



|
|
|
|
|
|
|
|
|
Depth Control for Implant at Healed Site
The edentulous ridge at #19 is moderately wide at the base, but pointed at the crest (Fig.1). After raising flaps, it appears that the ridge can hold a 5 mm implant using an implant positioner. The initial osteotomy is 12 mm deep and about 4 mm from the Inferior Alveolar Canal (Fig.2 yellow dashed line). Sequential osteotomy is carried out until 5x12 mm. Because of the pointed crest, 4.5 drill is used to extend the osteotomy at ~ 13 mm so that 12 mm implant can be placed a little deeper to reduce the amount of thread exposure. A 5.3x12 mm implant cannot be seated as deep as expected. A 5.3x10 mm drill with stopper is used before placing the same implant as mentioned above at the desirable depth (Fig.3). The insertion torque is > 60 Ncm. An abutment is placed immediately and an immediate provisional is fabricated and seated. Two to 3 microthreads buccally and lingually are covered by autogenous bone graft and collagen membrane. The patient returns for impression 4 months postop. There is bone loss distally (Fig.4 *). His oral hygiene is excellent. It is hoped that the bone loss will not get worse in the next visit.
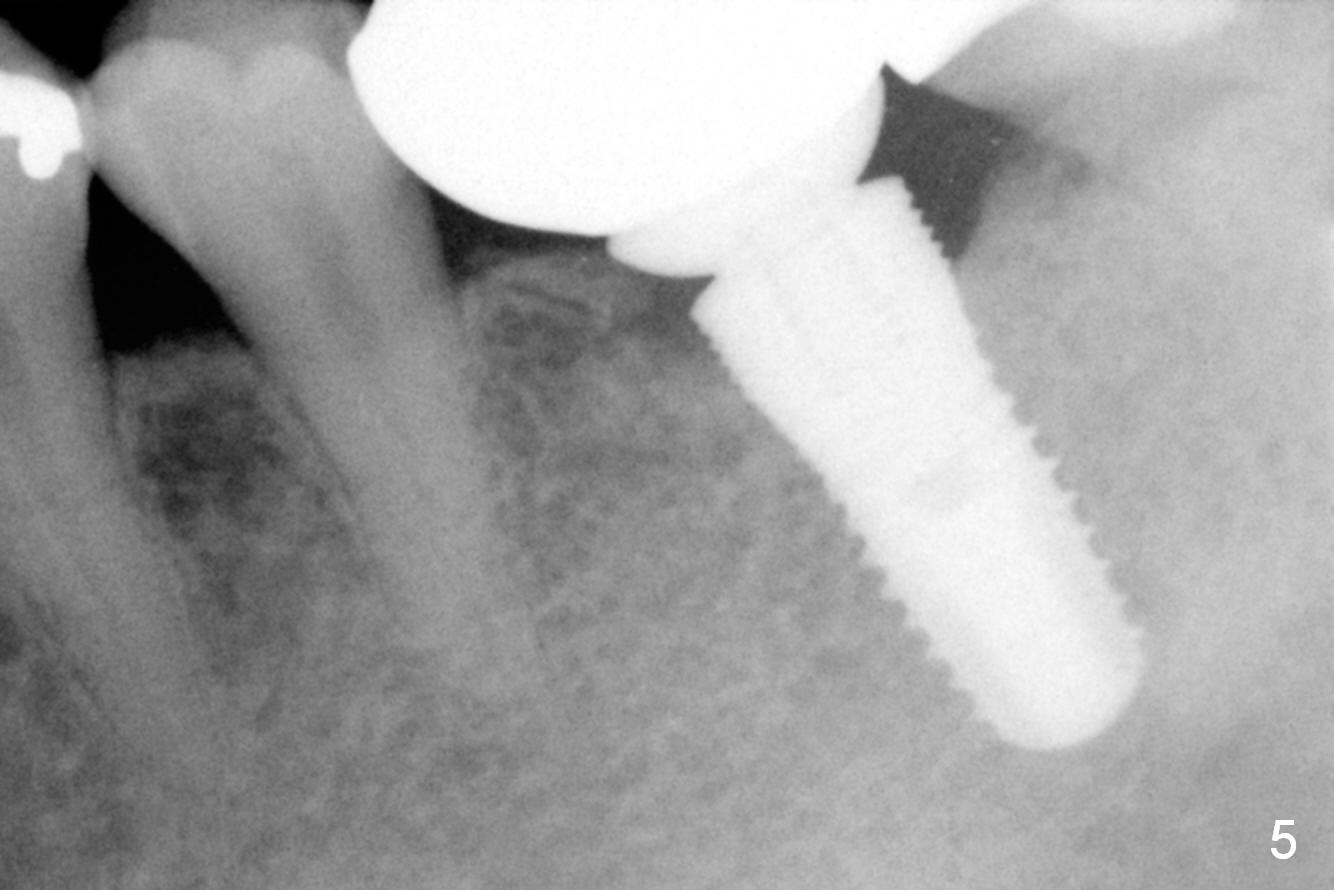
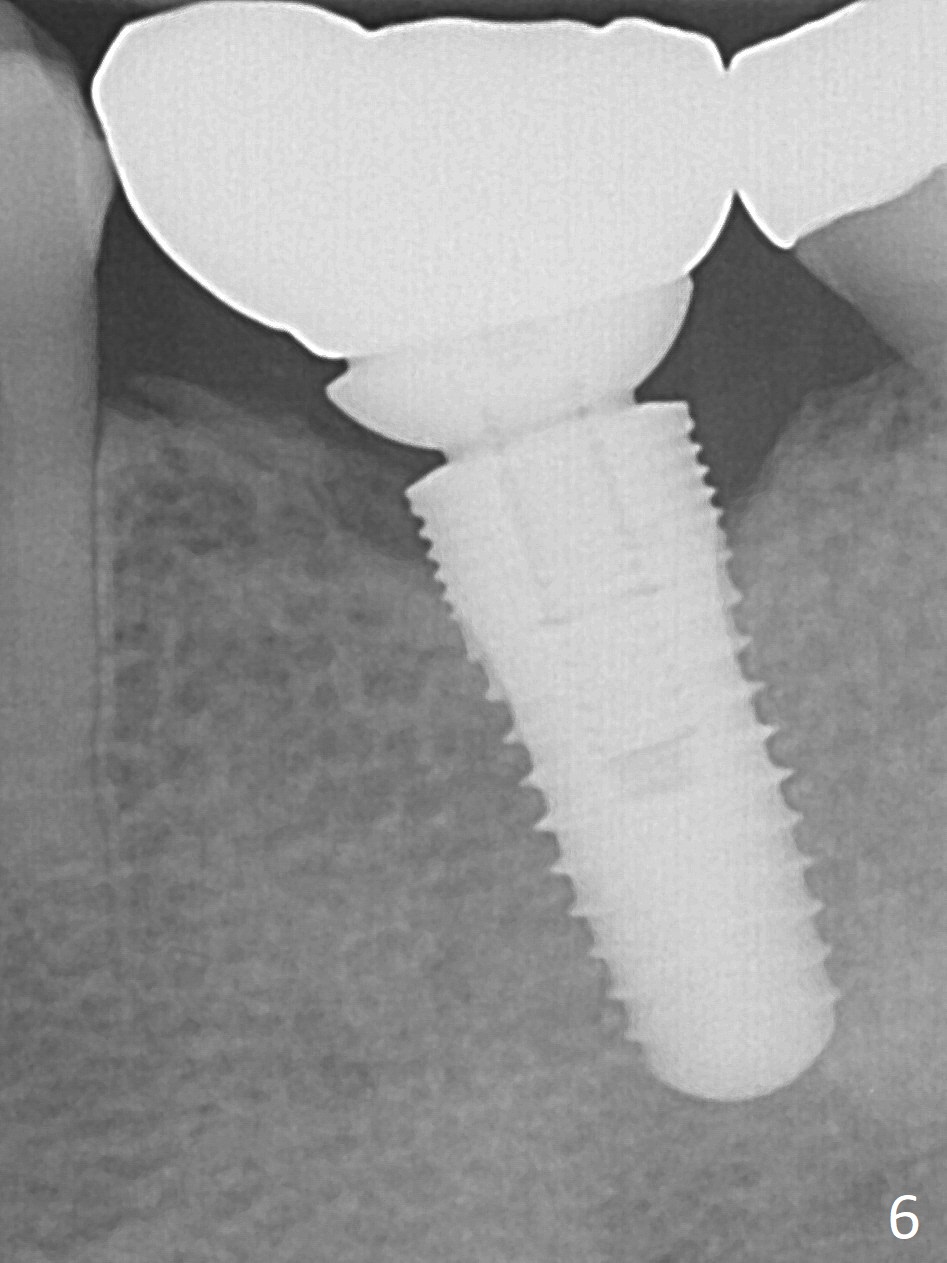
It appears that the diameter of the implant should be also controlled. A smaller implant may not lead to thread exposure and ultimately bone loss. It remains to be true 7 months post cementation (Fig.5). It appears that a 4.5 mm implant is better choice. There is no sign of periimplantitis. Oral hygiene, soft and hard tissues remains basically the same 2 years post cementation (Fig.6). The mesial open margin may be related to failure of impression material to get to the margin in spite of laser gingivectomy.
Return to Lower Molar Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 06/19/2015, last revision 11/24/2017