.jpg)



%20reprep%2023,27.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
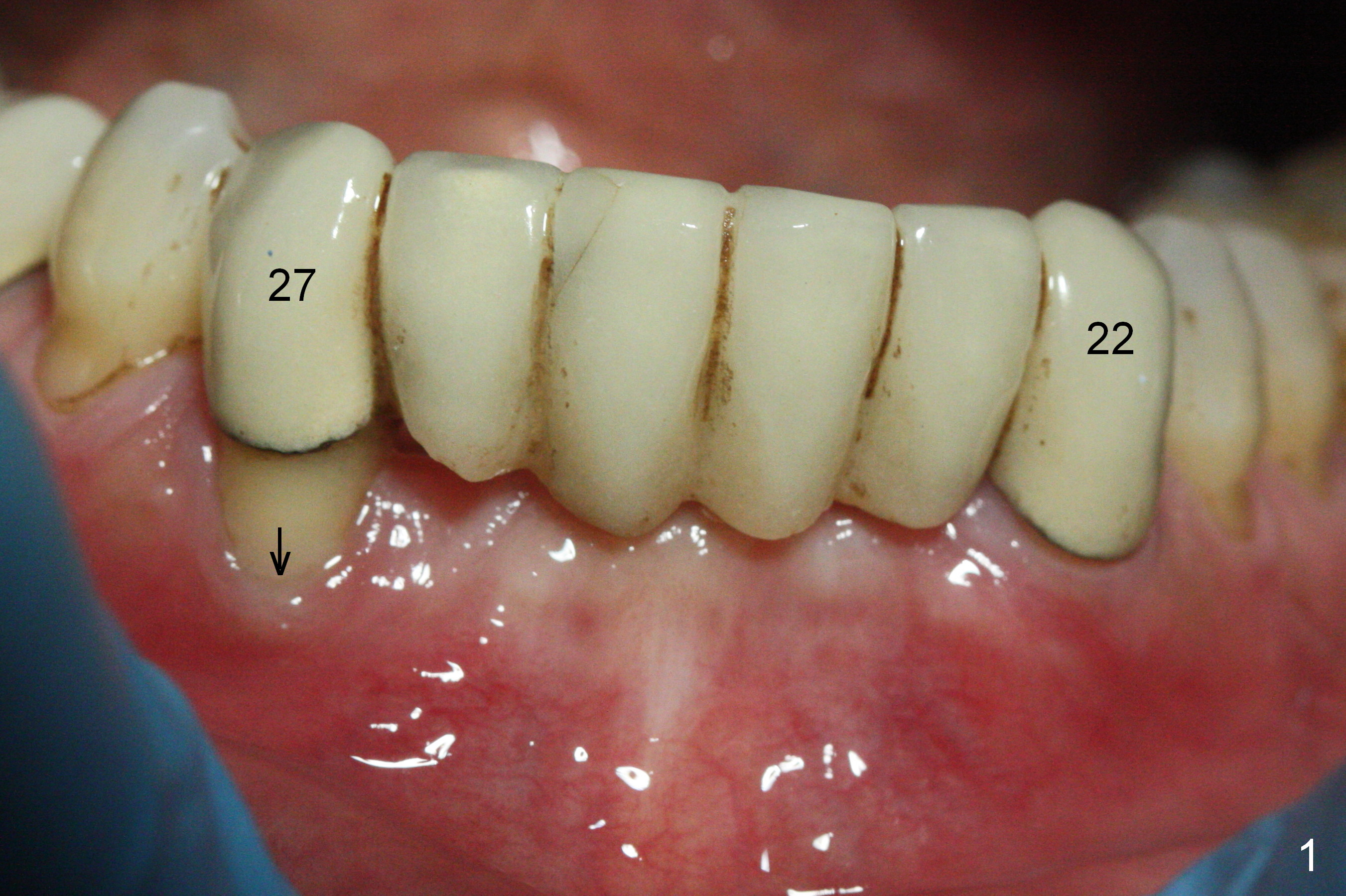
Narrow Implant for Severe Buccal Plate Defect
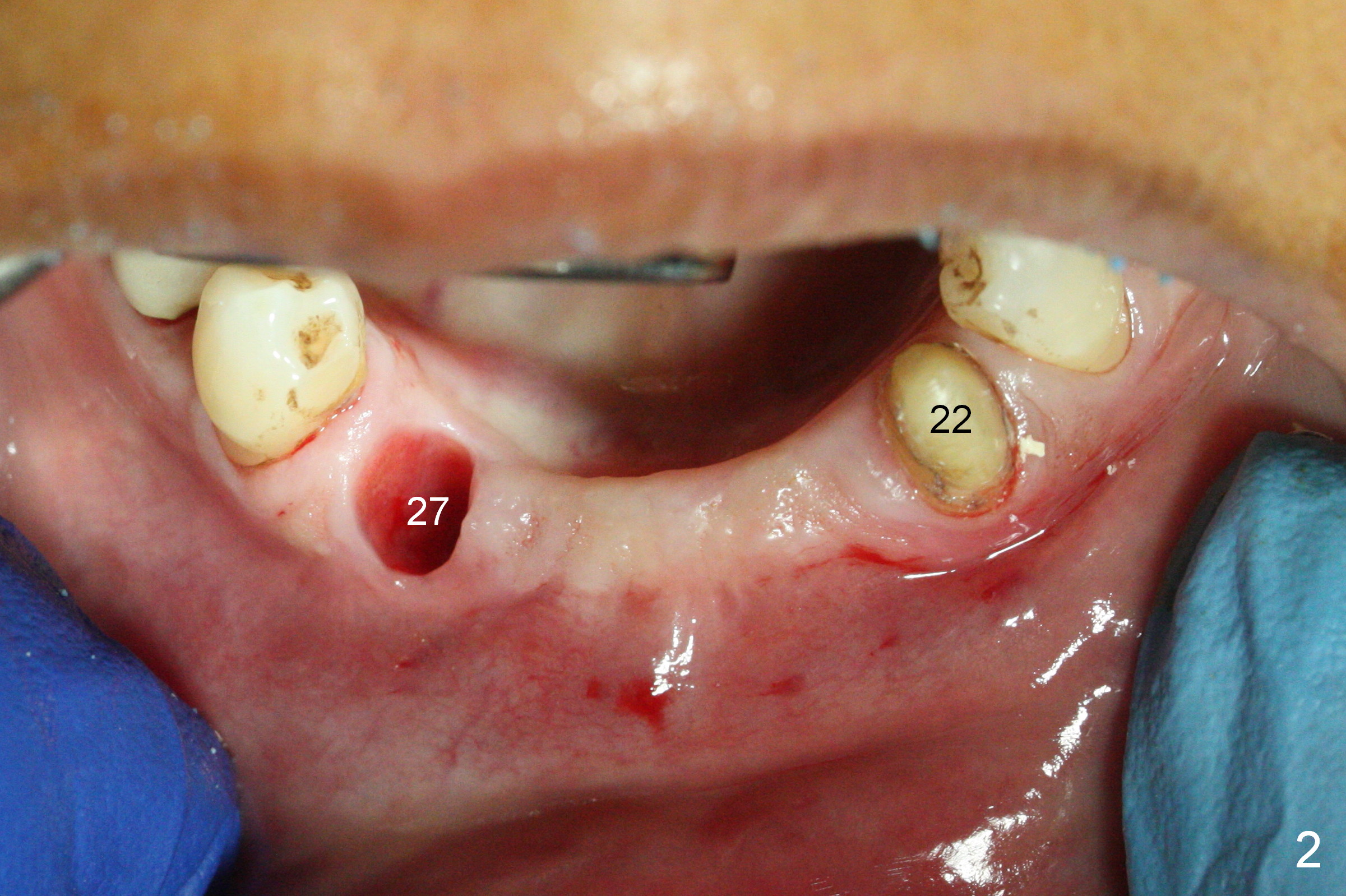
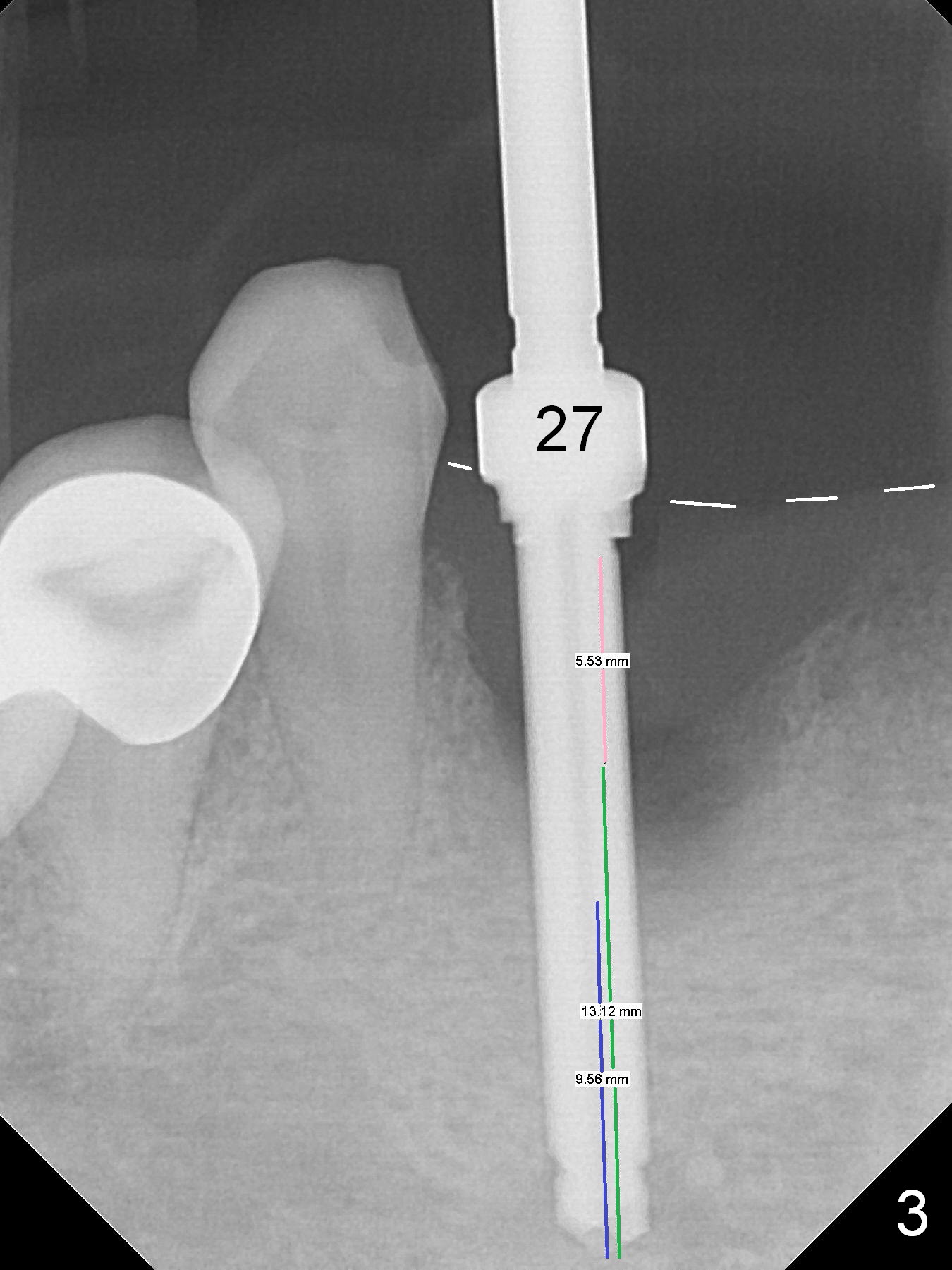
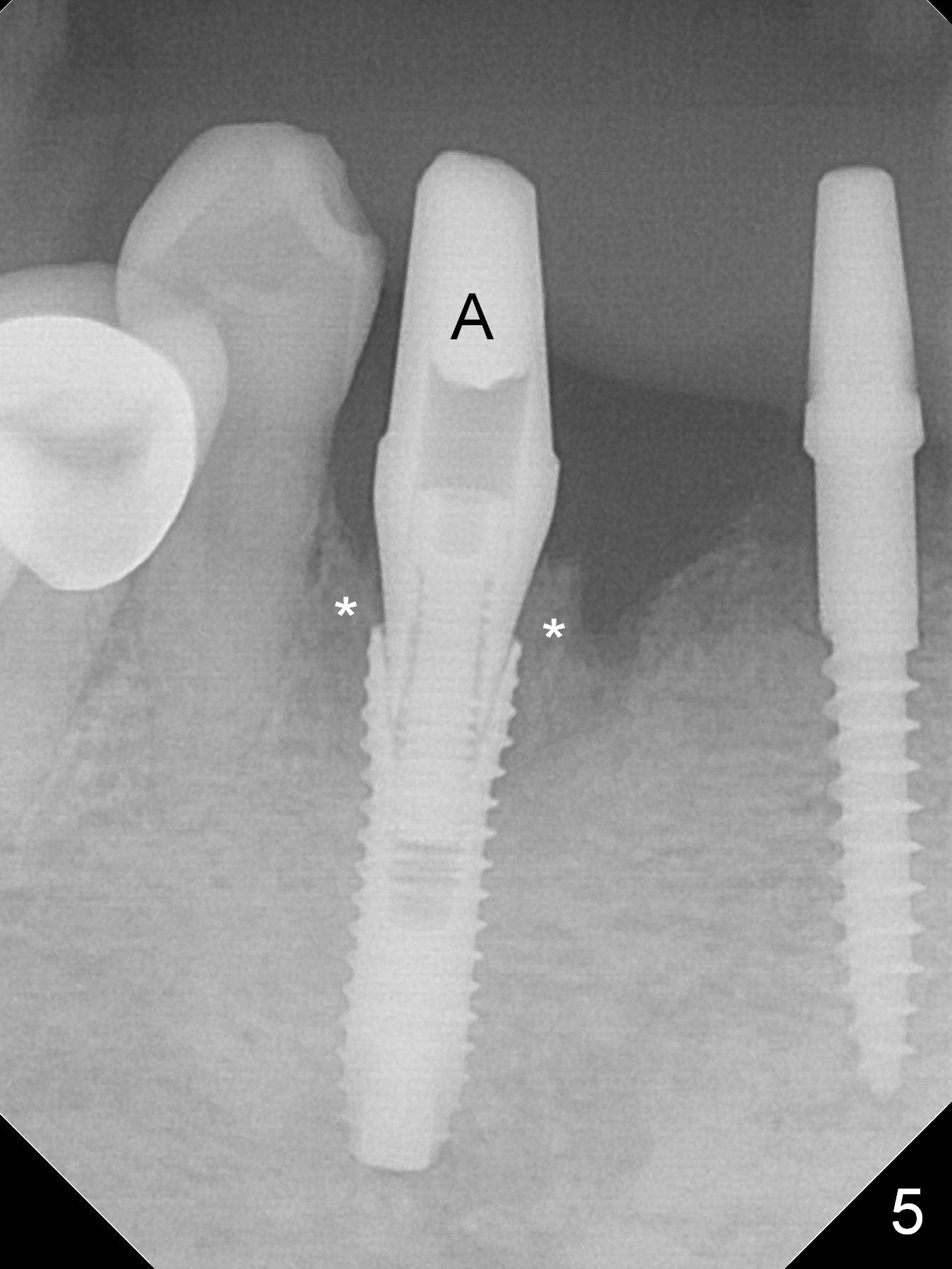
There is severe buccal gingival recession at #27 (Fig.1 arrow), as compared to that at #22. After removing the bridge and extraction of #27 (Fig.2 with severe loss of the buccal plate), a 3x18 mm drill is used to finish osteotomy (Fig.3). A 3.8x13 mm UF implant (Fig.3 green line) will be placed with 9 mm in the apparently solid, native (new) bone (blue line), while the coronal 5 mm will be occupied by the 5 mm cuff of a cemented abutment (pink line). The white dashed line is the gingival margin. The osteotomy is initiated as lingual as possible so that there will be at least 2 mm buccal gap when the narrow implant is placed. In spite of effort and precaution (guided surgery could control the trajetory), the coronal end of the implant tilts buccally so that a 4.5 mm 15 ° A 4 mm angled abutment is placed slightly subgingival (except buccal; Fig.5 A).
