







|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
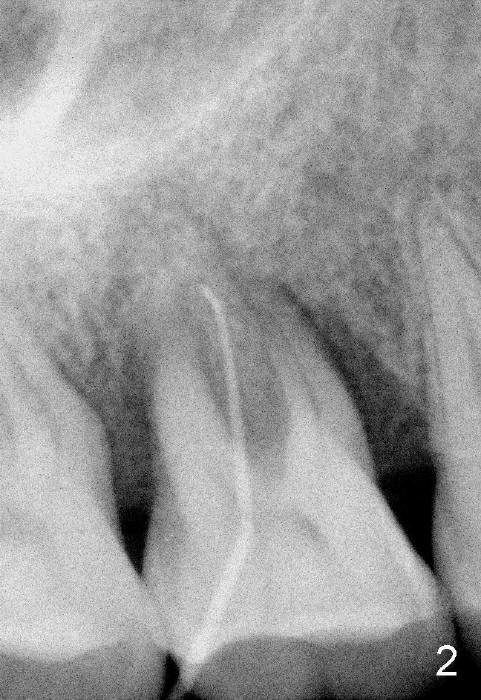
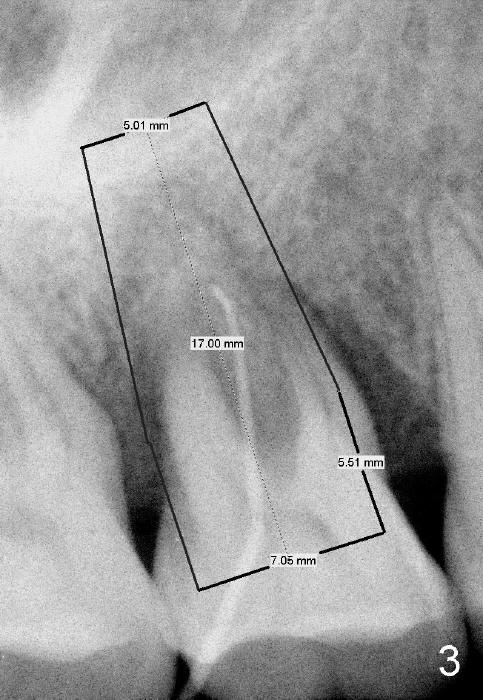
