
.jpg)
%204y4m%20post%20cem.jpg)
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
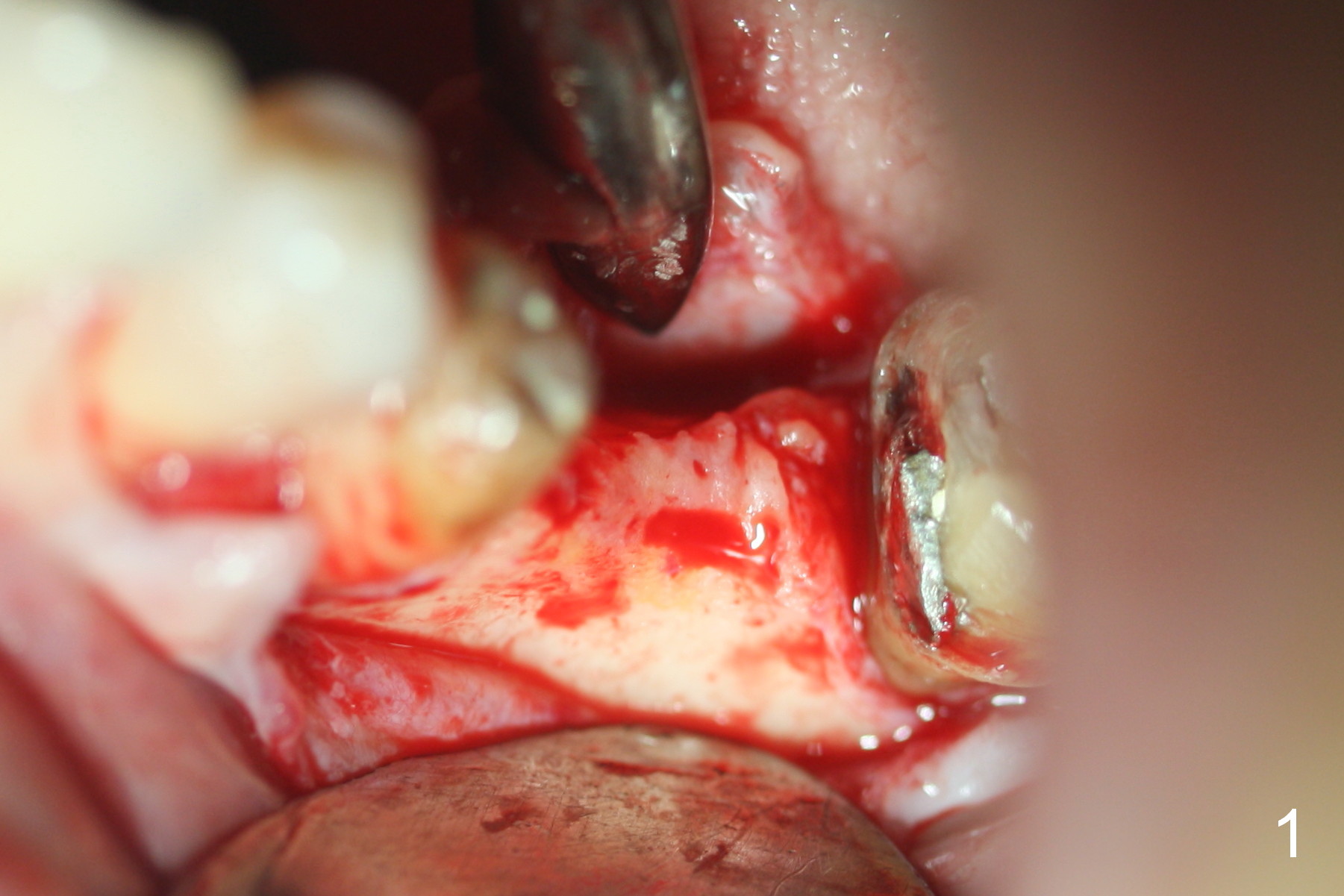
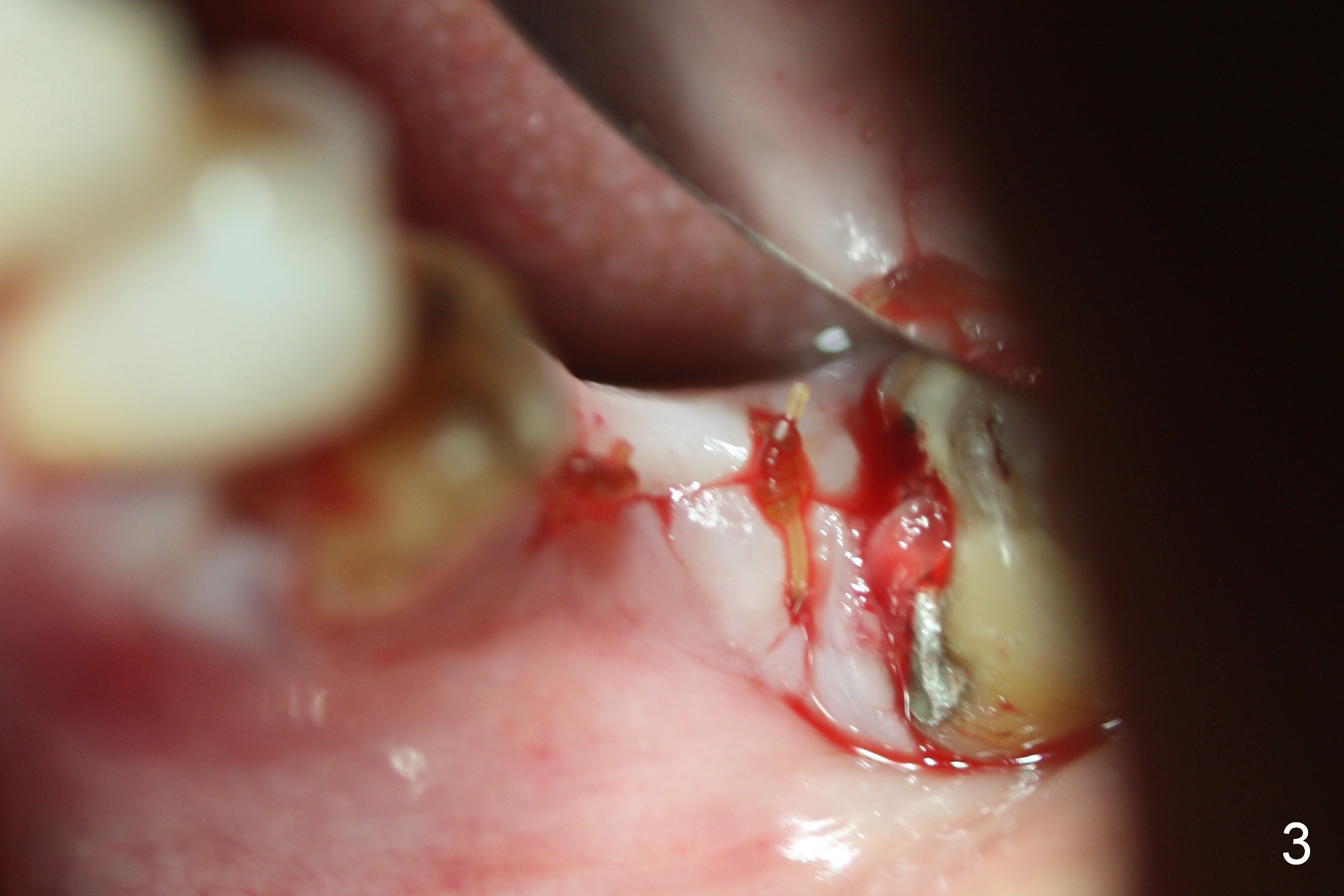
Preop palpation shows that the ridge is moderately atrophic. When flaps are raised, the crest is quite narrow (Fig.1). The limited access is not favorable for bone graft (primary closure). A surgical bur is used to make bone cut as shown in Fig.2. The incision is closed with 4-0 Chromic gut suture (Fig.3).
