|
|
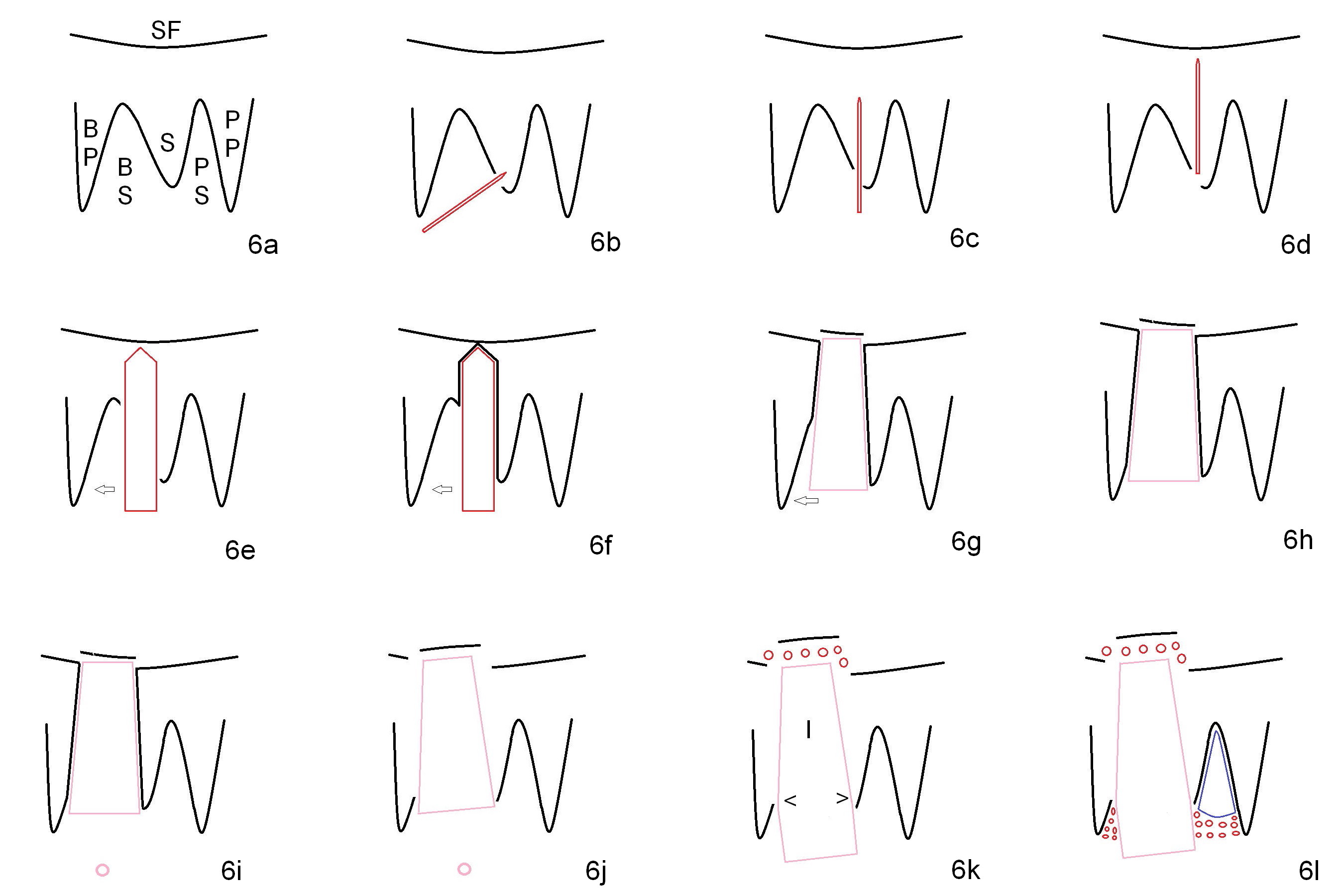
The buccal roots are fused. The buccal socket (BS) seems to be larger than the palatal one (PS). There is a septum (S) between the 2 sockets. Both the buccal and palatal plates (BP, PP) are intact. The anatomy is illustrated in Fig.6a (buccopalatal section) with the same abbreviations, mentioned above. SF: sinus floor.
Osteotomy for immediate implant is initiated with a 2 mm pilot drill (Fig.6b red arrow) in the coronal end of the buccal slope of the septum (center of the socket). Once the drill gets initial penetration, the trajectory changes to the long axis of the tooth (Fig.6c). The osteotomy is deepened (Fig.6d). As drill diameter increases, they deviate buccally (Fig.6e arrow), since there is less bone contact buccally than lingually (compare Fig.6e,f). With the same reason, smaller tapered taps (Fig.6g pink, 5 and 6 mm) tend to be mobile buccally (arrow). When a large tap (7 mm) is inserted, there is no buccal mobility. It appears that the tap contacts more of the buccal plate (Fig.6h), but the coronal end of the tap is buccal (Fig.6i, pink circle). At each step of osteotomy, the coronal end of a bur or tap should be pushed as lingual as possible so that the final tap is favorable for restoration (Fig.6j). Sinus lift is done (Fig.6k red circle) before placement of 7x17 mm implant (I). Arrowheads in Fig.6k point to the most coronal thread. Since the palatal socket is not associated with implant stability, it is closed by collagen plug (Fig.6l, blue area). As extra precaution, bone graft is placed around the coronal portion of the tissue-level implant (Fig.6l red circles), followed by collagen dressing.
Xin Wei, DDS, PhD, MS 1st edition 02/20/2015, last revision 02/22/2015