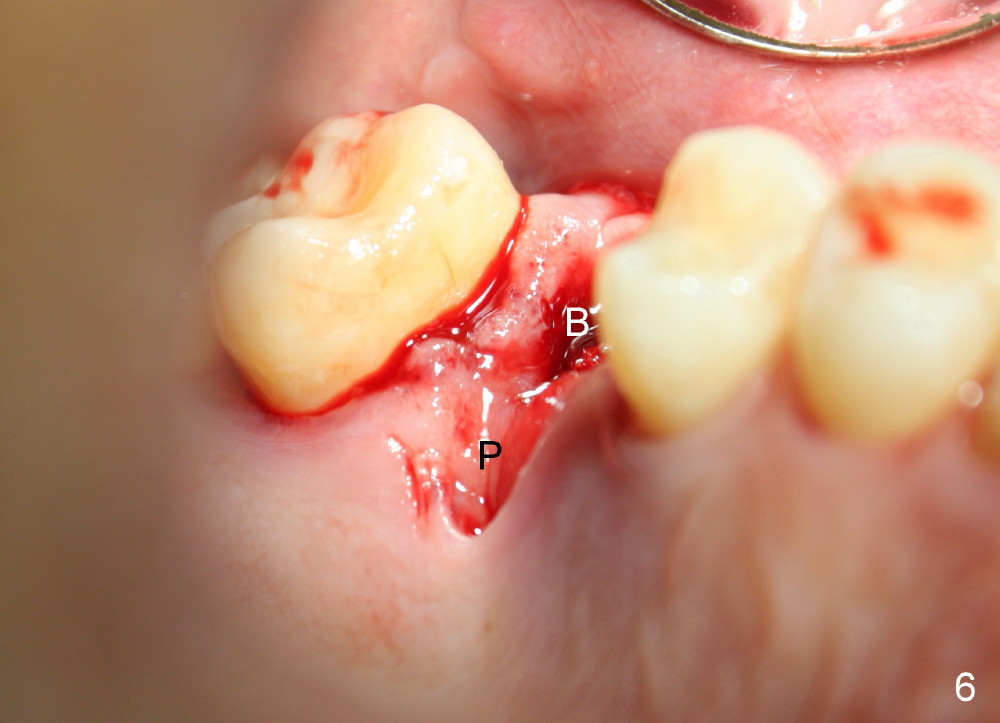
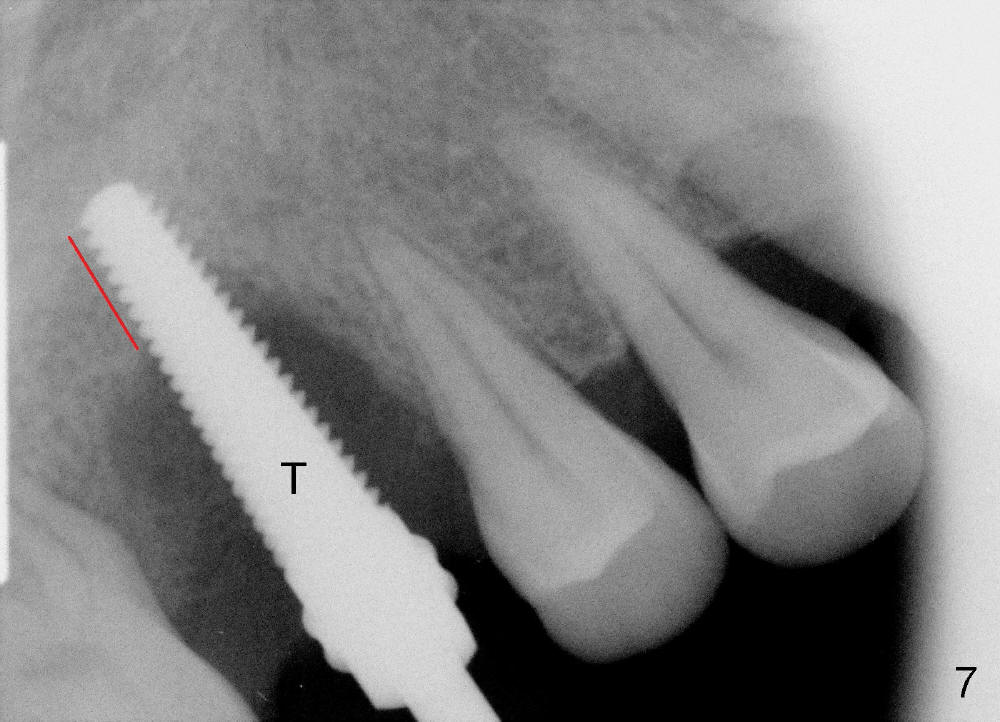
Why Needs a Large Immediate Implant for An Upper Molar?
