











|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
Never Too Easy
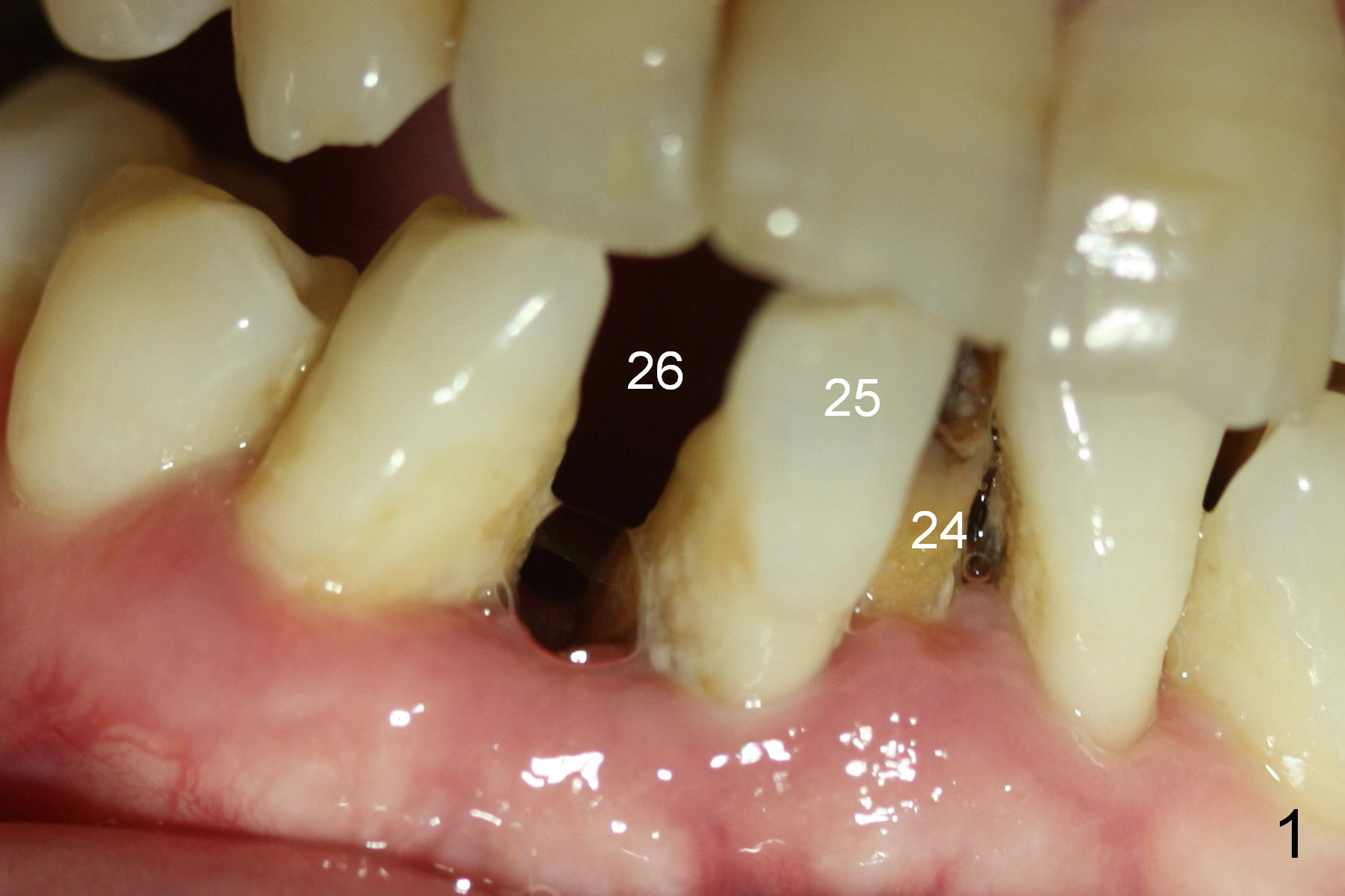
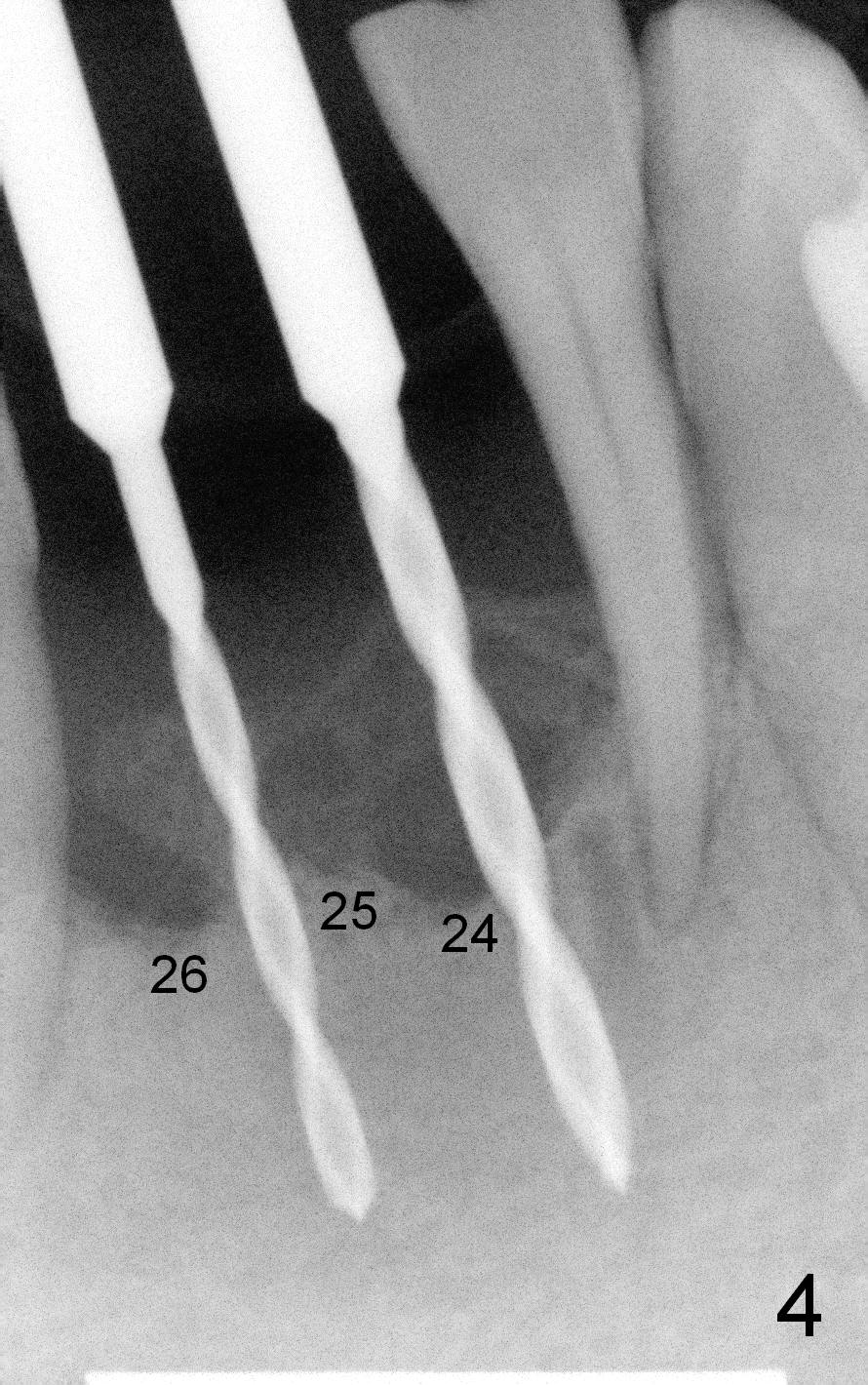
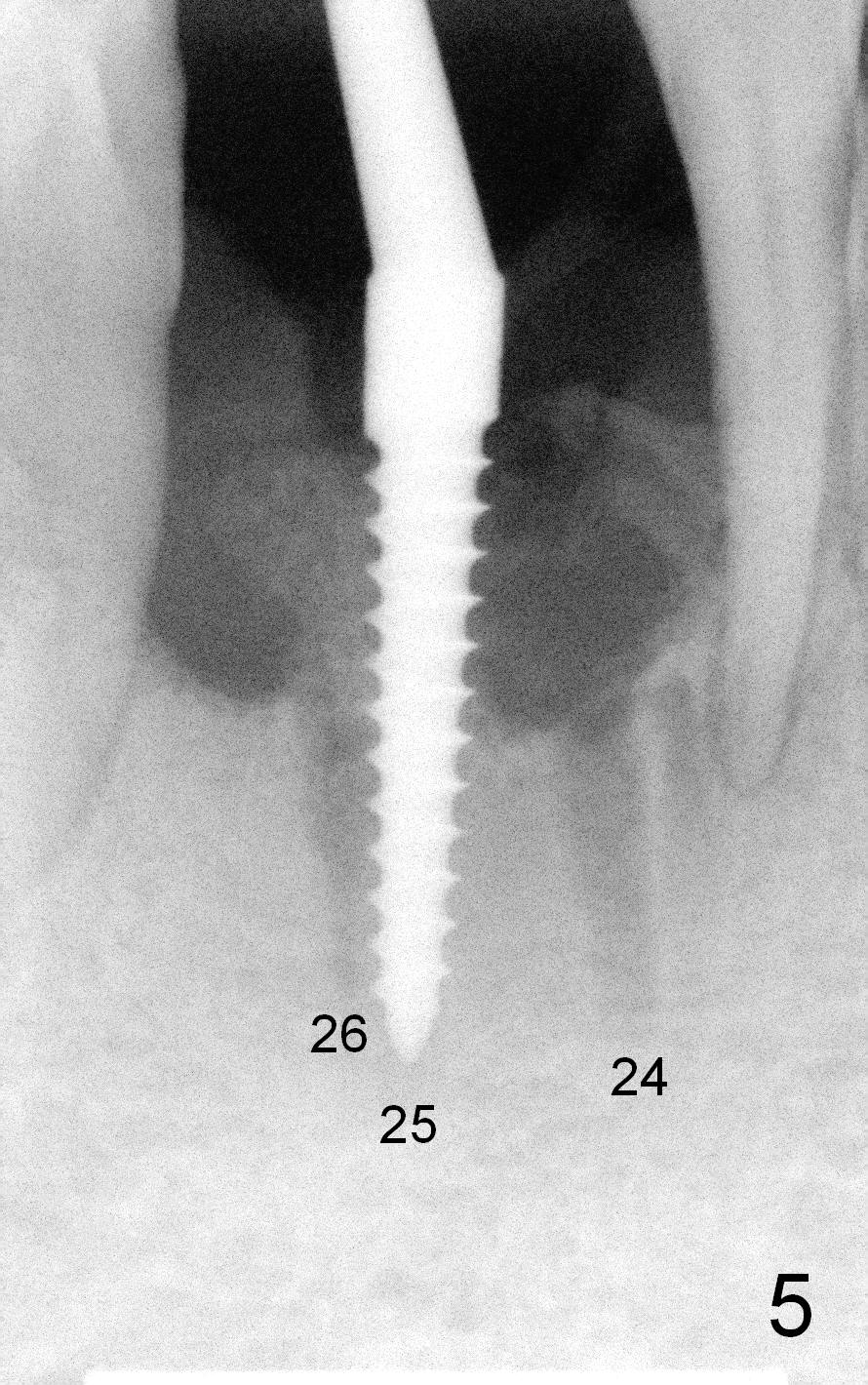
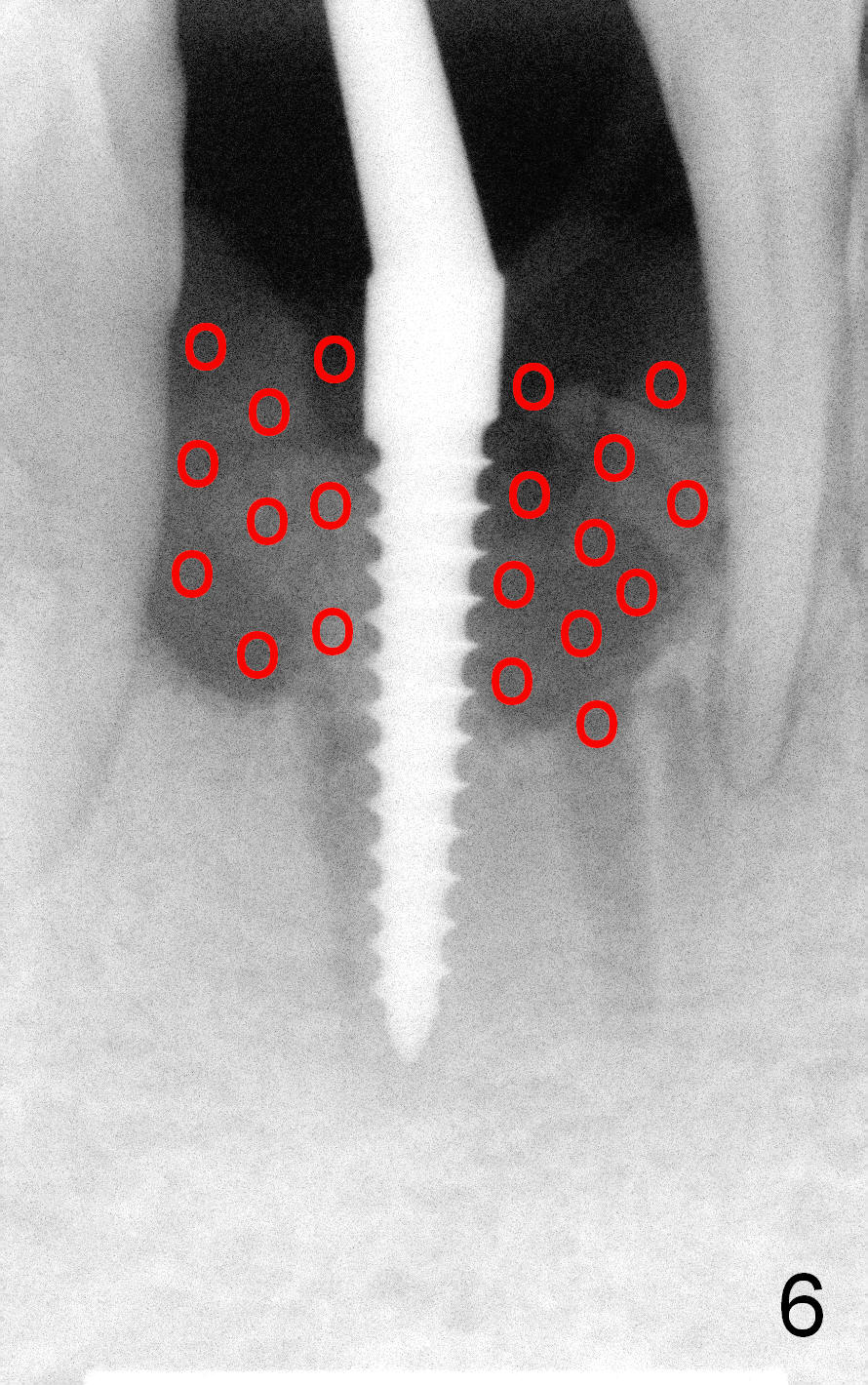
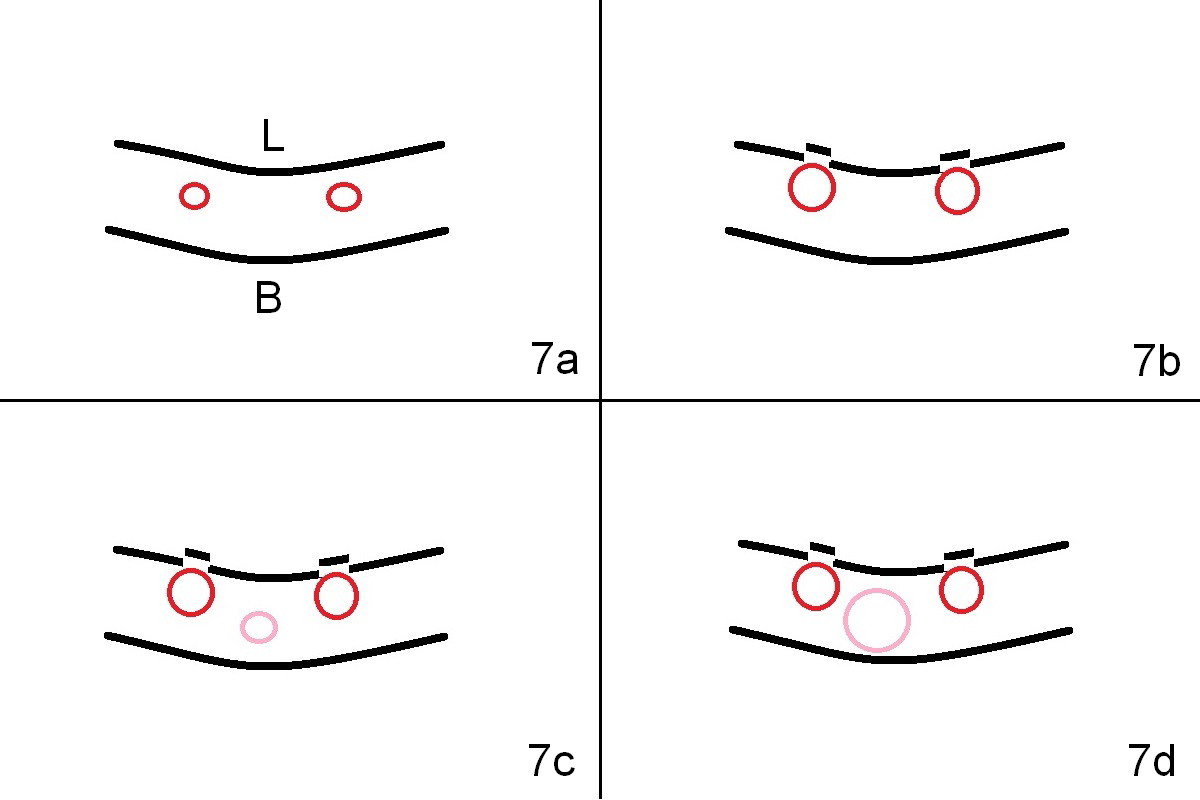
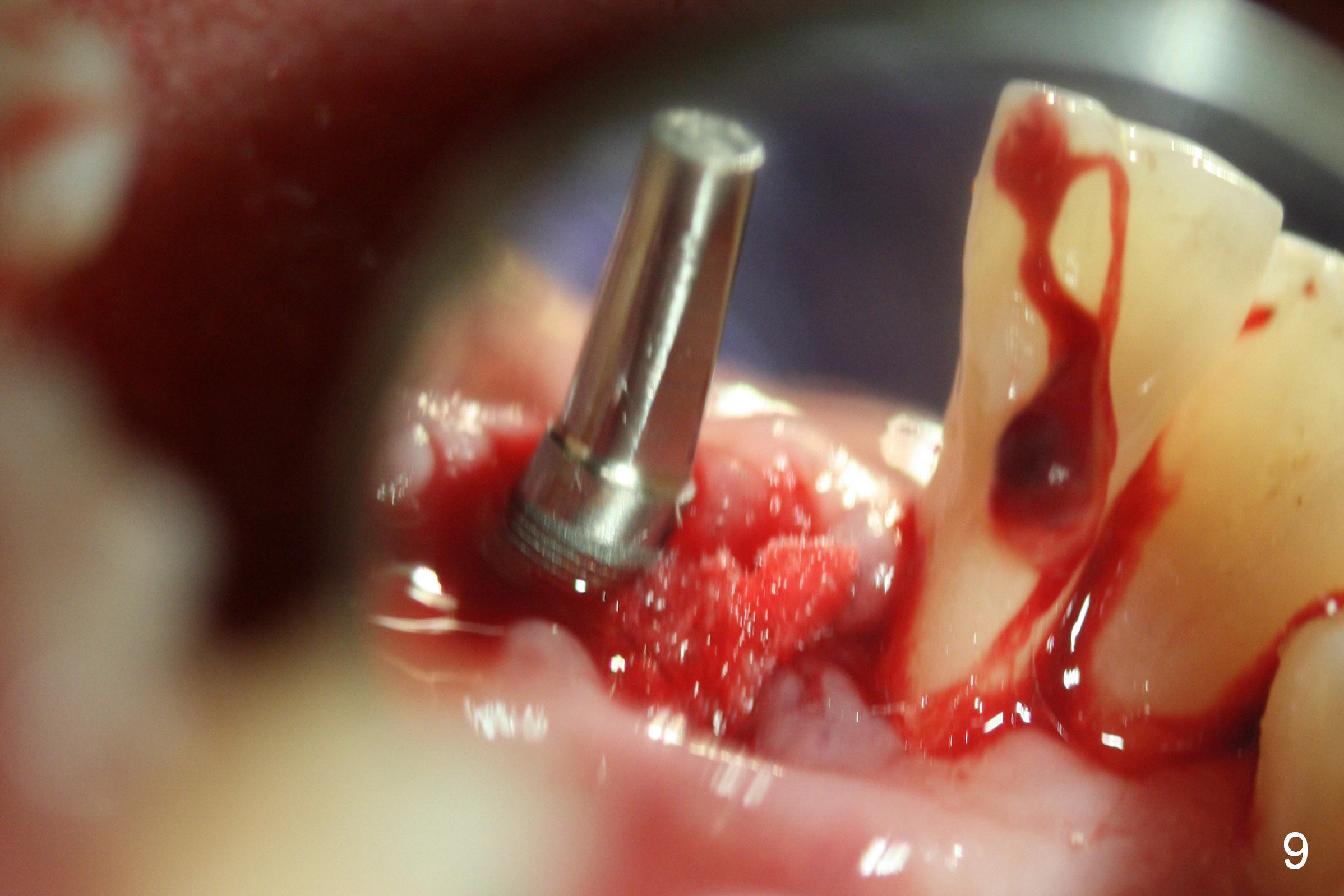
