


.jpg)



.jpg)
%203y10m%20post%20cem.jpg)
%20bw.jpg)
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
||||
Sudden Change from Extraction to Immediate Implant
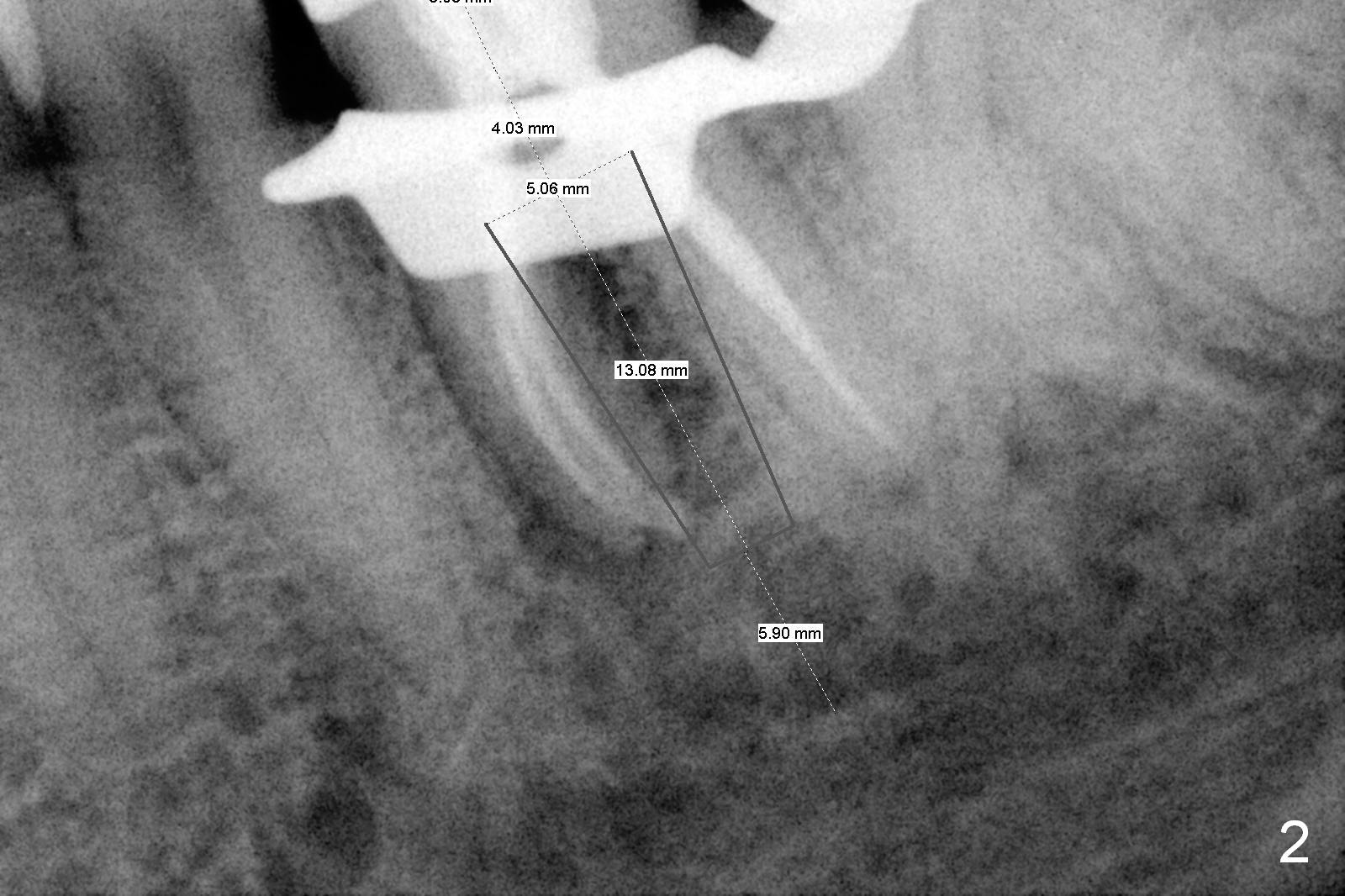
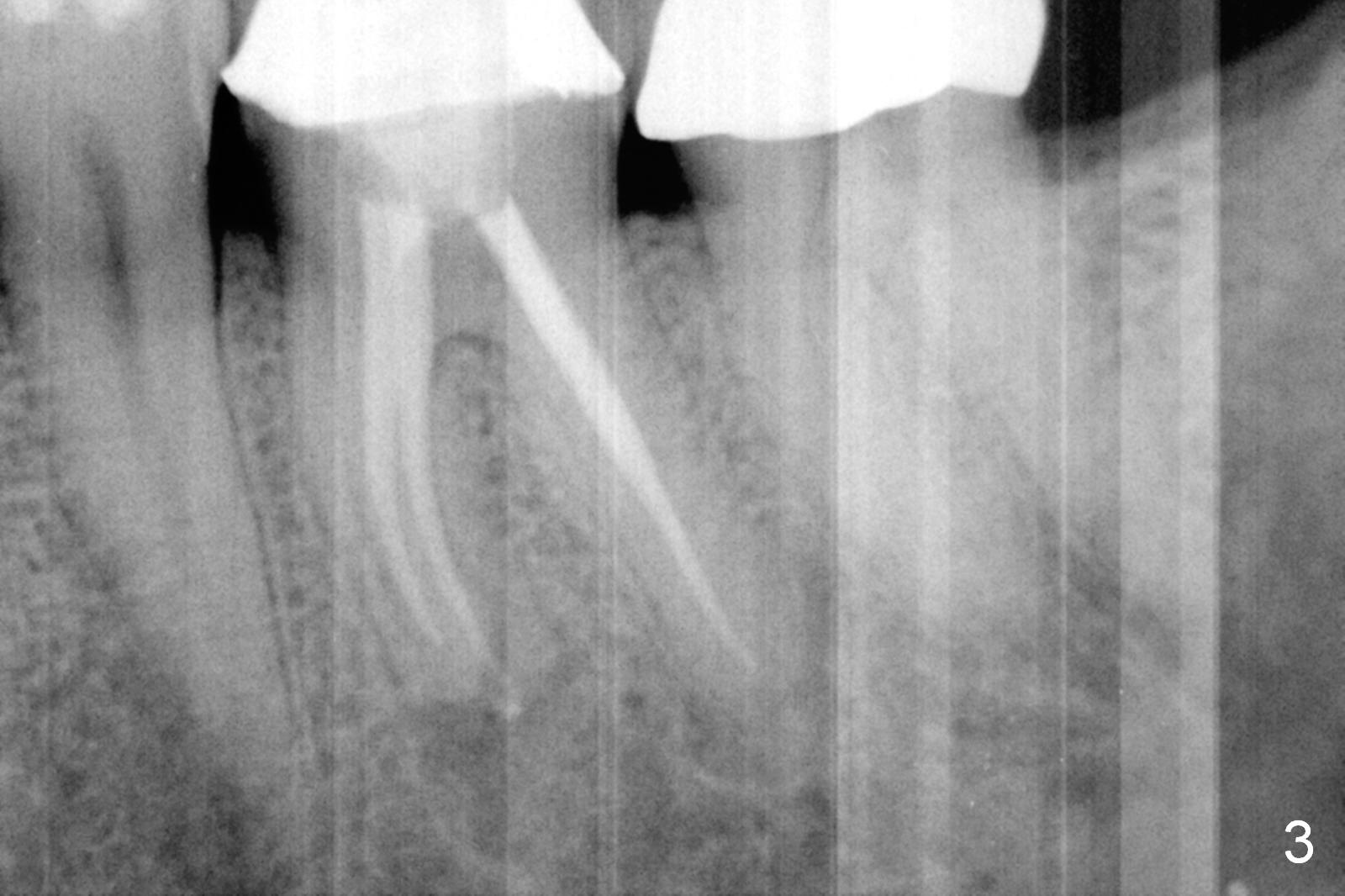
A 50-year-old man had pulpitis at #19 six years ago (Fig.1). RCT looks well filled (Fig.2). Recently he returns with severe toothache, involving the tooth #20 (Fig.3). There is no sign of crack tooth. Endo referral is recommended, but he would rather have it extracted first, since he is going to buy insurance near the end of the year for implant. He returns for extraction, since he could not sleep well the previous night. After block and periodontal ligament injection with two carpules of Lidocaine, extraction proves to be painful. A carpule of Marcaine is administered for block. While waiting for anesthesia to settle in, he suddenly agrees for immediate implant, since he had history of failure of bone graft after extraction at #30. The site needs regraft. The whole treatment takes two years.