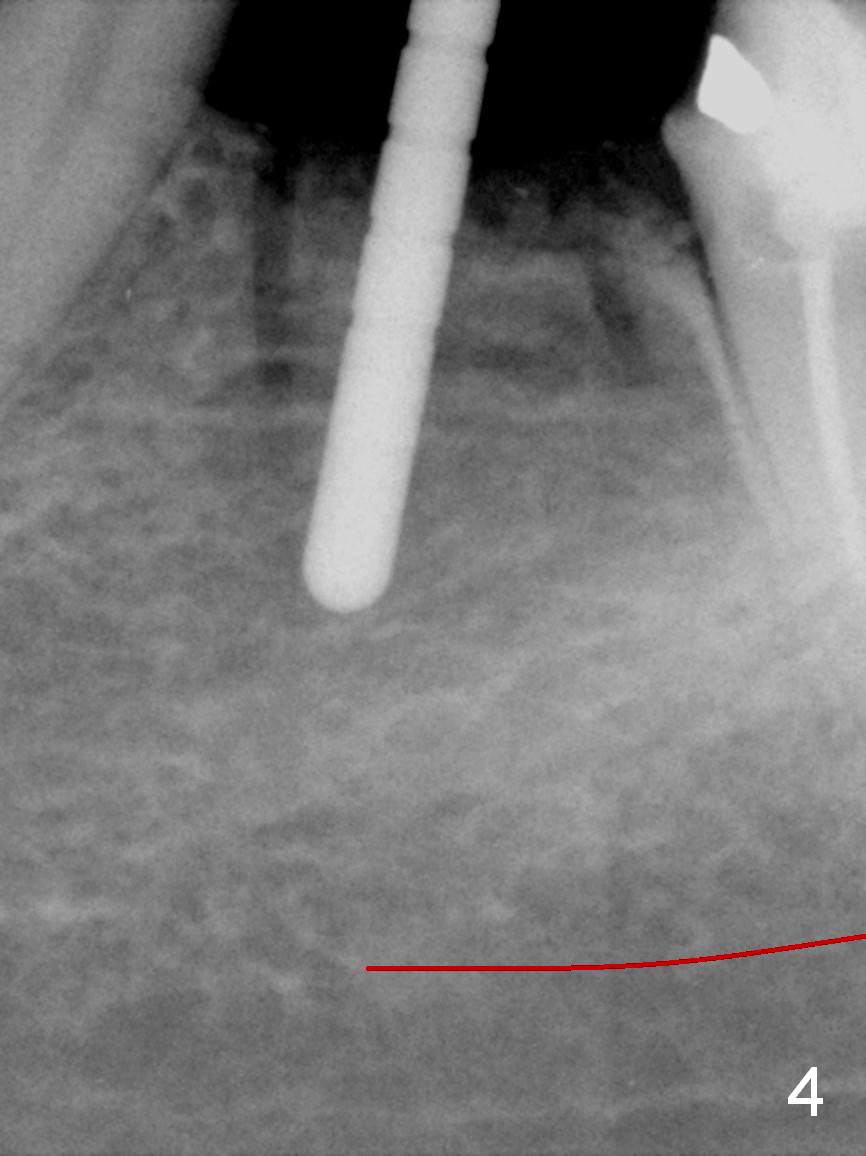
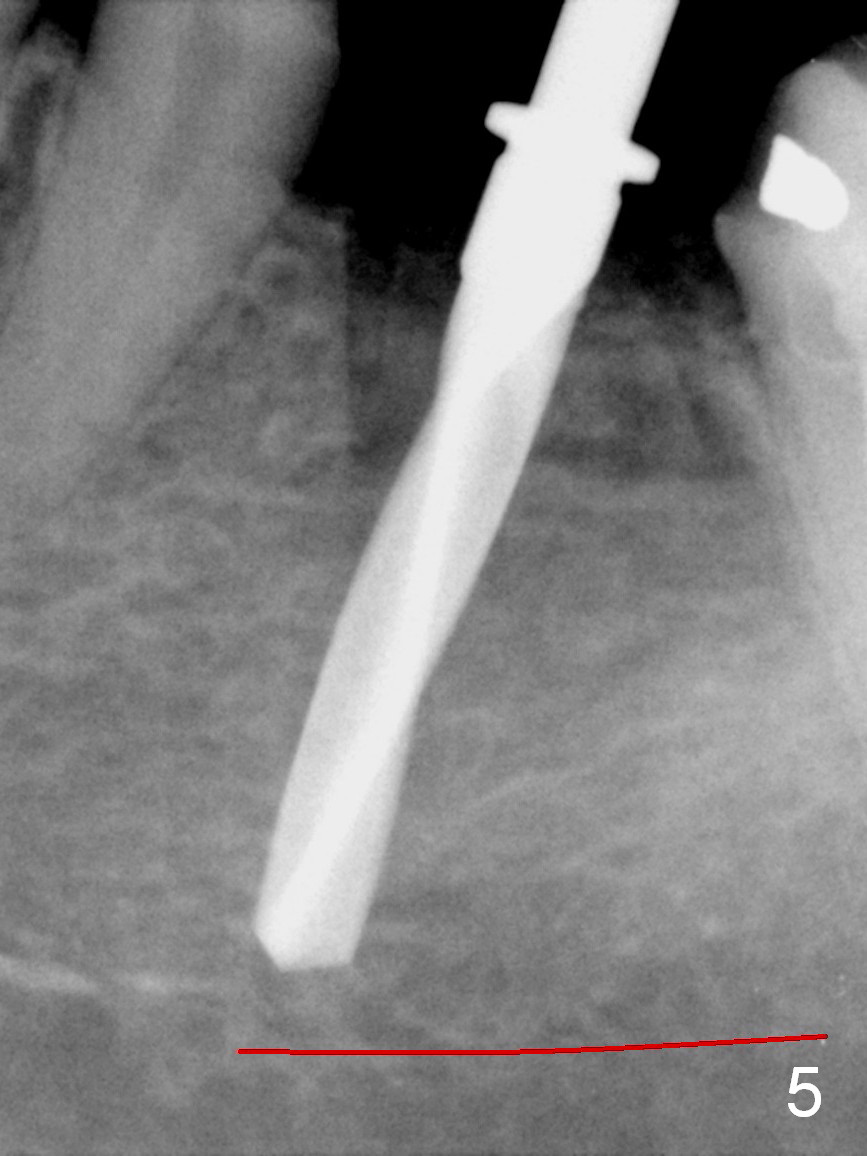
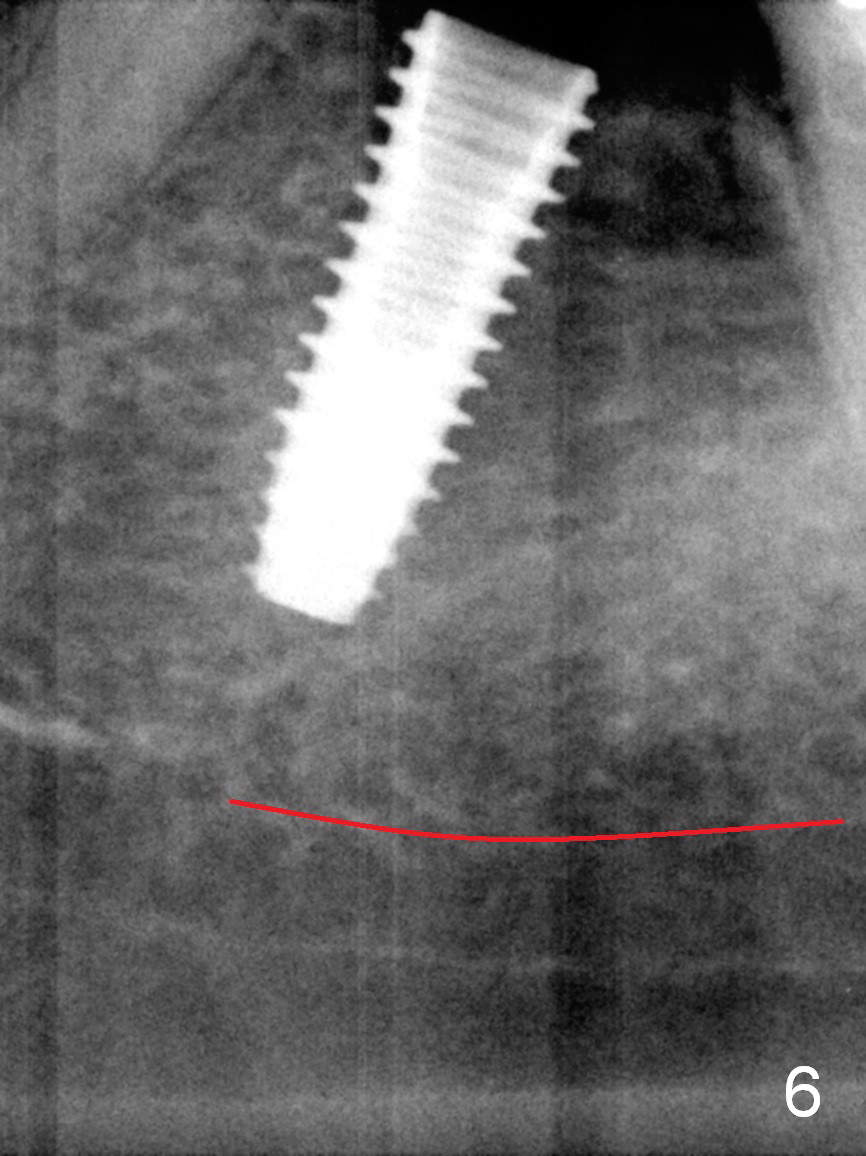
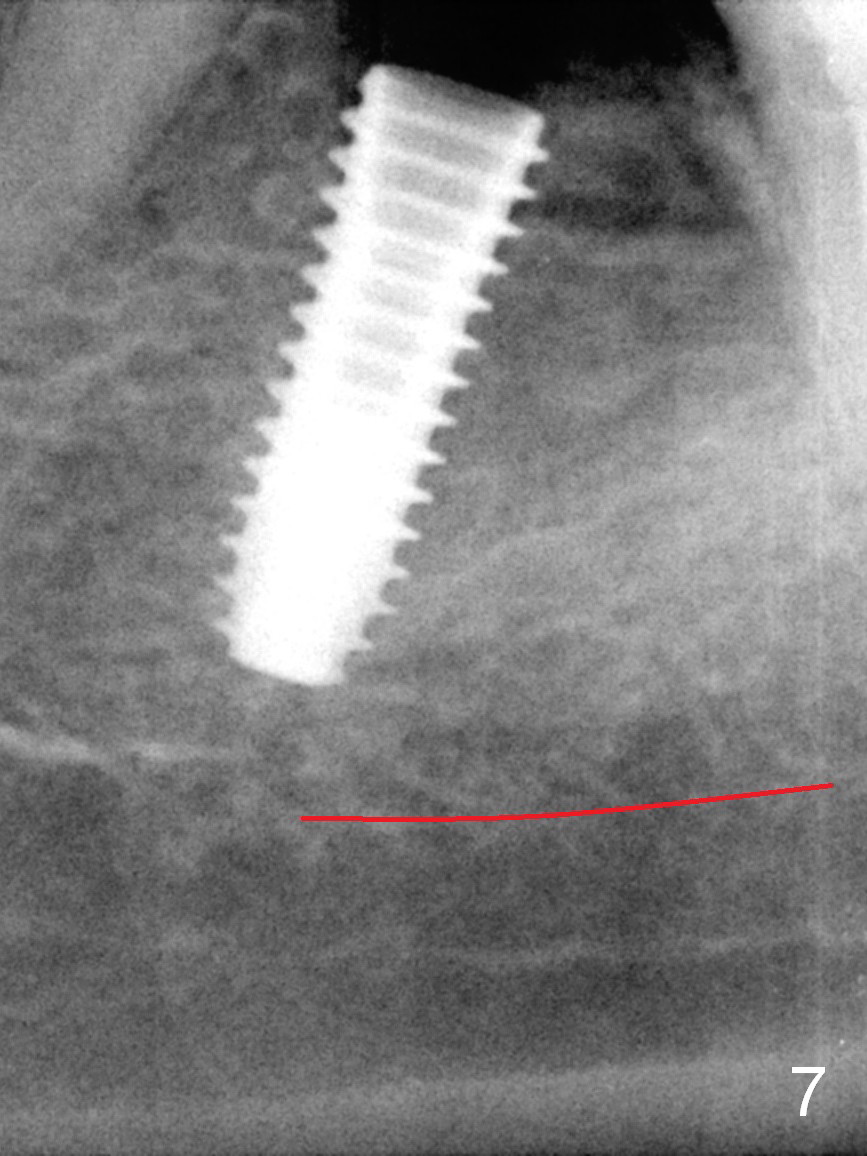
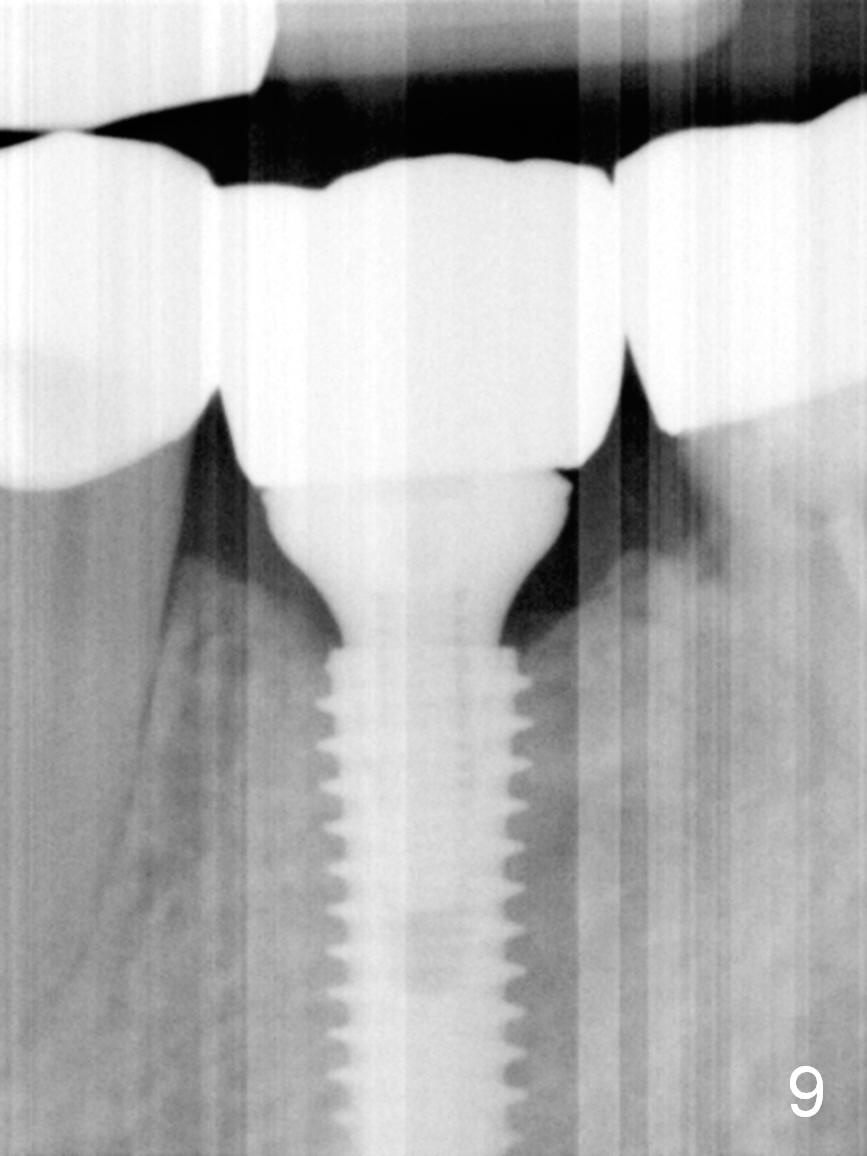
Two weeks later, small incision is made on the crest. Limited exposure to the crestal bony cut is provided. A curved chisel is used to try to split the crest. It feels more likely that the lingual plate is fractured. A starter drill and 2 mm initial drill are used for osteotomy 12 mm deep from gingival margin (Fig.4 (red line: the superior border of the Inferior Alveolar Canal)). The 2 smallest bone drills from Esset Kit (Hiossen) are used with purpose to push the buccal plate buccally. Sequential osteotomy is finished until 4x13 mm drill with stopper. With soft tissue interference, the depth is assumed not enough. A 2.7 mm drill is re-used with intention to go down for 16 mm. Because of soft bone, the drill dropped deeper than expected (Fig.5). When a 4.5x13 mm implant is being placed, it is deviated buccally. With the implant being removed, the osteotomy is moved lingually with Lindamann bur and 4 and 4.5x13 mm drills. When the implant is placed for the second time, the buccolingual position is acceptable; the depth is a little shallow (Fig.6). Further adjustment of the depth appears to be acceptable (Fig.7). After placing an abutment, an immediate splint provisional is fabricated between #18-20. Three months postop, the split ridge appears to have healed with formation of apparent lamina dura distally (Fig.8 arrowheads). Clinically the margin of the abutment (A) is supragingival. A shorter cuff abutment should be used prior to impression. There is no bone loss 5 months post cementation (Fig.9). The 2-staged ridge split seems to be safer in term of bone resorption than the 1-staged one (2,3).