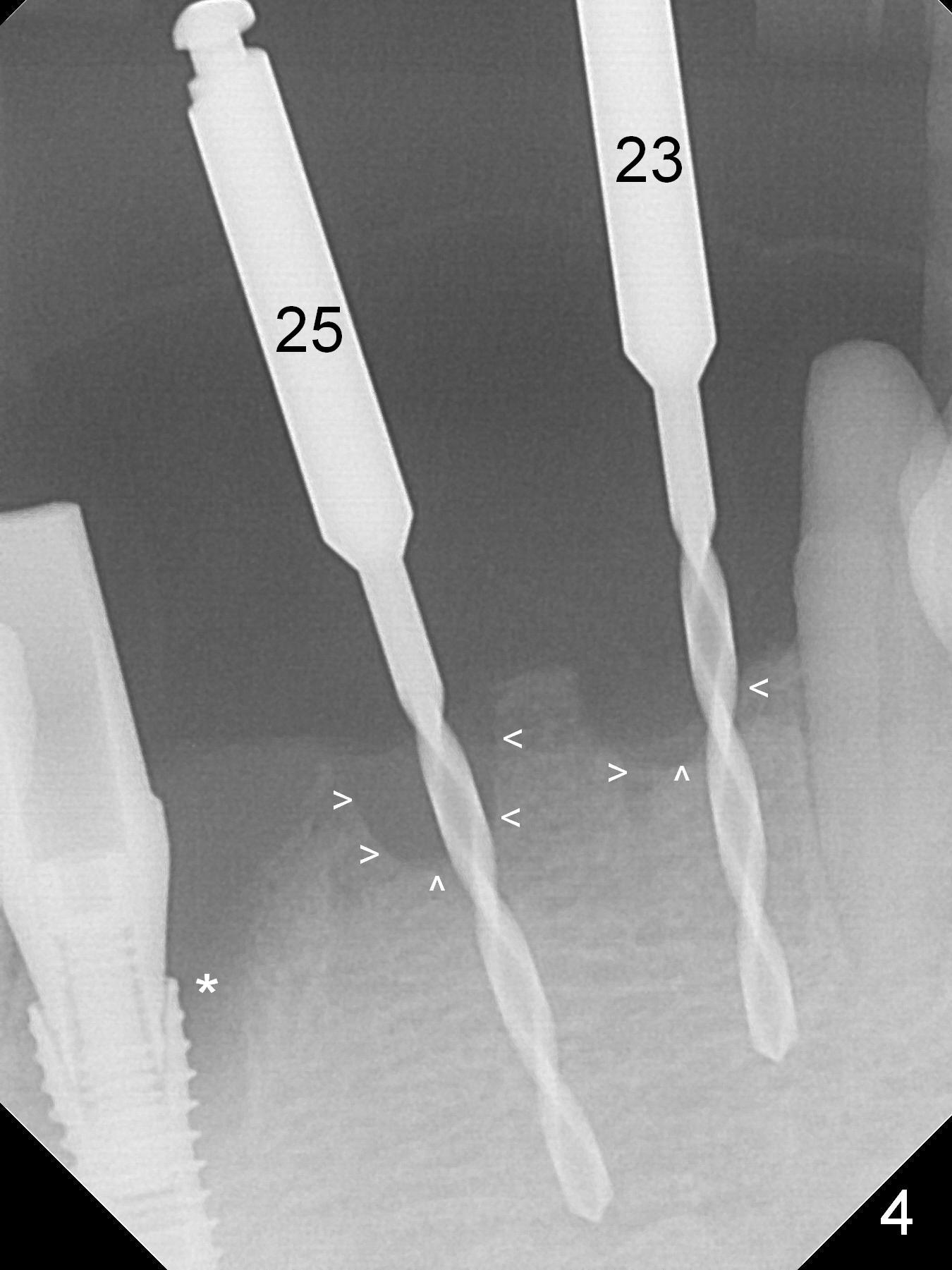
Since the ridge between the lower canines is atrophic (Fig.2), osteotomy starts at #23 and 25 after crestal reduction (Fig.4 arrowheads), Two of 2.5x12(4) mm 1-piece implants are placed (Fig.6). The implants at #23, 