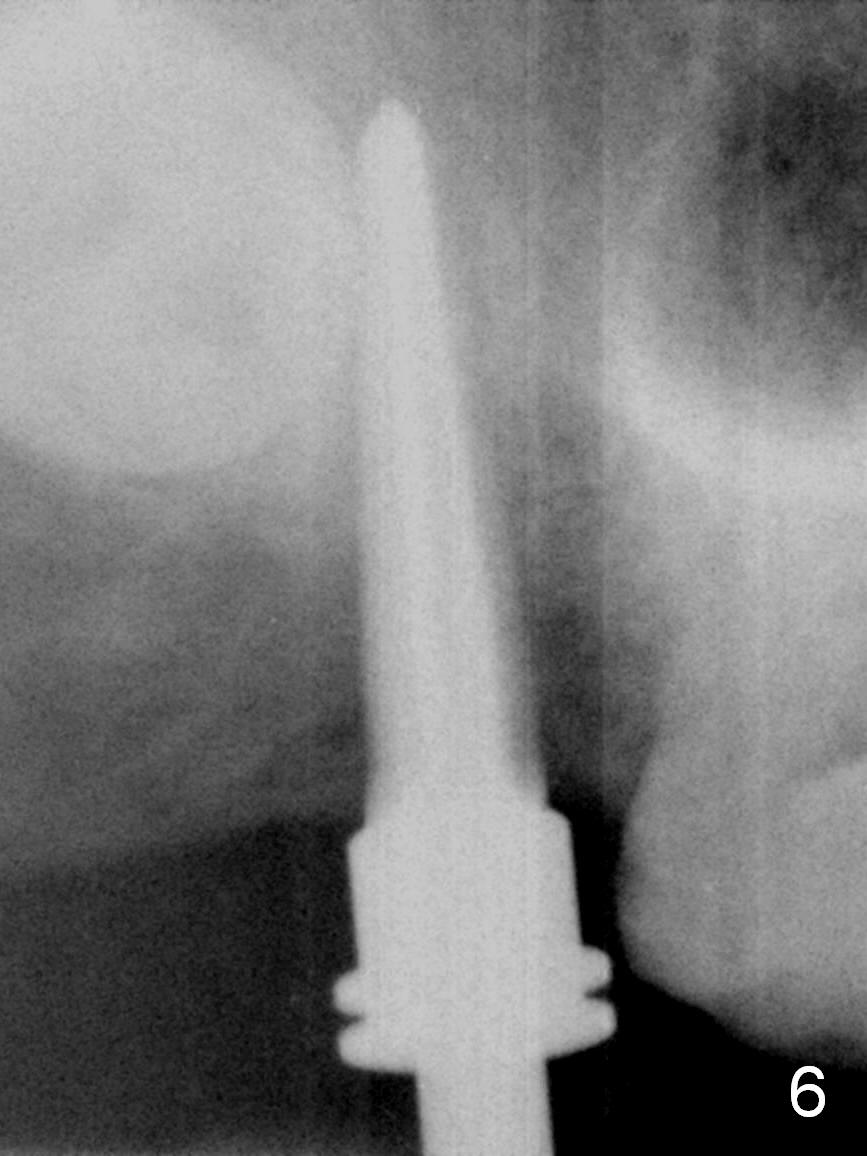
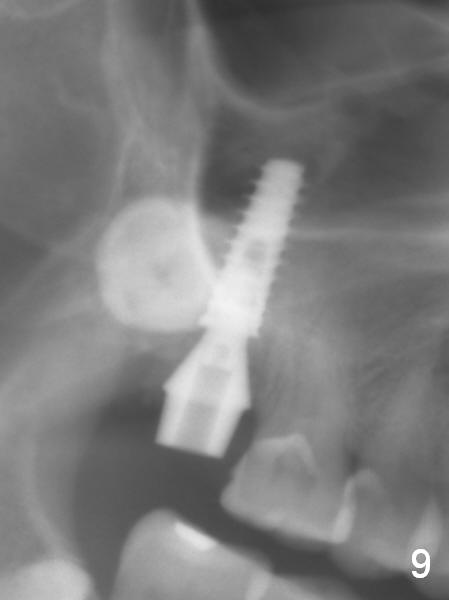
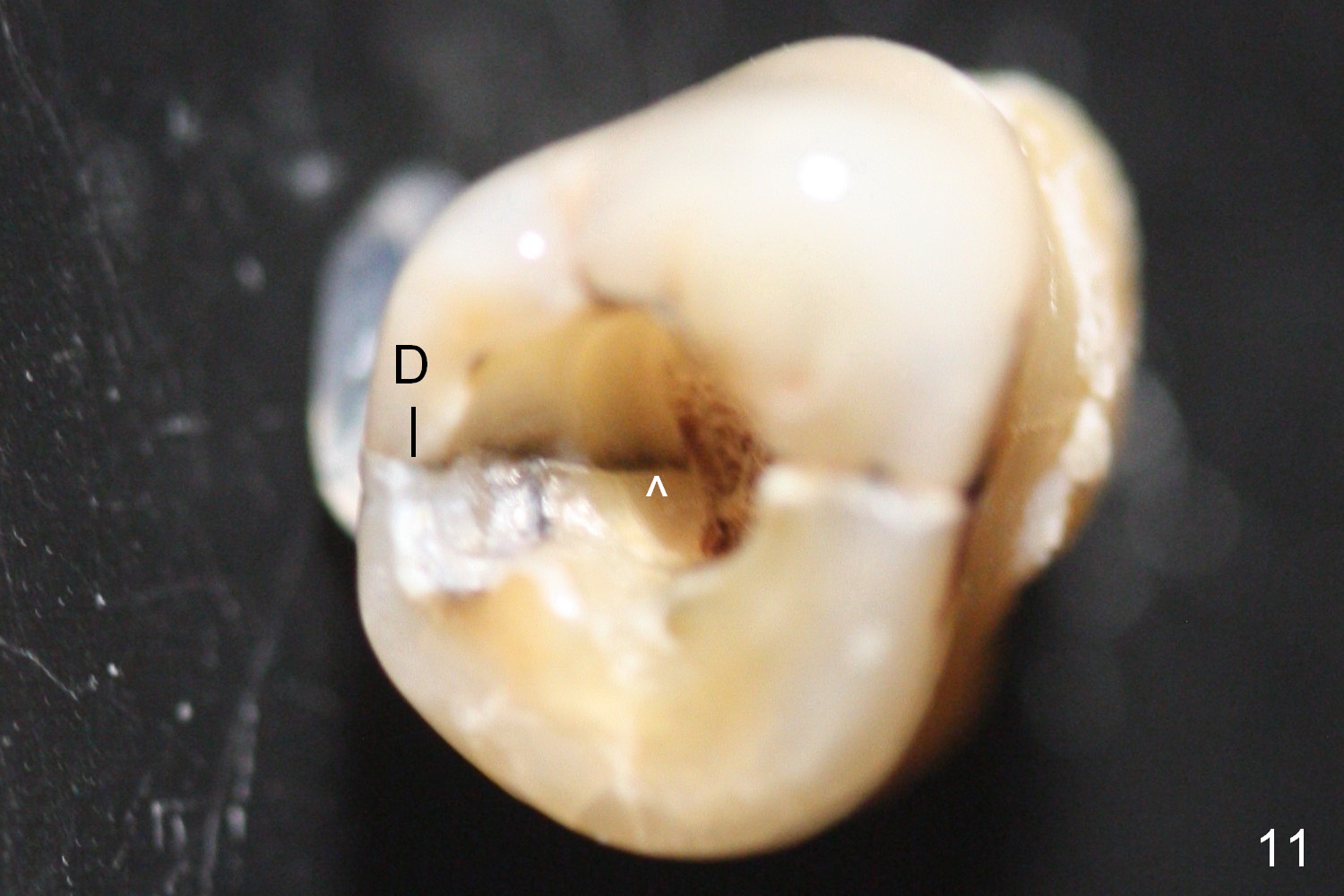
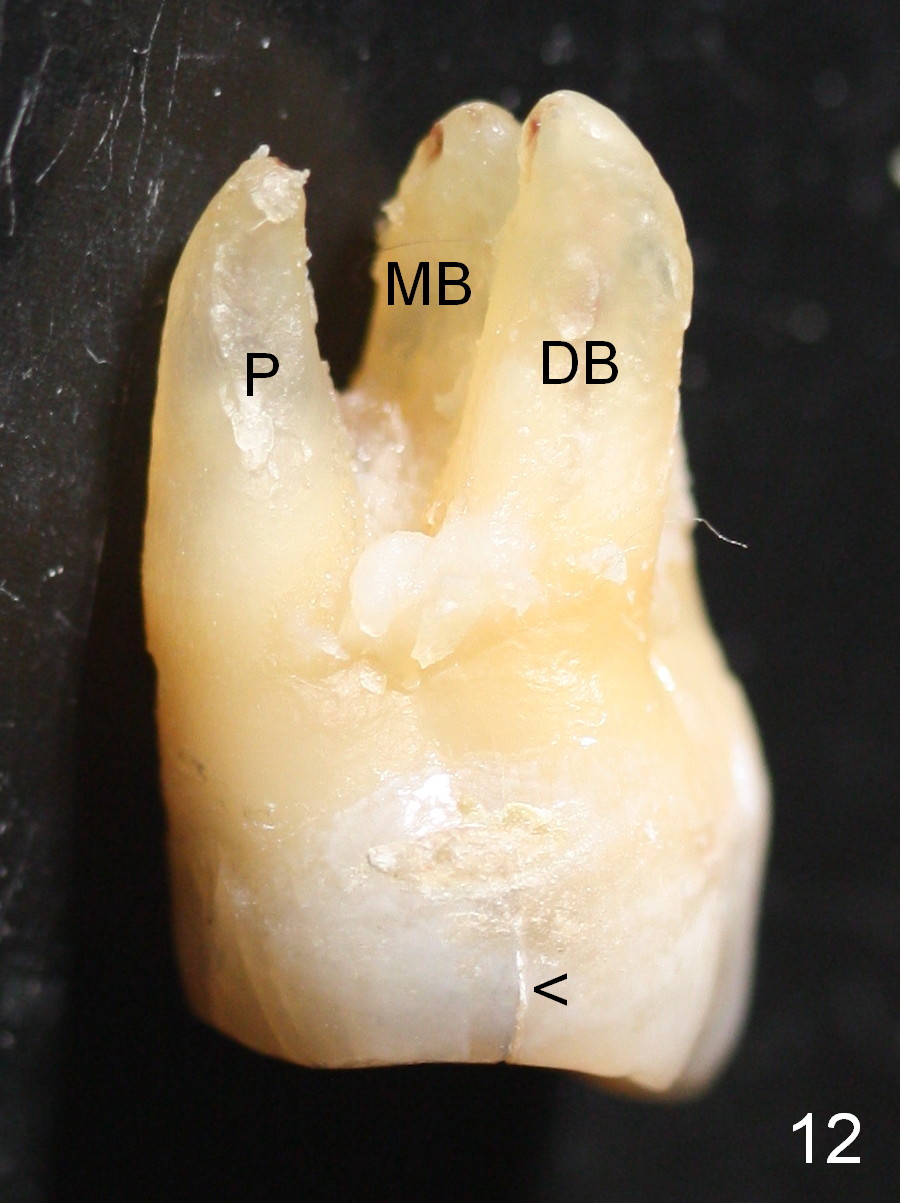
Extraction confirms crack tooth at #2 (Fig.1 (mesial view) <). The buccal (Fig.2 (illustration) B) socket is larger than the palatal (P) one, while the septum (S) is small. Osteotomy is initiated on the buccal slope of the septum (Fig.3 red arrow), followed by Magic osteotomes (Fig.4-7). As the diameter of the osteotomes increases, so does the depth with sinus lift (Fig.5 arrow). The largest osteotome is 4.8 mm. When a 5x13 mm implant is placed, it has low torque (Fig.8,9). The implant resists lateral movement, but keeps turning. When a largest pair abutment with the longest cuff is placed (6.5x4(4) mm to hold an immediate provisional in place), it seems to turn with the underlying implant together for a half turn. Since the provisional is engaged into the distal undercut of the tooth #3 (while the acrylic is setting), it may increase the implant stability. Anyway, overprep in this case leads to low primary stability. For immediate implant, underprep is a must. For this case, the last osteotome should have been 4.3 mm (.7 mm (one or two size(s)) smaller than the implant). When the implant is found to have low torque value, remove it, place bone graft in the osteotomy site and surrounding socket for sinus lift as well and place the implant again. The primary stability should have been increased. Preferably, a larger implant should be used (5.5 mm). Fortunately there is nasal hemorrhage postop. Reexamination of the extracted tooth after being soaked in bleach for 2 days confirms that the mesial (Fig.10 M) and distal (Fig.11 D,12 <) crack lines extend intrapulpally (^).