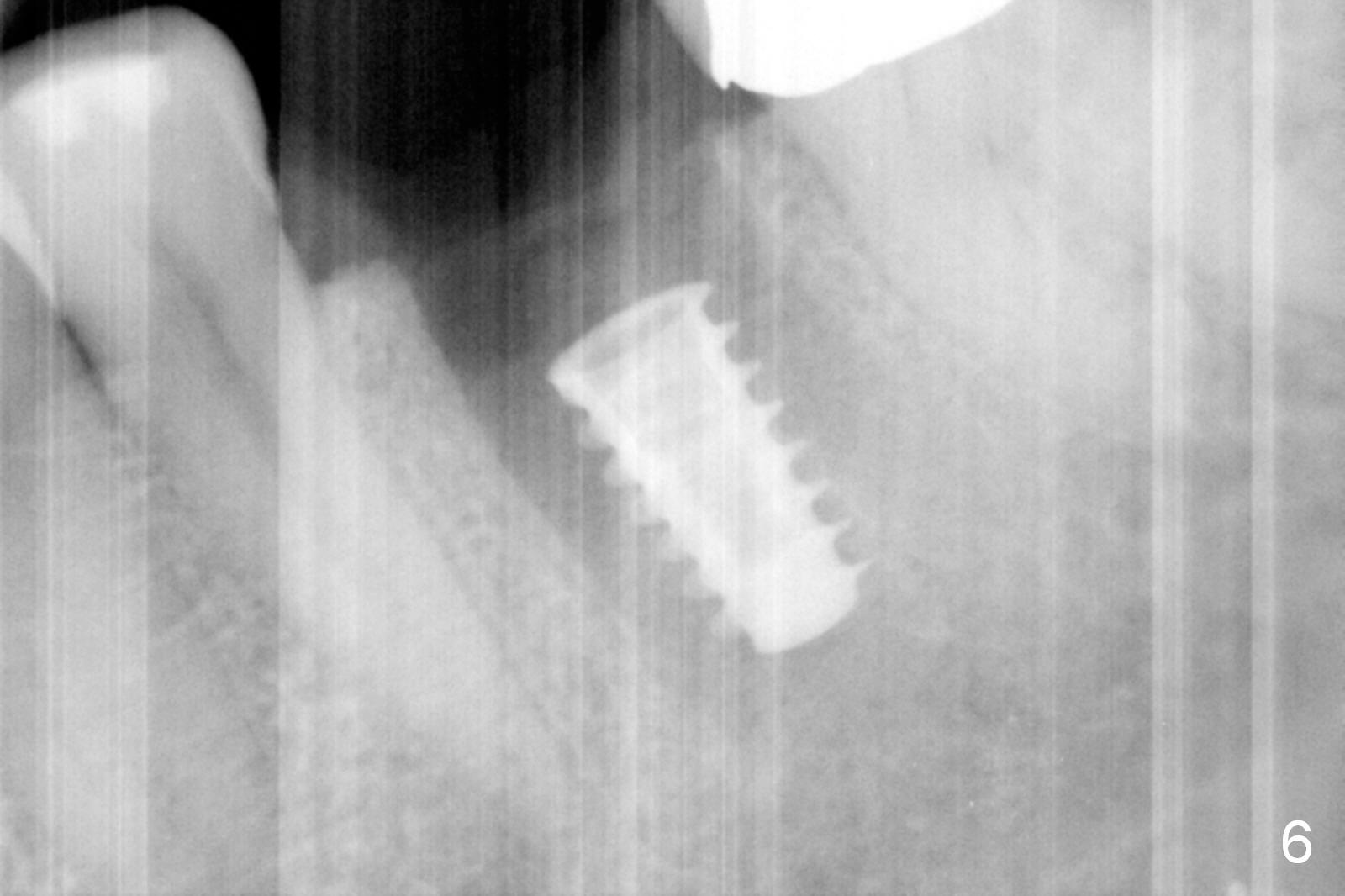