25 and 27 and the tooth #22 support an immediate provisional bridge (Fig.7).
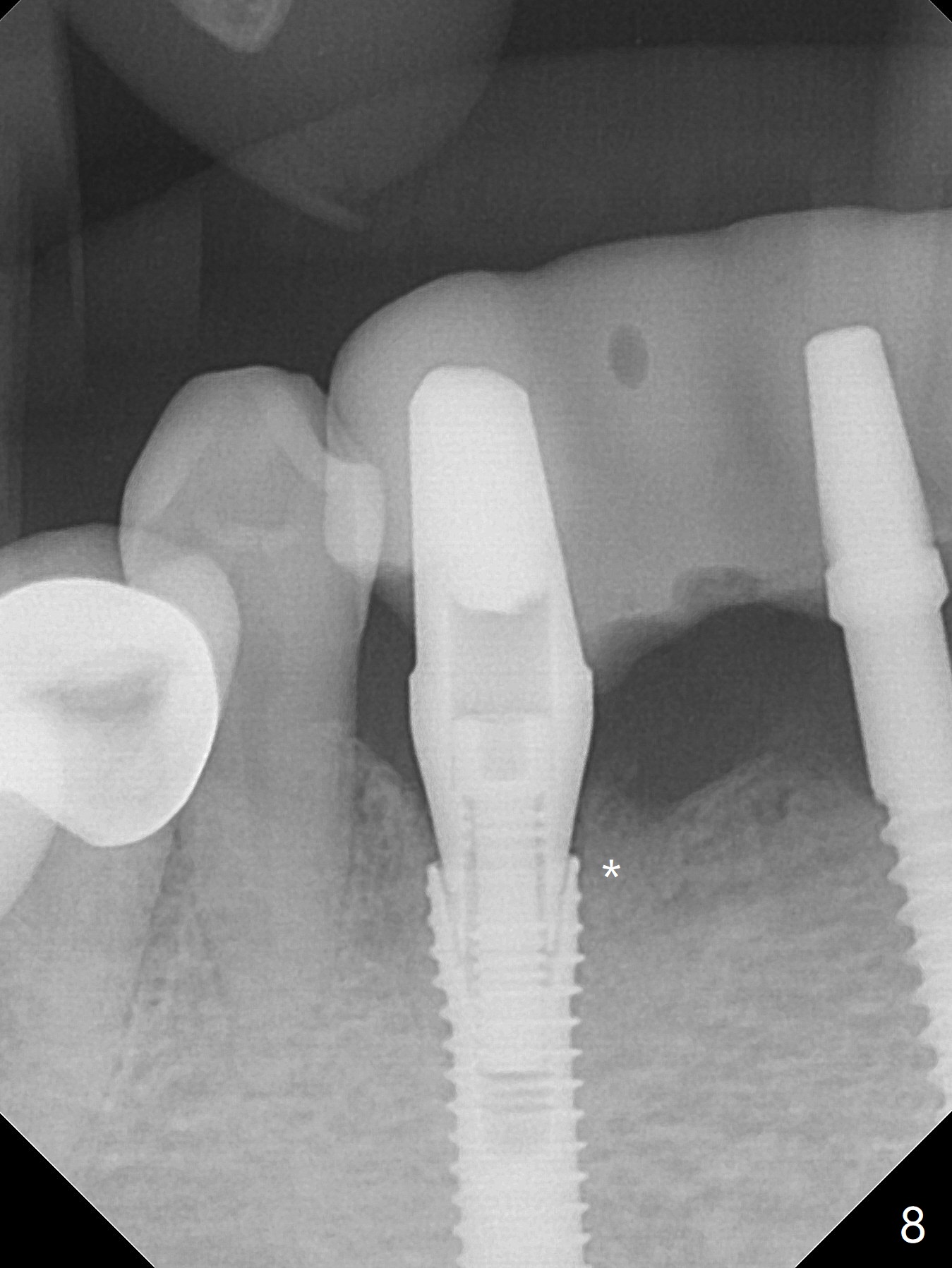
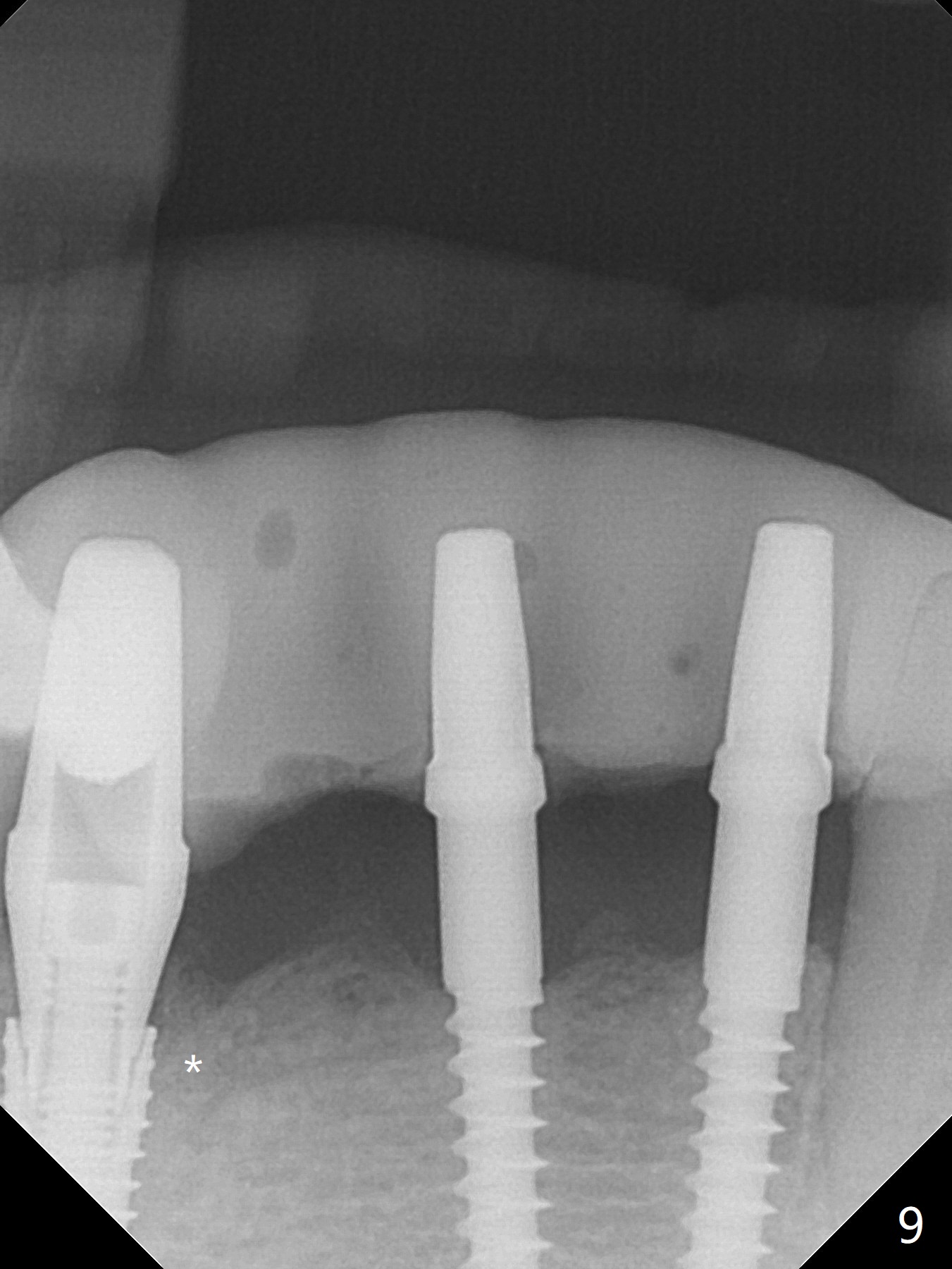
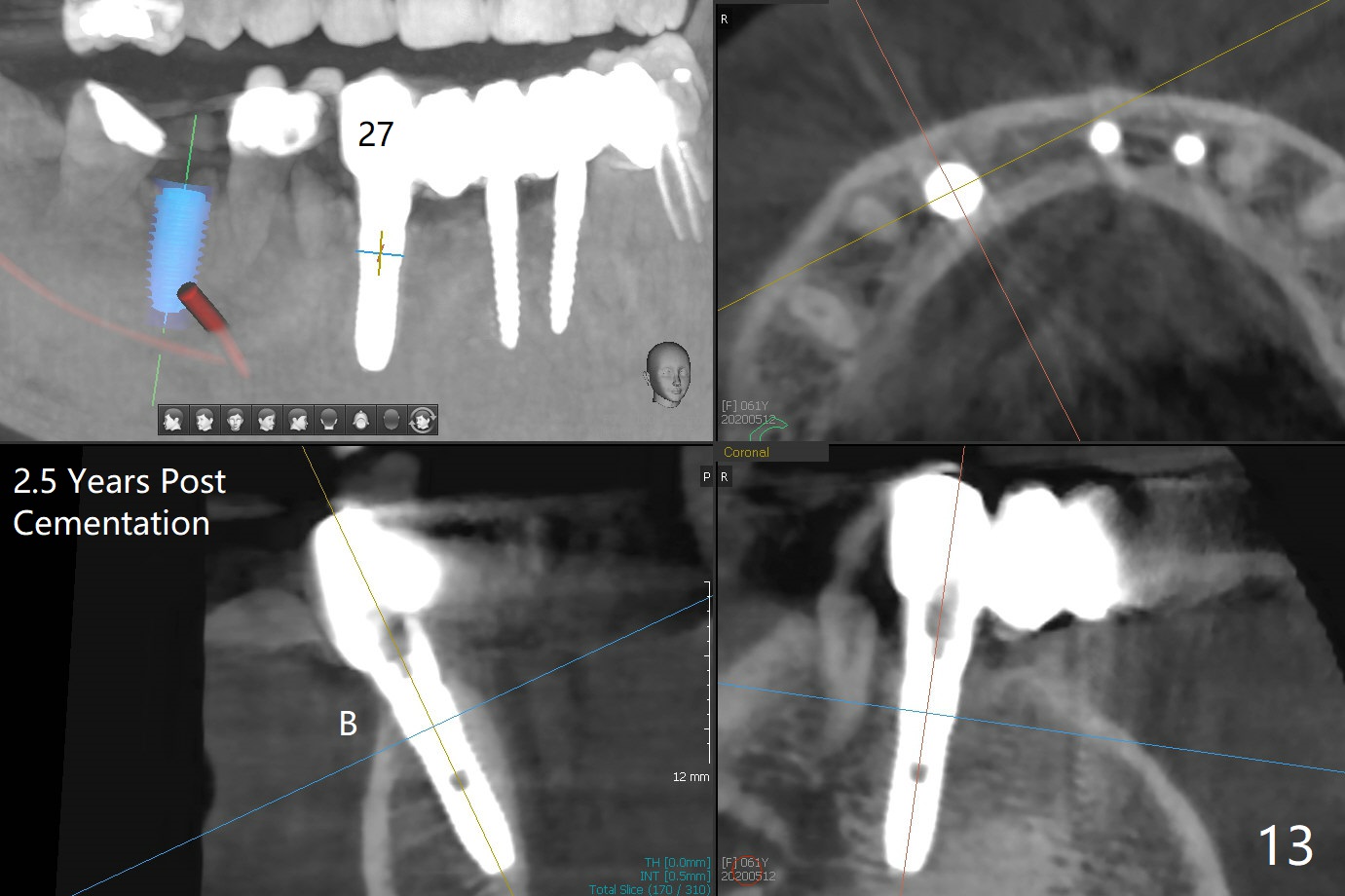
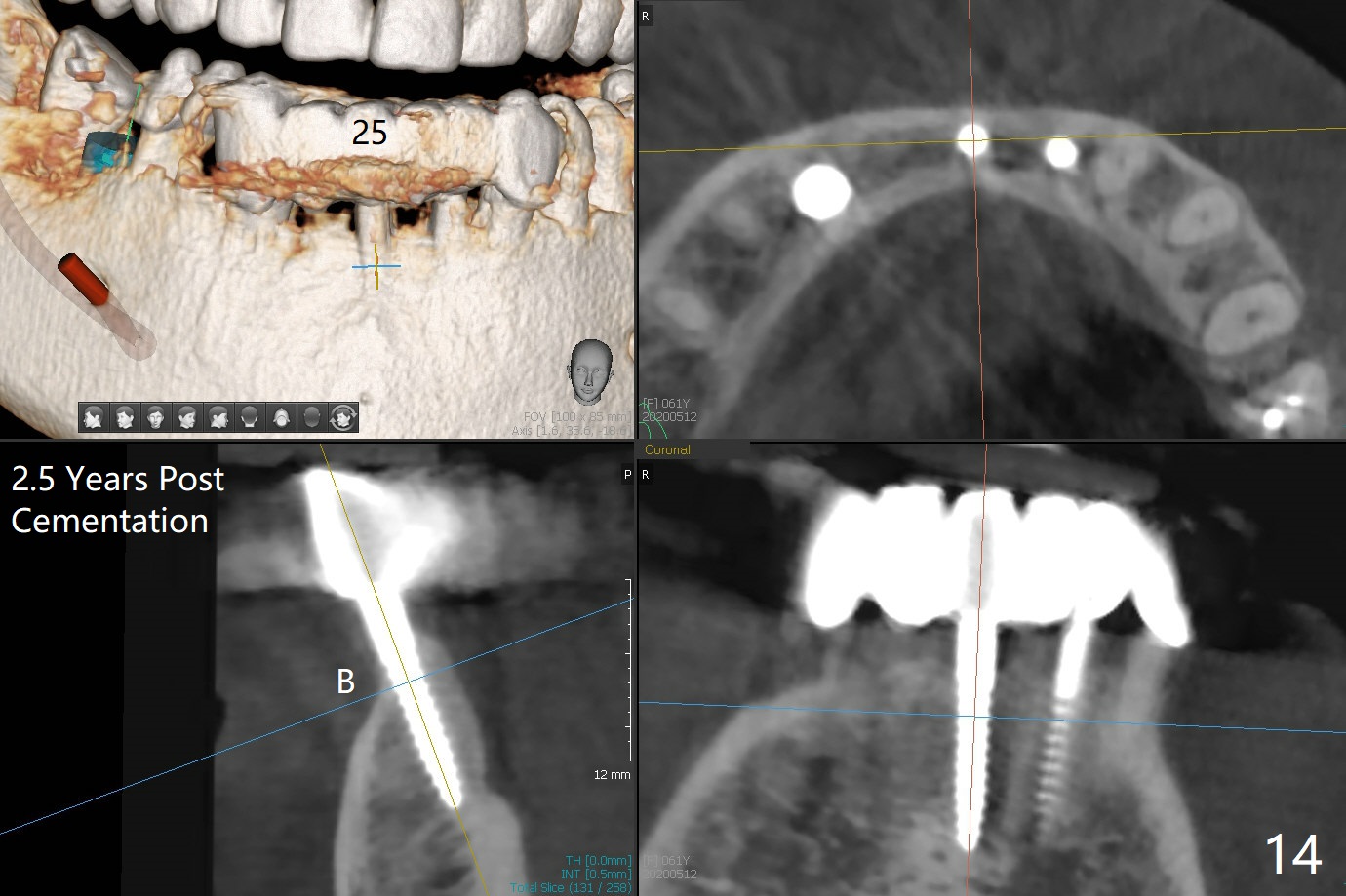