A 63-year-old lady is a dental phobic, returning to clinic because the tooth #26 exfoliates lately and #24 and 25 have mobility III (Fig.1-3). It appears that 2 of 1-piece implants are a proper mode of treatment considering crowding in this area. Since the buccal (B) plate is thinner than the lingual (L) one, two of osteotomy are initiated lingually (Fig.4,7a). As the osteotomies increase in diameter and depth, the lingual plate starts to be perforated with hemorrhage (Fig.7b). Osteotomy is changed buccal and between the 2 previous ones (Fig.7c pink). When a 3x17 mm angulated (15°) 1-piece implant is placed (Fig.5,8,9), the buccal plate is thinner, but not perforated (Fig.7d). No attempt is tried to increase the length of the osteotomy to avoid buccal plate perforation. Bone graft is placed around the implant and over the roots of the neighboring teeth (Fig.6 red circles). An upper incisor crown form is used for an immediate provisional with a notch fabricated in the middle to simulate 2 lower incisors (Fig.10 I, 9 days postop). It appears difficult to place an implant in the lower incisor region due to limited buccolingual width particularly in a petit lady with a small mouth.
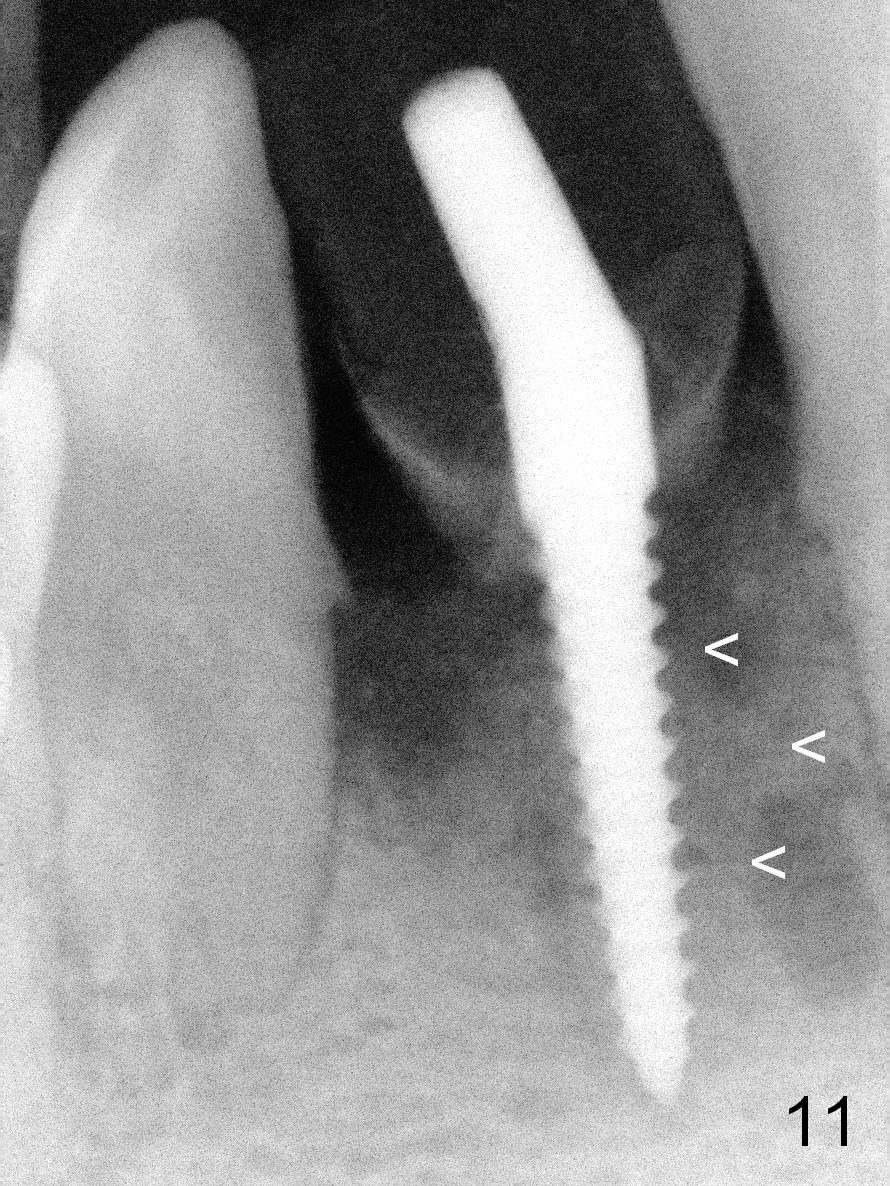
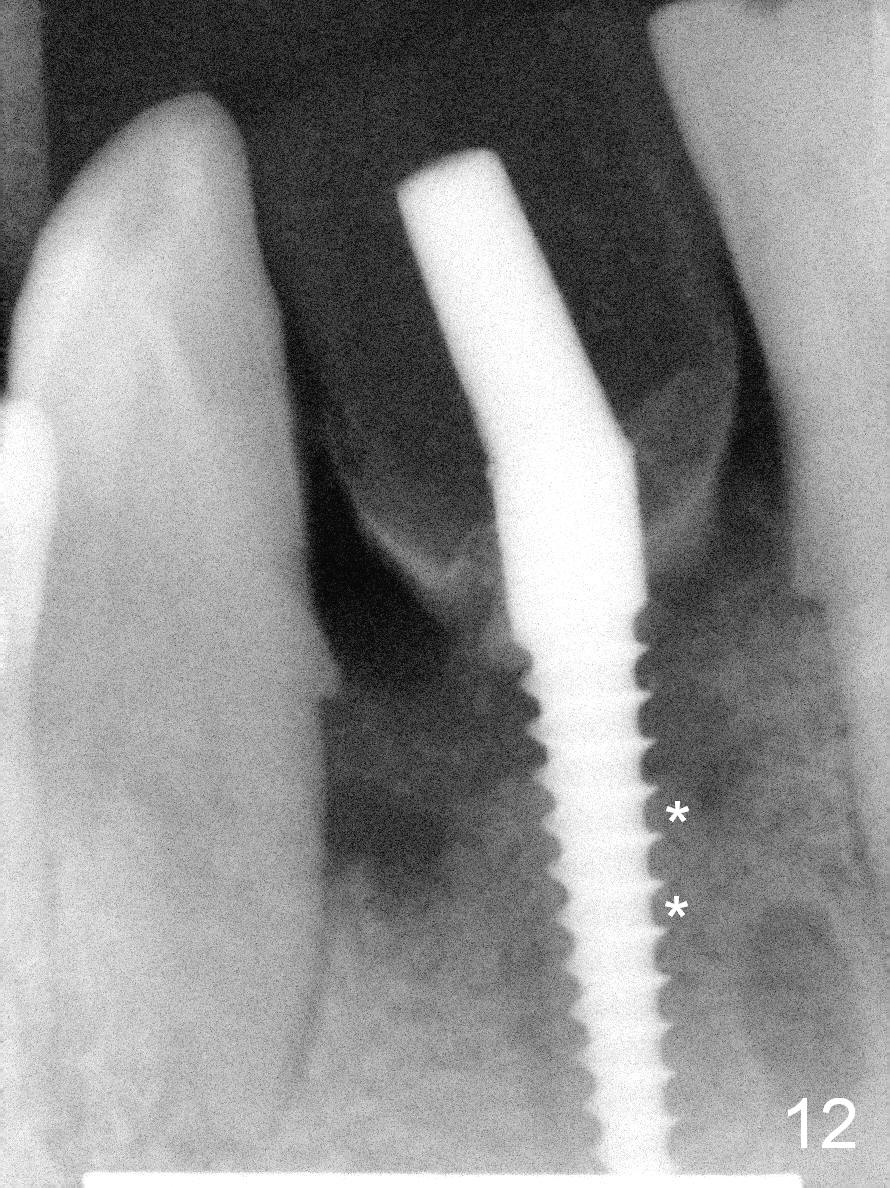
The patient returns for final restoration 7 months postop. There is bone growth mesially (Fig.11,12 arrowheads or *). The margin is prep equigingival buccally and supragingival lingually (Fig.13); two incisors are to be fabricated (Fig.13 I). The margin of the 2 provisional crowns is intentionally trimmed short so that the gingival infection may resolve after improved oral hygiene. The margin of the final restoration should extend as gingival as possible buccally; the embrasures are to be closed as much as possible; the cervical triangle could be pink porcelain or shade could be darker, e.g., A3.5 (Fig.14, as compared to Fig.15,16).