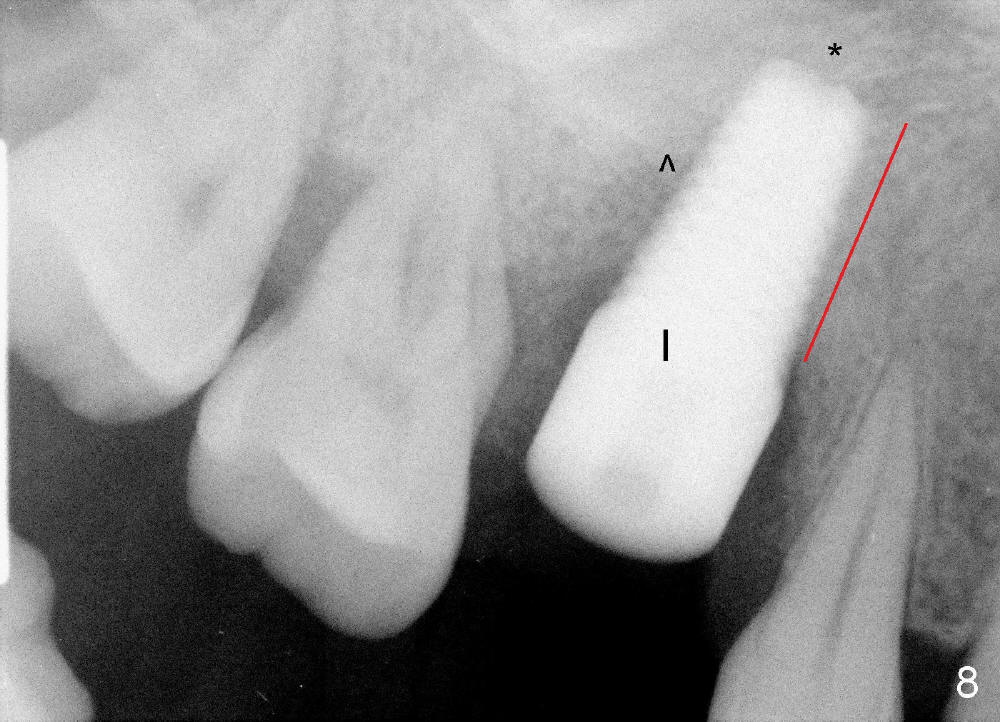
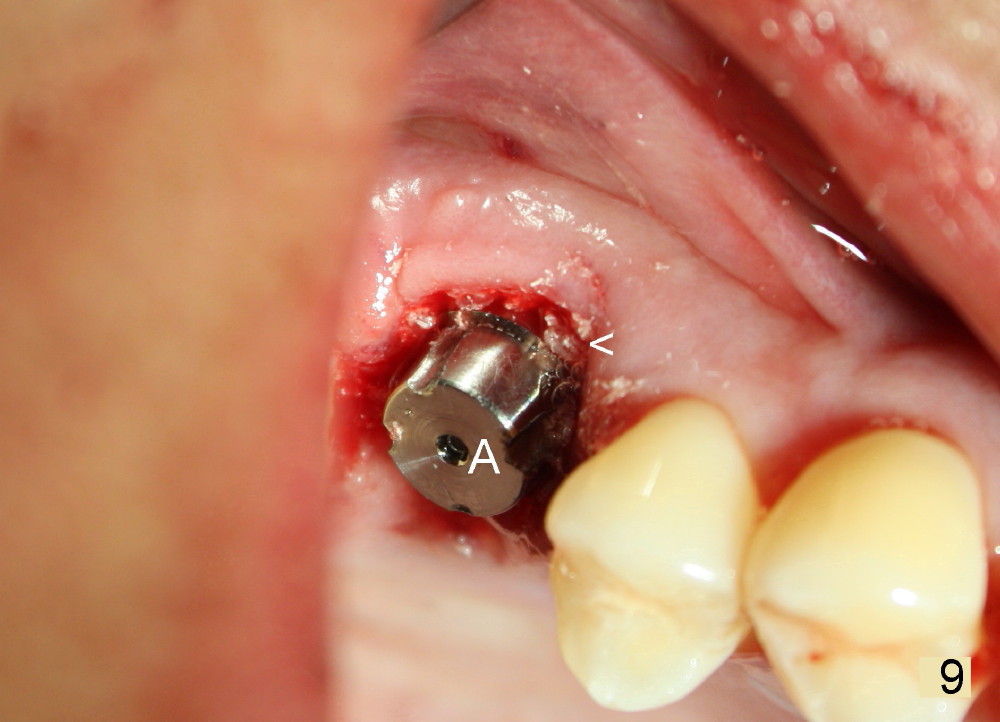
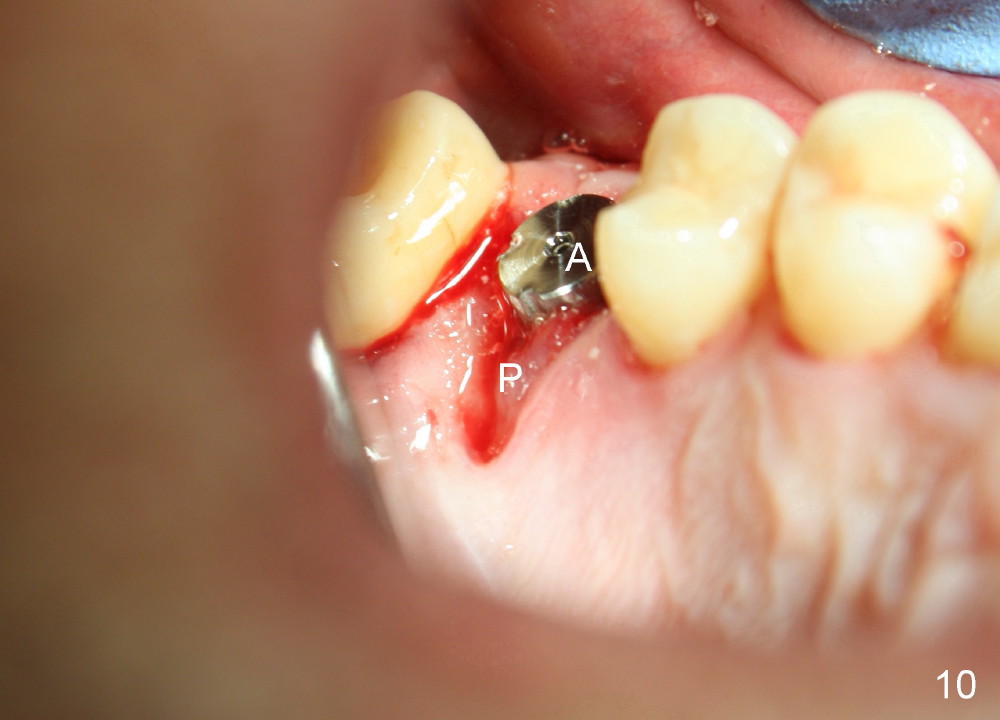
The tooth #3 has severe periodontitis with probably endodontic lesion (Fig.1,2). The patient is a 43-year-old man with apprehension of dentistry. An acute infection causes pain and tooth shift (Fig.4,5). A 7x17 mm immediate implant is planned (Fig.3). The palatal socket is shallow (Fig.6 P), corresponding to severe recessive palatal root (Fig.5 P). The osteotomy is created mainly in the buccal socket (Fig.6 B), exactly in the lingual slope of the septum. Initially osteotomes are used, followed by tap placement (Fig.7 T (4.5x20 mm at the depth of 17 mm). When the implant is placed as planned (Fig.8 I), there is more vertical contact (Fig.8 red line) than that associated with the tap (Fig.7 red line). The corresponding insertion torque is between 50 and 60 Ncm. There is only one small gap buccally, which is filled with bone graft (Fig.9 <). After the insertion of a short abutments with vertical slots (Fig.9,10 A), perio dressing is used to cover the wound. The palatal socket is expected to heal uneventfully (Fig.10 P). In fact, it does in 7 days (Fig.12 P); the bone graft in the mesiobuccal aspect is healing and stabilized (Fig.11 <). By two weeks postop, the mesiobuccal socket has healed (Fig.13 <). With removal of a diseased tooth, our body has amazing power to heal.
