|
|
|
|
|
|
|
7 mm Fixture
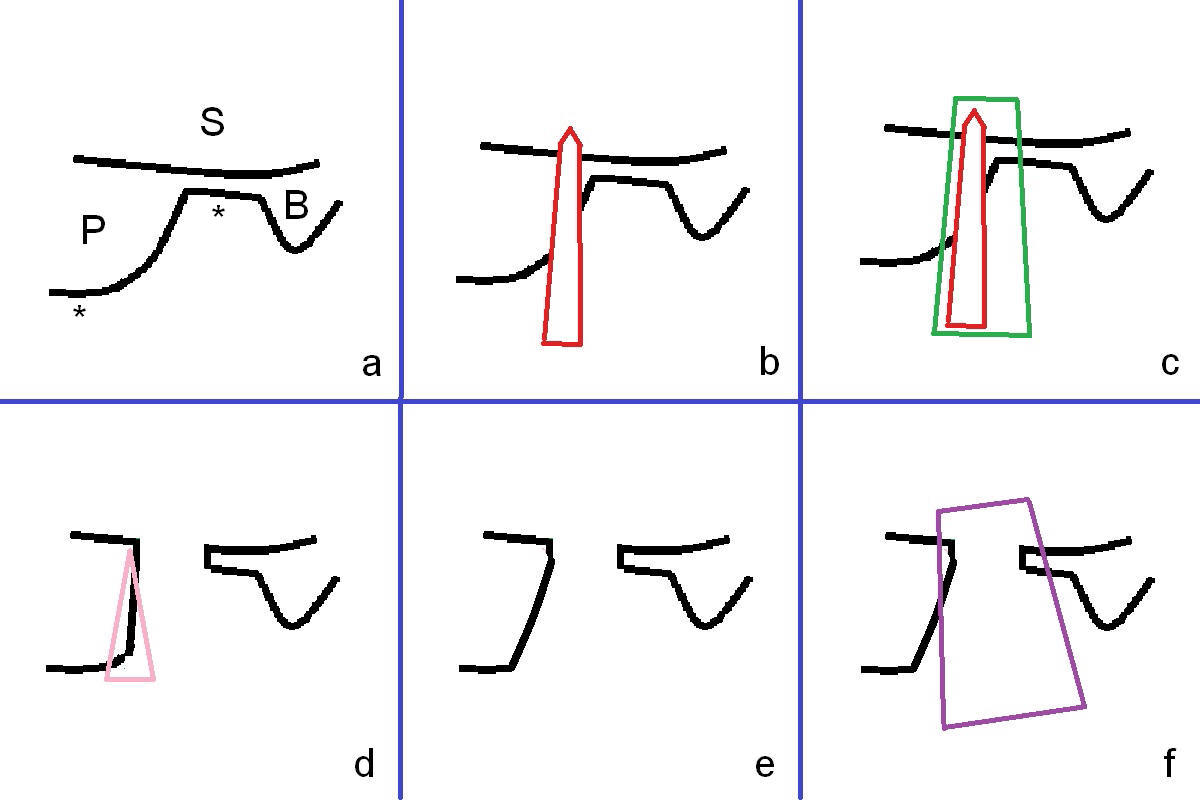
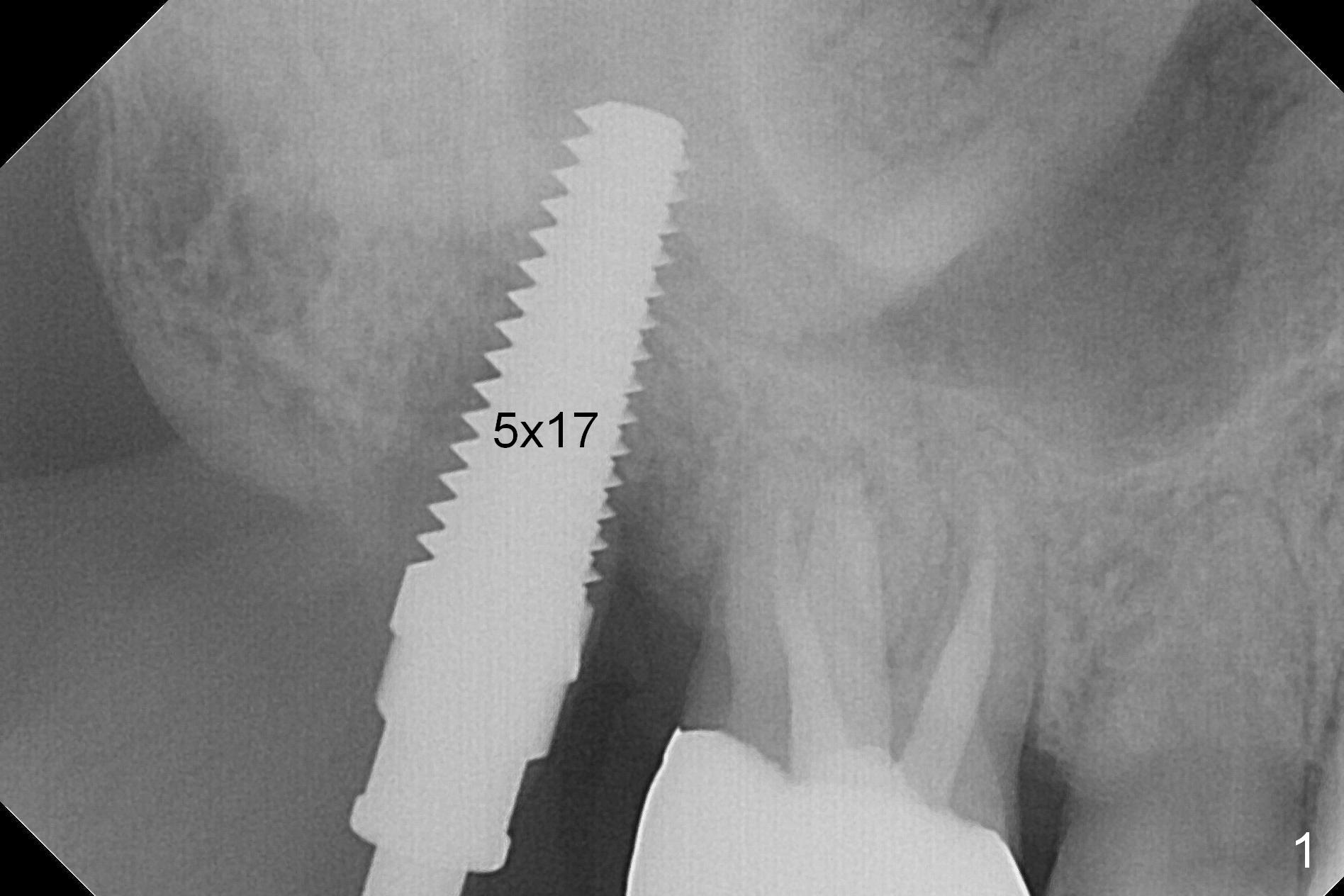
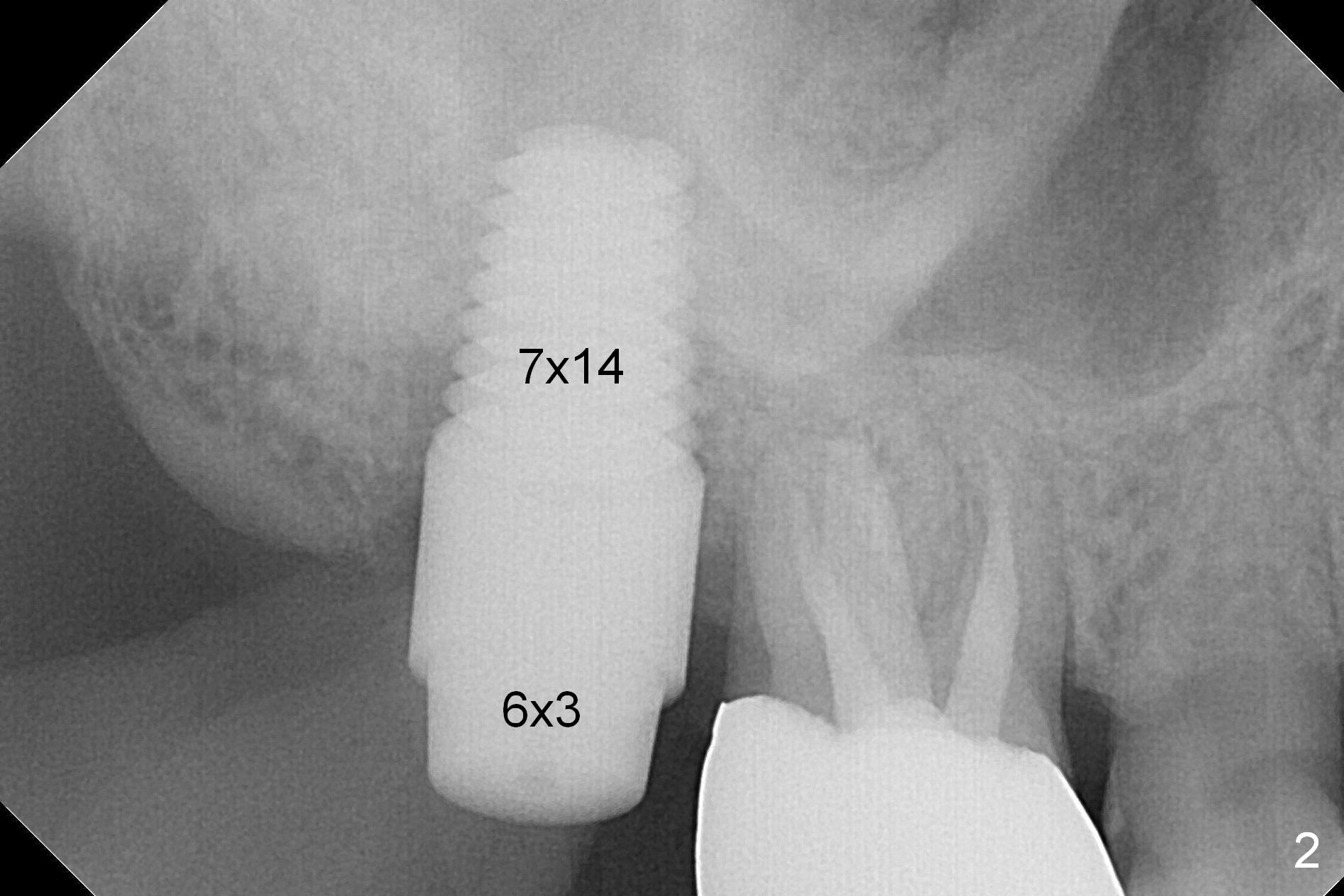
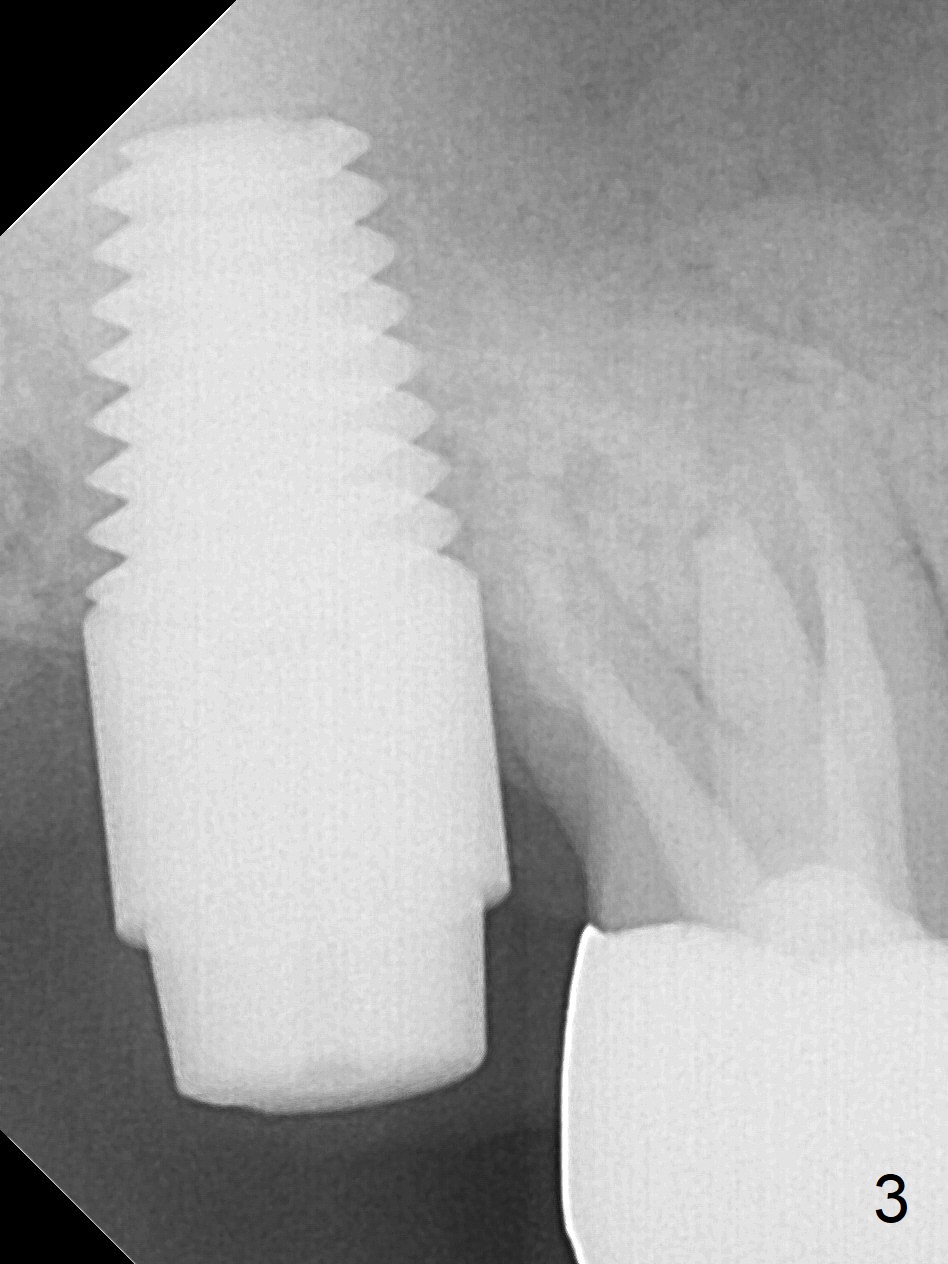
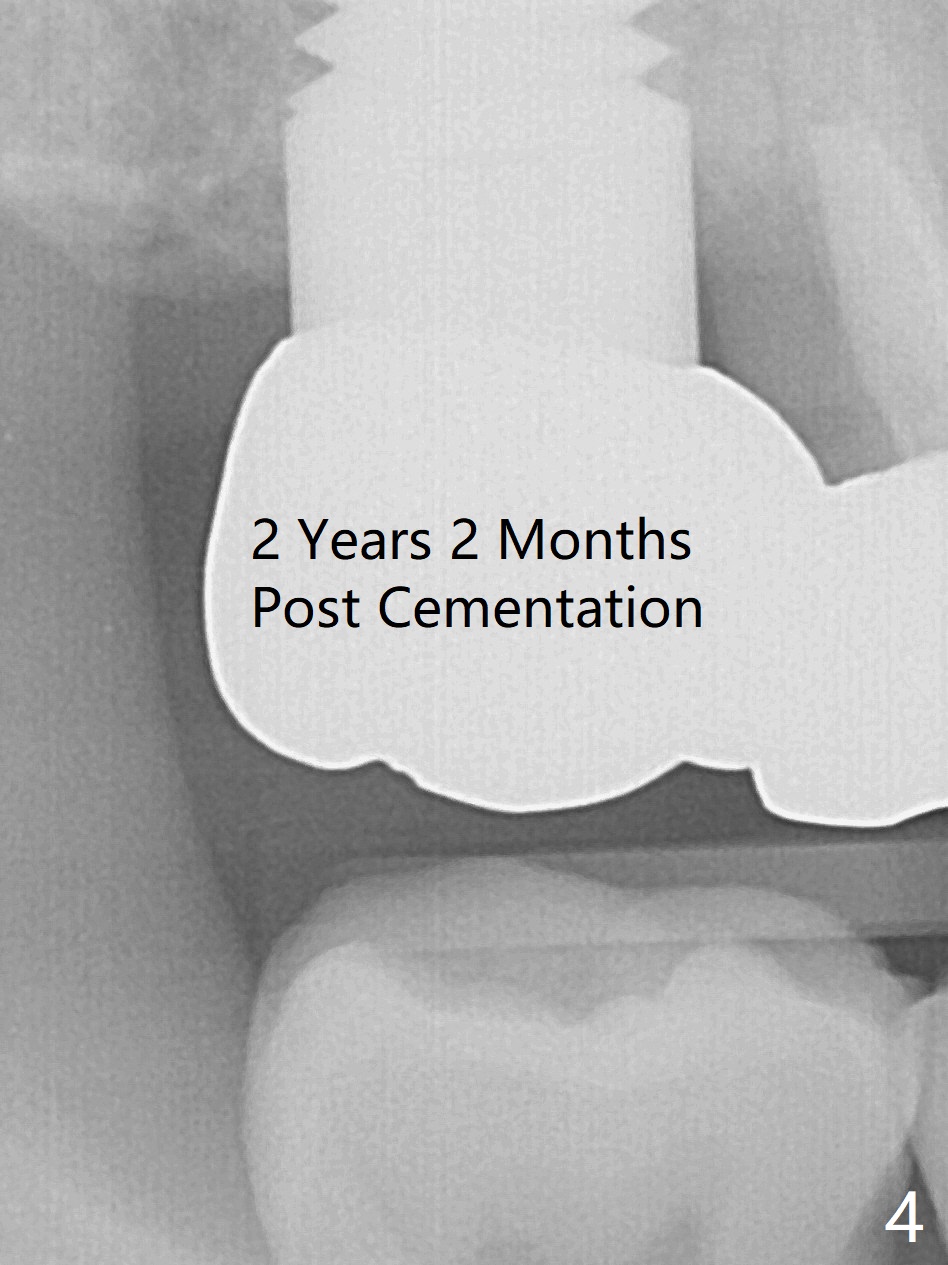
The tooth #2 is found to have fracture at extraction. The buccal (B) socket (*) has more resorption than the palatal (P) one (Fig. A (S: sinus). The buccal plate is also lower. Osteotomy is initiated in the buccal slope of the septum with Magic Expanders (ME, 3-4.8 mm, Fig. B (red)), followed by Tatum tapered tap drills (Fig. C (green), Fig.1 (5x17 mm)). As the diameter of ME and tap increases, the osteotomy is shifting buccally due to bone height discrepancy (Fig. C). A Lindamann bur is used to remove the palatal bone (Fig. D (pink) and move the osteotomy palatally (Fig. E). The coronal end of 7x14 mm tissue-level fixture (Fig.2) tilts buccally (Fig. F purple). Insertion torque is 35/40 Ncm. Prior to implantation, a piece of PRF membrane and allograft are pushed into the sinus. A 6x3 mm abutment (Fig.2) is immediately placed to keep an immediate provisional, bone graft and collagen membrane in place. Bone seems to have grown into the space between the implant threads 5.5 months postop (Fig.3). There is no bone loss 2 years 2 months post cementation (Fig.4).
Return to Upper Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), IBS Xin Wei, DDS, PhD, MS 1st edition 01/31/2017, last revision 10/02/2019