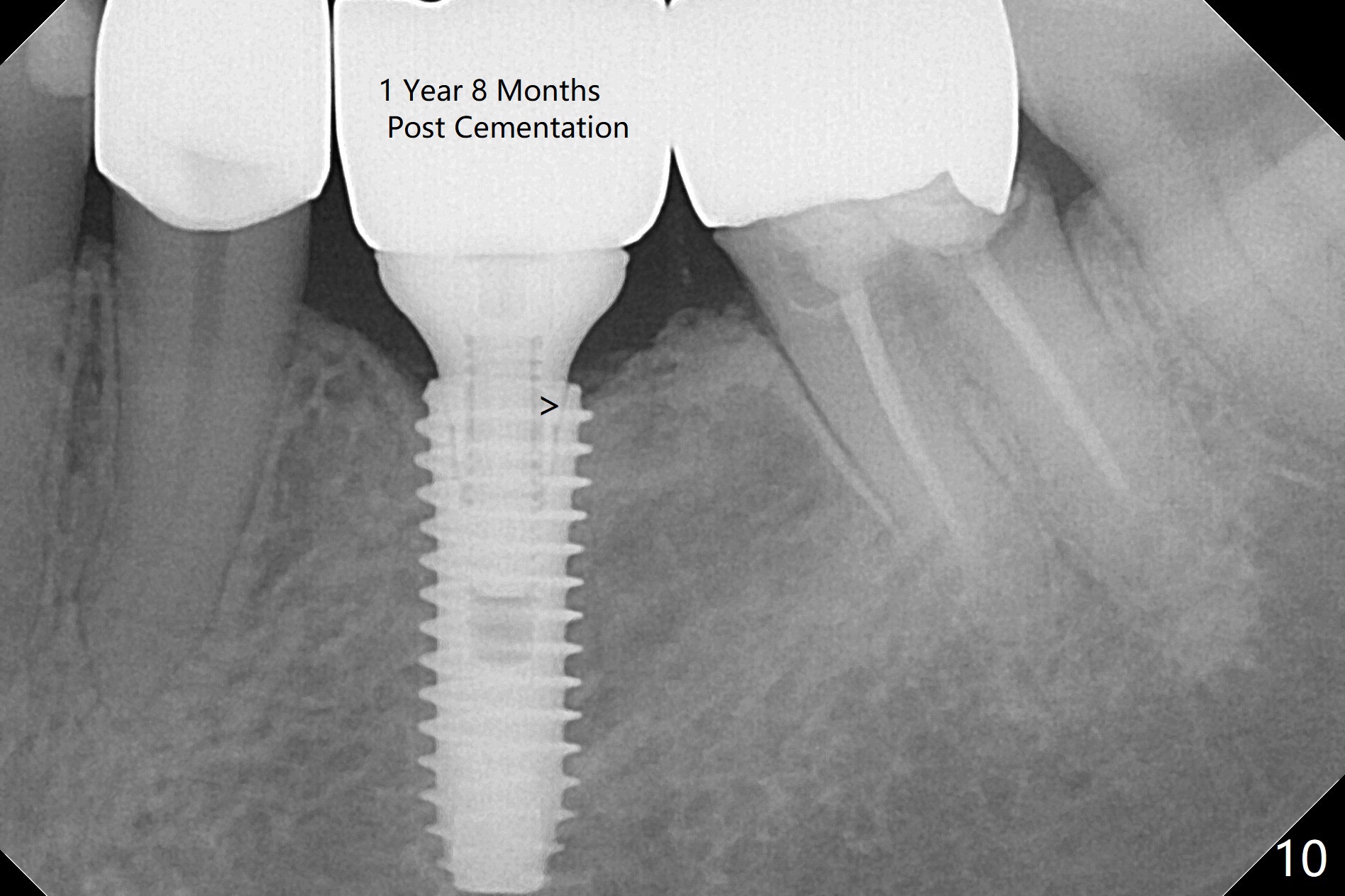
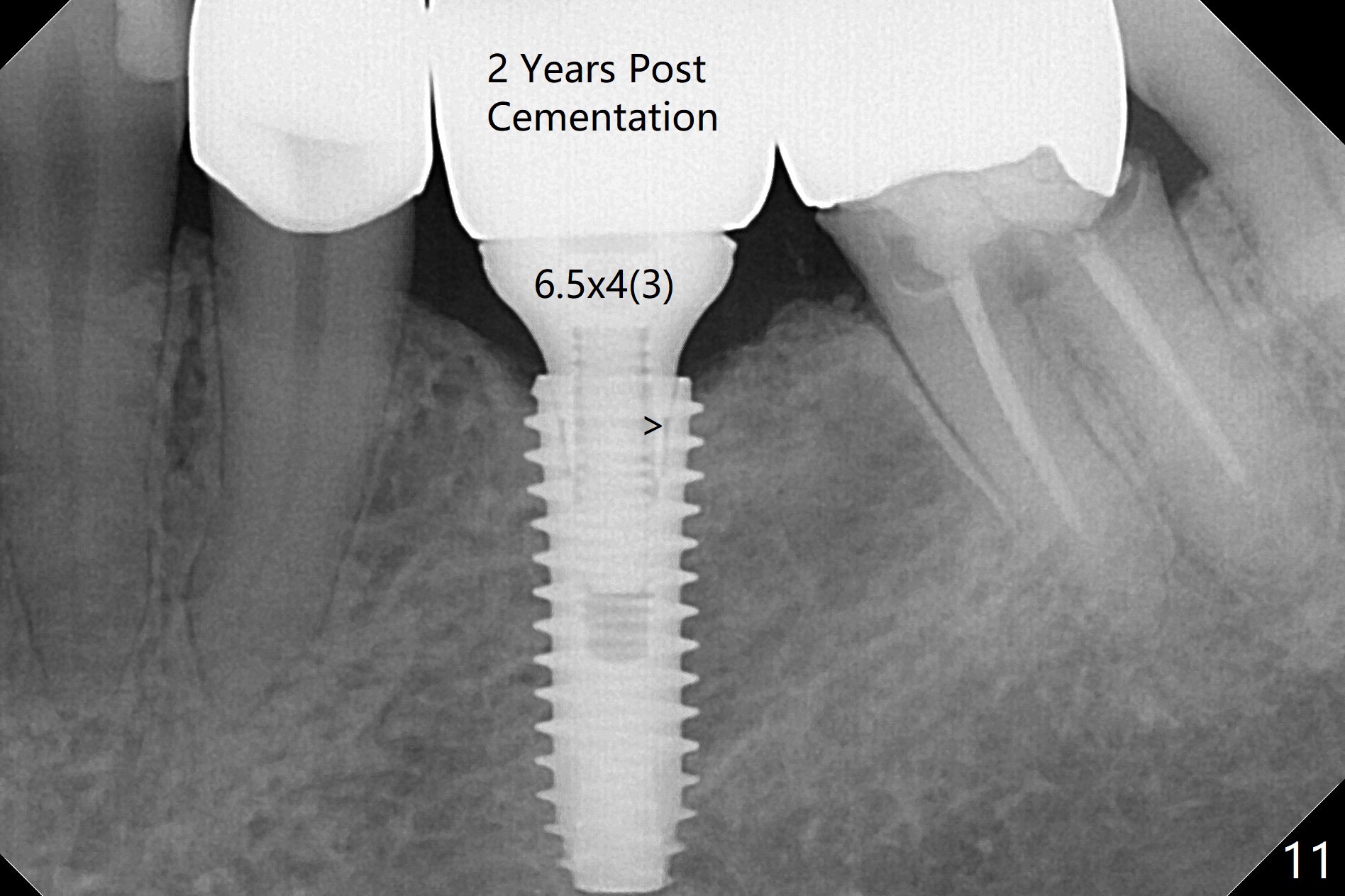
Since the tooth #15 is missing, the abutment screw at #19 was loose 5 months post cementation. Less than 10 days later, the upper right bridge dislodges. In fact the abutment screw loosening is due to incomplete seating of the abutment (Fig.10,11 >), which is neglected until the screw becomes loose again (nearly 4 years later). Using a smaller abutment, the seating is apparently complete (Fig.12).
Return to
Lower Molar Immediate Implant
劈开术
Xin Wei, DDS, PhD, MS 1st edition 12/01/2015, last revision 04/10/2021