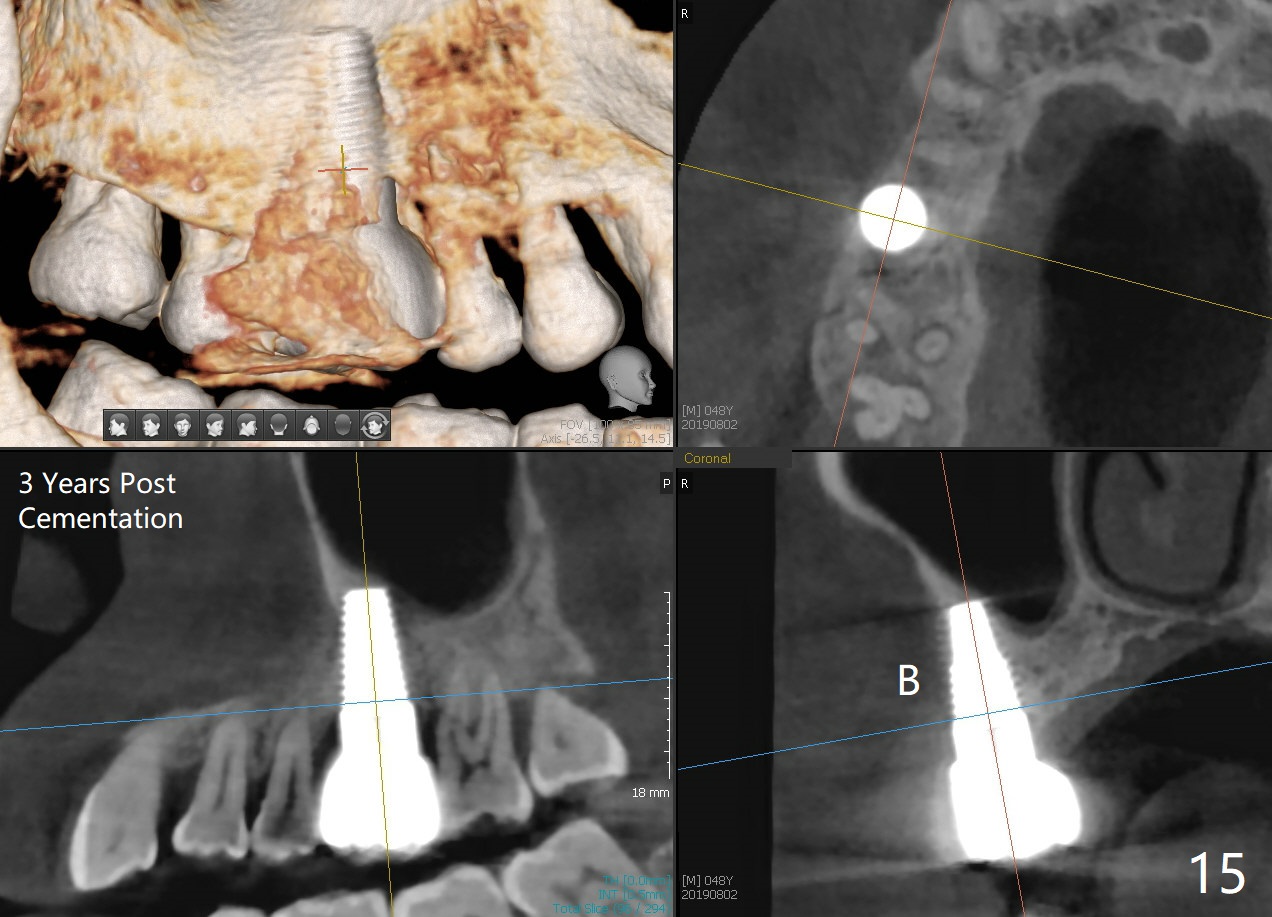
The patient returns for restoration 23 months postop; the implant appears to have been osteointegrated (Fig.14). There is no buccal or palatal gingival recession. The large implant appears to close the large defect readily and enhances bone/implant contact. The buccal plate seems to be thin 3 years post cementation, although there is no sign of periimplantitis (Fig.15). The mesial papilla is severely recessive with open contact 3 years 5 months post cementation. BW shows DO caries of the teeth #2, 4 and 30. The crown is removed for better oral hygiene by fabricating a provisional and conservative composite for #4. Water Pik is recommended.
Return to
Upper Molar Immediate Implant
14
Placement
Xin Wei, DDS, PhD, MS 1st edition 07/02/2014, last revision 01/24/2020