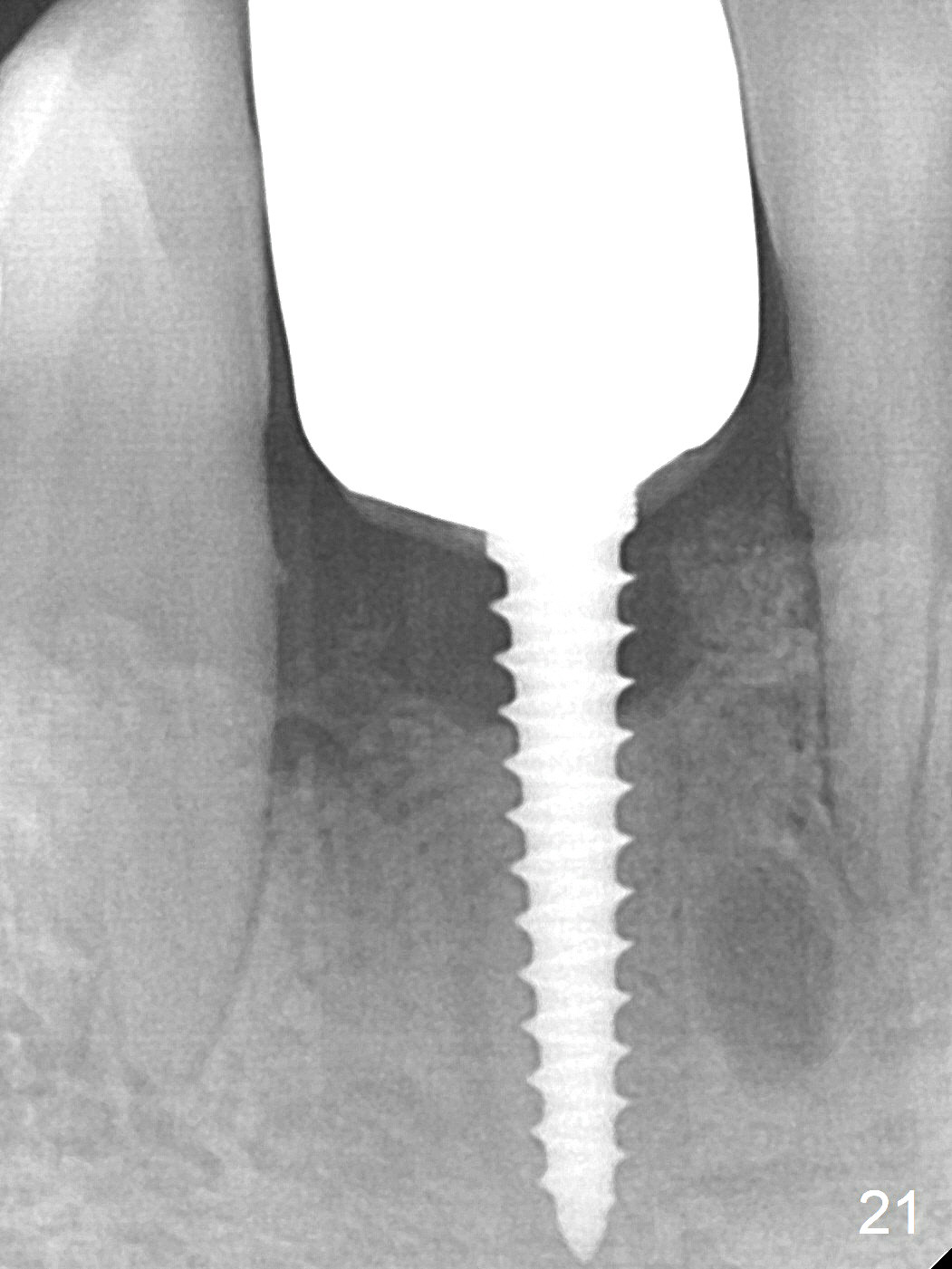
The gingival infection does resolve to certain degree in 2 weeks (Fig.17, as compared to Fig.13) due to modification of the provisional for self cleansing. The ridge has been atrophic in the last 7.5 months (since extraction); it is wide enough to hold the implant (Fig.18,19, compare to Fig.1,2). Fig.20 shows the final crowns at cementation. The restoration is fine 9 months post cementation at the time of the last revision. More implant threads are buried in the solid bone 22 months post cementation (Fig.21).
Return to Lower Incisor Immediate Implant,
Technicians, #4,
14,
1-Piece
Xin Wei, DDS, PhD, MS 1st edition 03/01/2015, last revision 01/19/2018