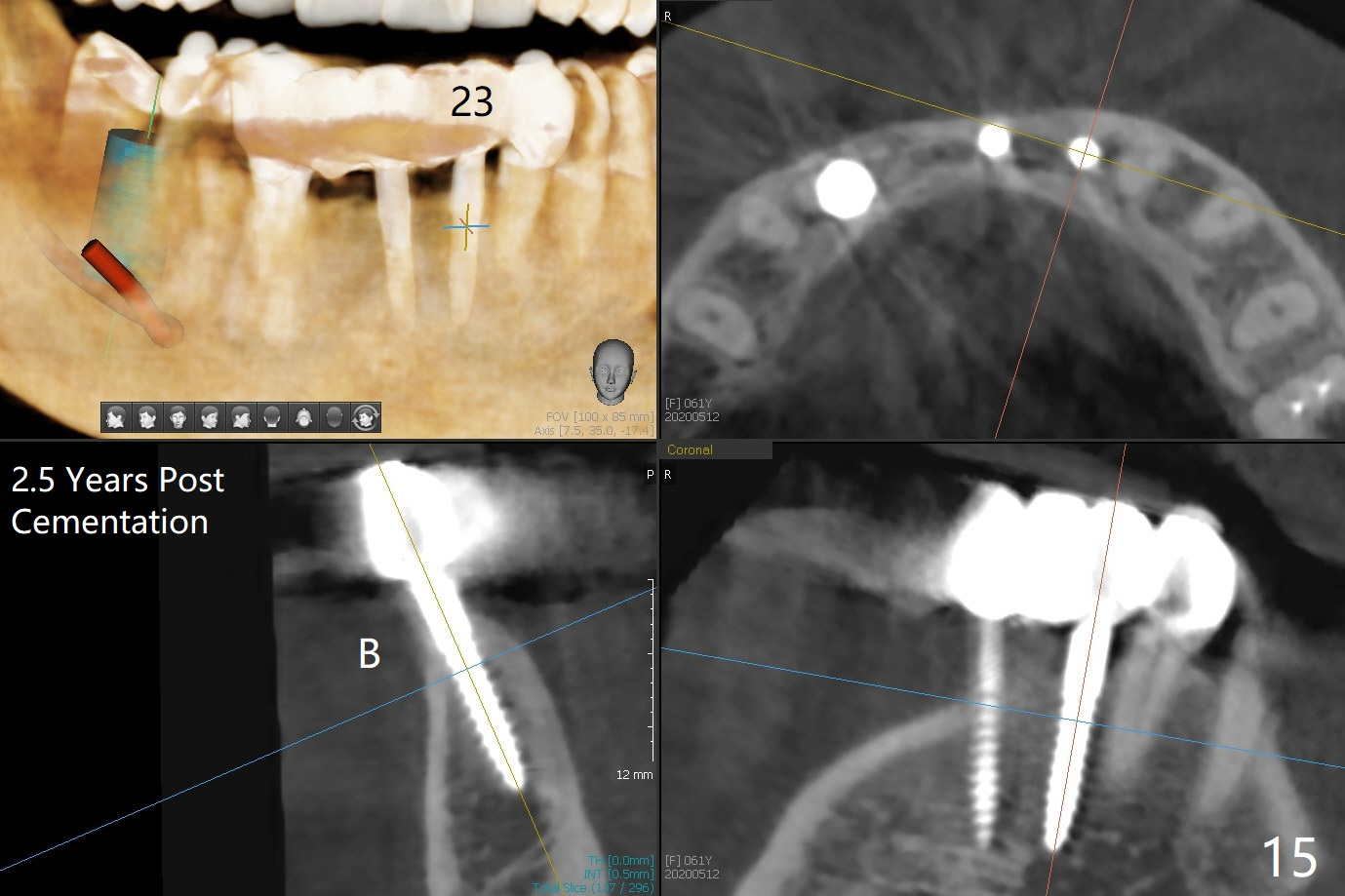
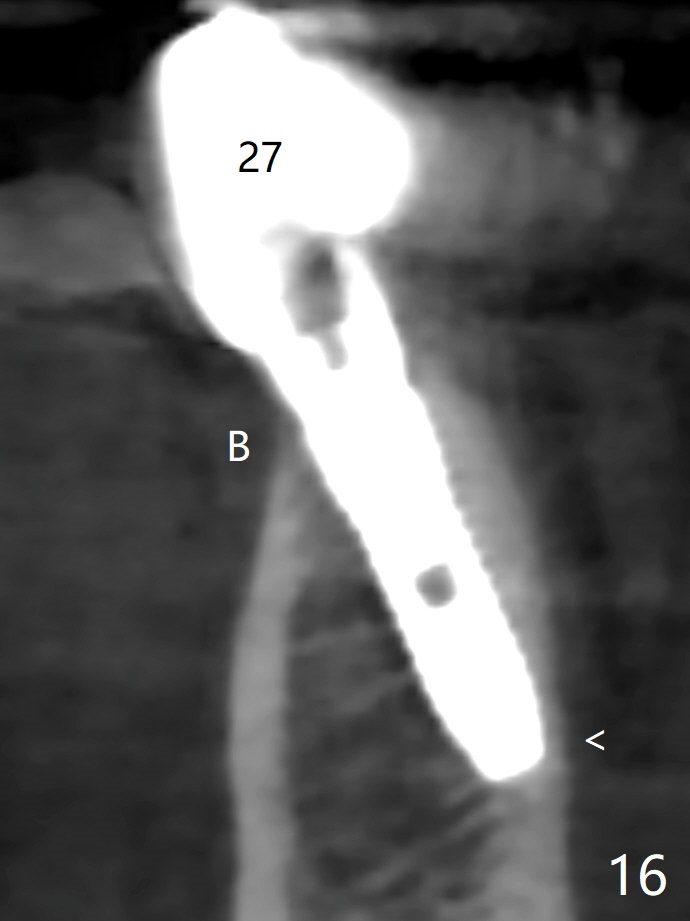
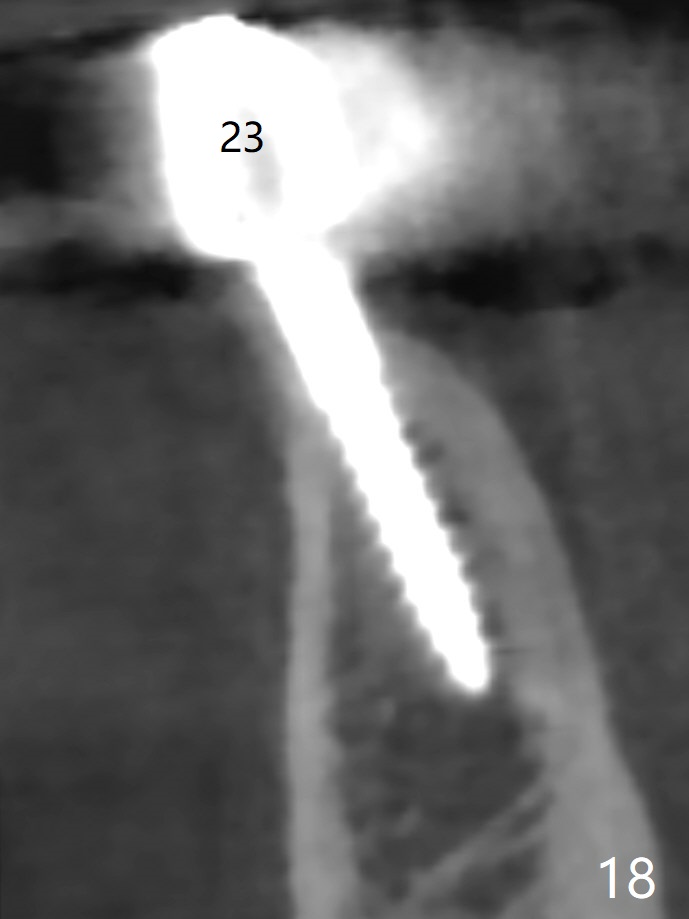
The mesial defect at #27 appears to have been repaired 8 months postop (Fig.8,9 *); there is no bone loss at 1-piece implant sites. The gingival recession seems to remain the same before and after removal of the provisional FPD (Fig.10,11). The bulging abutment at the cervix is less prominent when a straight abutment is used and prepared (Fig.12, 4.5x5.5(5) mm). There is no bone loss at #23, 25 and 27 sites 2.5 years post cementation (Fig.12-15), although the trajectory of the implants could be improved by using surgical guide (Fig.16-18).
Return to
Lower
Canine Immediate Implant,
IBS #30
Xin Wei, DDS, PhD, MS 1st edition 02/02/2017, last revision 05/12/2020