Four weeks postop, the immediate provisional and the abutment are to be removed. With or without anesthesia, the implant is going to be un-torqued a few times. The pair abutment or a healing one will be placed. In fact, there is pain when the mobile pair abutment is being removed without anesthesia 4 weeks postop. An immediate provisional is refabricated to keep the abutment and implant in place.
When the patient returns again, the abutment and implant will be removed with local anesthesia. Check whether the sinus membrane is perforated or not. Repair the perforation with collagen plug saturated with Metronidazole. Place allograft before insertion of 5.3 mm Magic Osteotome and a larger implant (6 or 6.5 x11 or 13 mm).
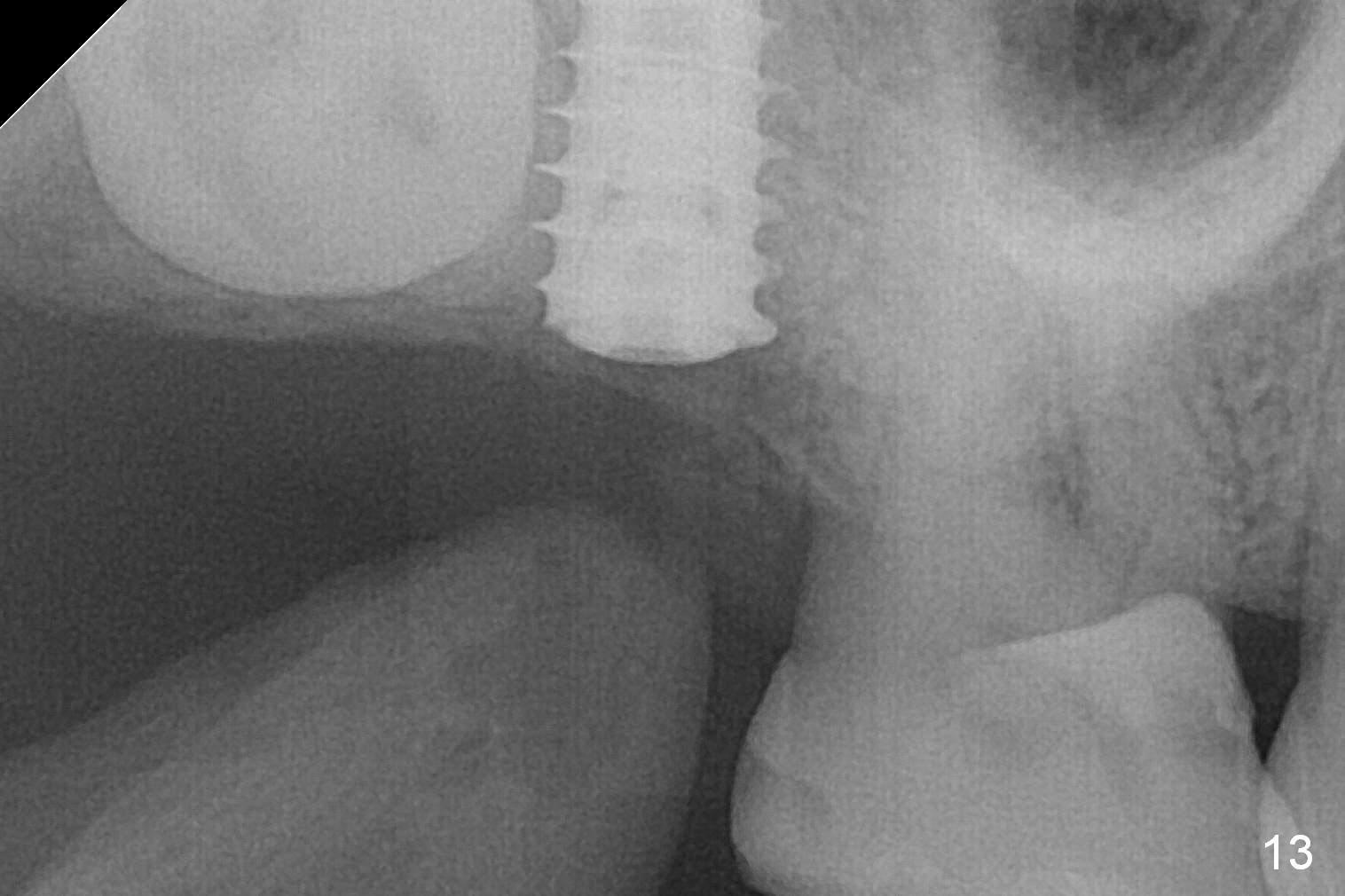
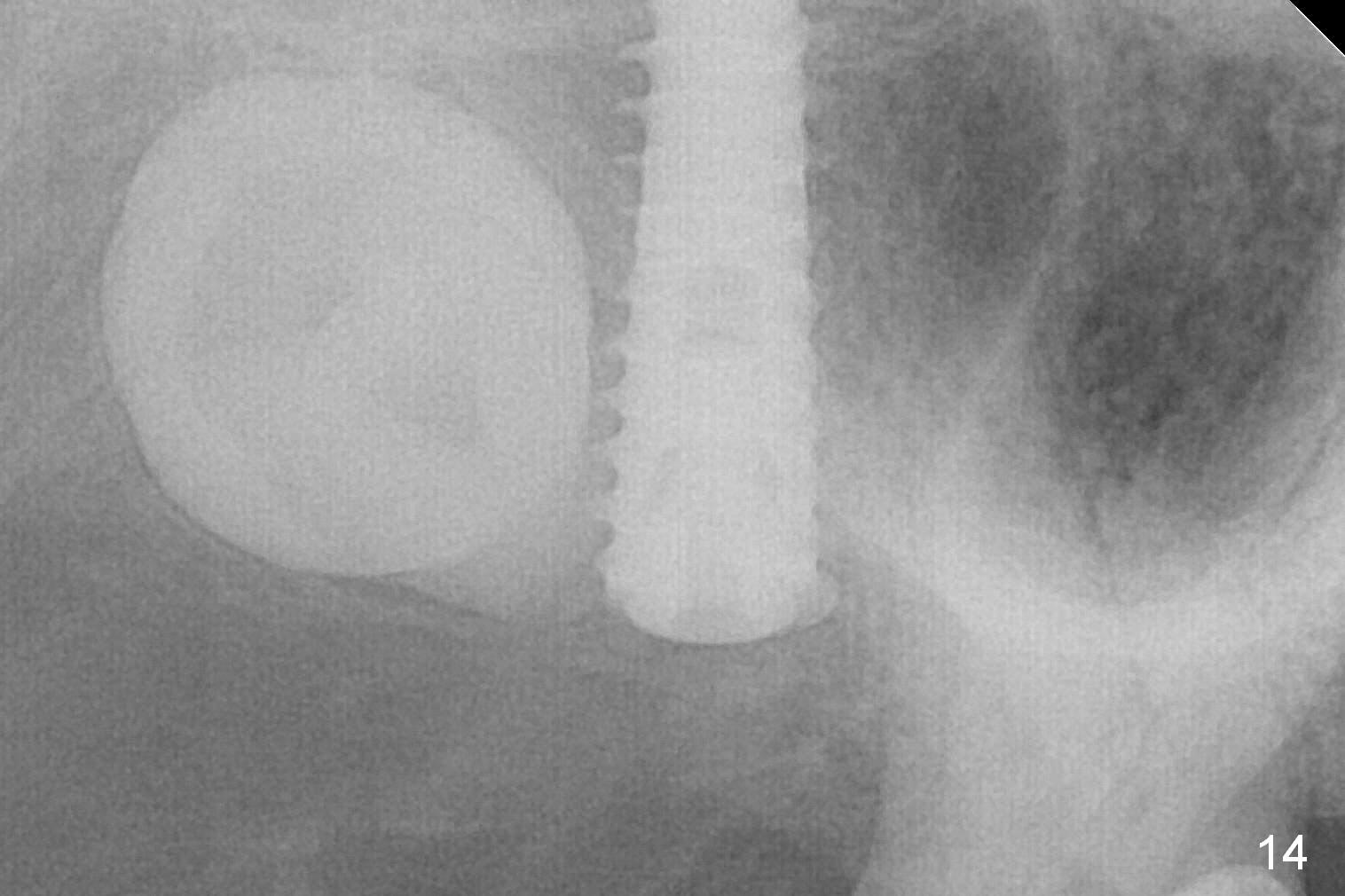
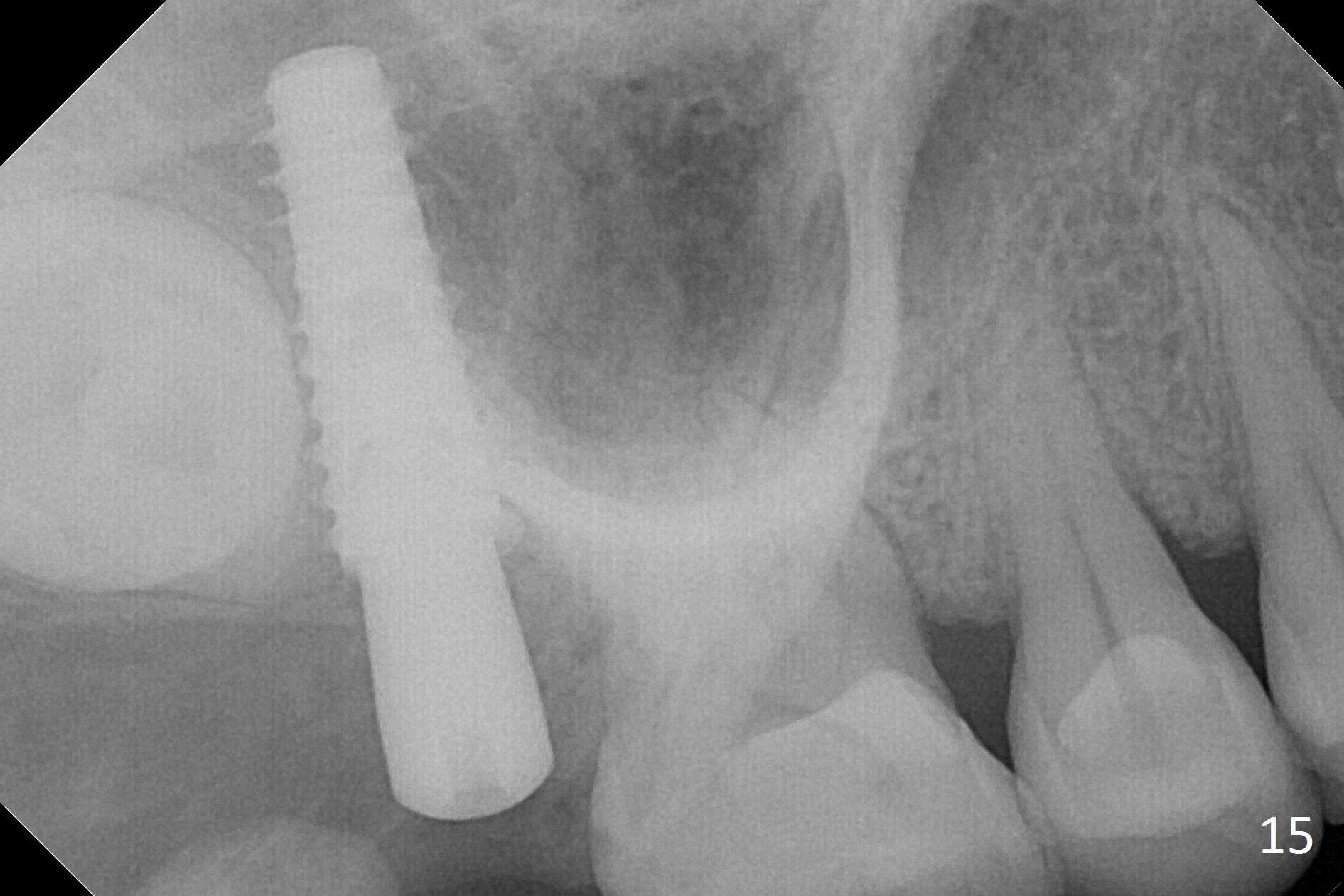
In fact, the implant is reversely torqued (1 month postop) and ~ 2 mm more coronally. It becomes looser. A healing screw is placed. With insertion of collagen plug, sutures are placed. Five days postop, the wound appears to be healing with sutures being dissolved. Four months later (5 months post placement), the patient returns asymptomatic. The wound heals. The implant appears to have osteointegrated and is at the crestal level (Fig.13,14). At uncover, the implant is found unstable; a healing abutment is placed. The implant is stable 8 months postop with apparently no gap between the bone and threads (Fig.15, as compared to Fig.13).
Orthodontic extrusion may be an option.
Return to
Upper
Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table), IBS,
#14
Xin Wei, DDS, PhD, MS 1st edition 08/25/2016, last revision 07/28/2017