|
|
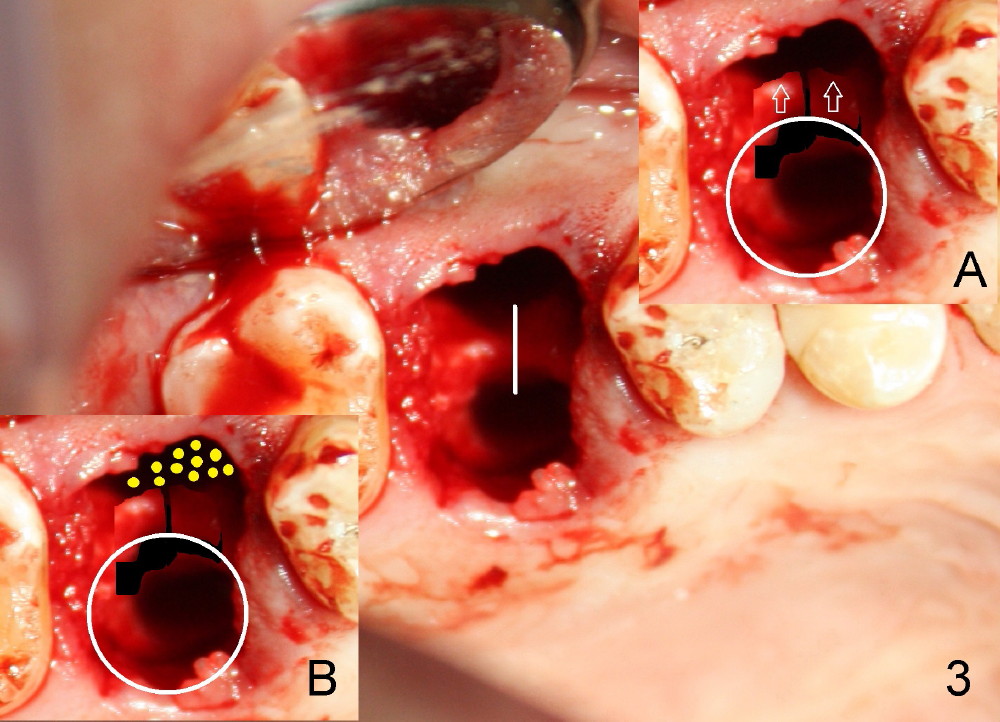
It would be ideal to move the apical end of the implant buccally to certain degree. In order to do that, the septum is sectioned buccolingually (Fig.3 white line) with a series of blade shaped osteotomes (bone scalpel, bone blade, D shaped spreaders, Tatum Surgical). Probably due to extensive apical bony lesions in the buccal and palatal sockets, sectioning with the osteotomes is relatively easy, approximately 17 mm deep. The osteotomy is initiated in the palatal socket by using a 7x17 mm tap manually. It appears that the sectioned septum undergoes further fracture and are pushed buccally (Inset A: arrows) while the tap is screwed in (white circle). A second associated advantage of the bone expansion is narrowing the buccal socket. The septum is assumed to be further pushed buccally when a 8x17 mm tap and its corresponding implant are being inserted. Prior to implant placement, approximately 1 cc allograft is placed in the remaining buccal socket (Insert B: yellow circles).
Return to Split Septum for Implant Last Next
Xin Wei, DDS, PhD, MS 1st edition 02/12/2014, last revision 07/14/2018