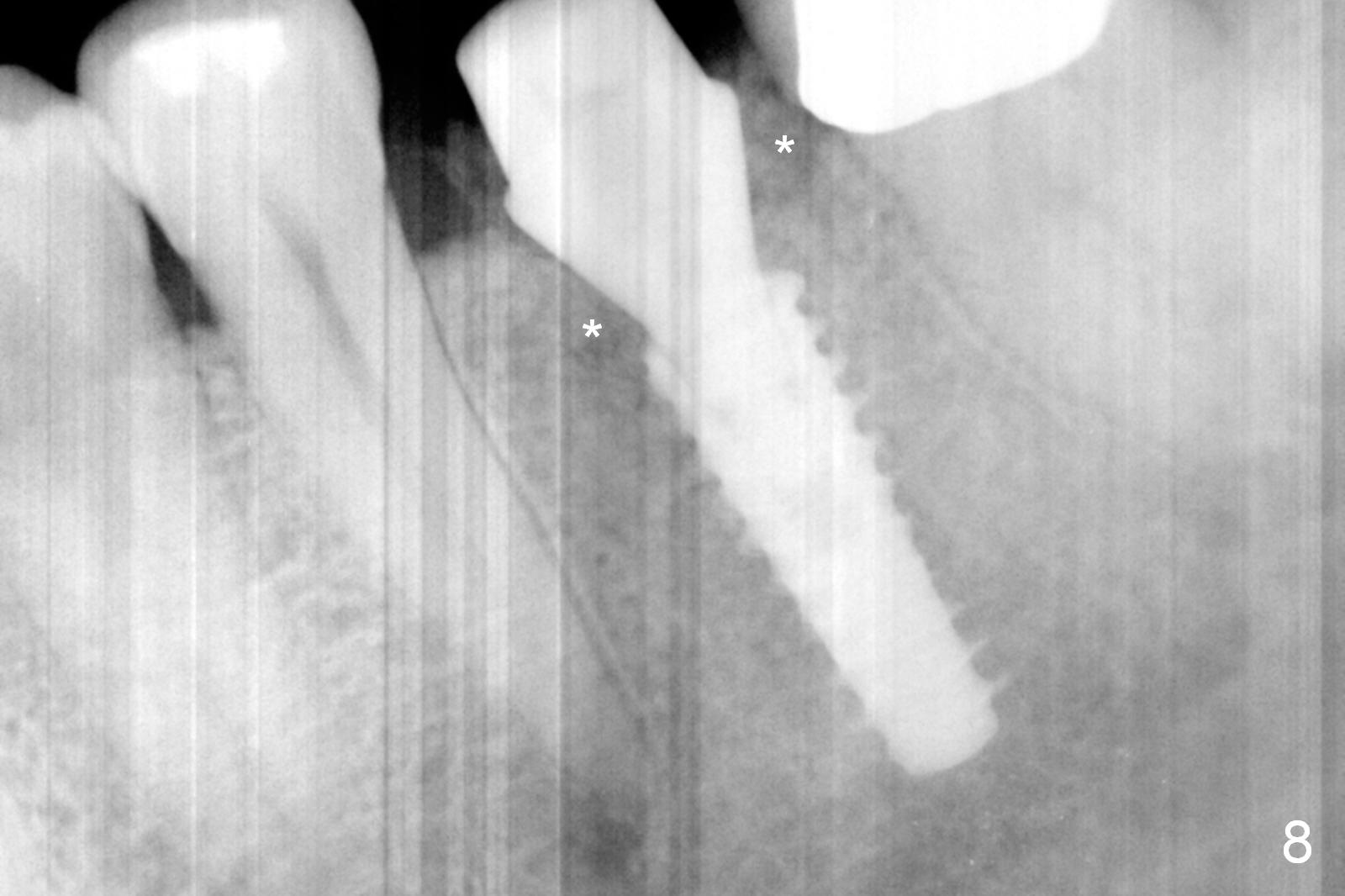
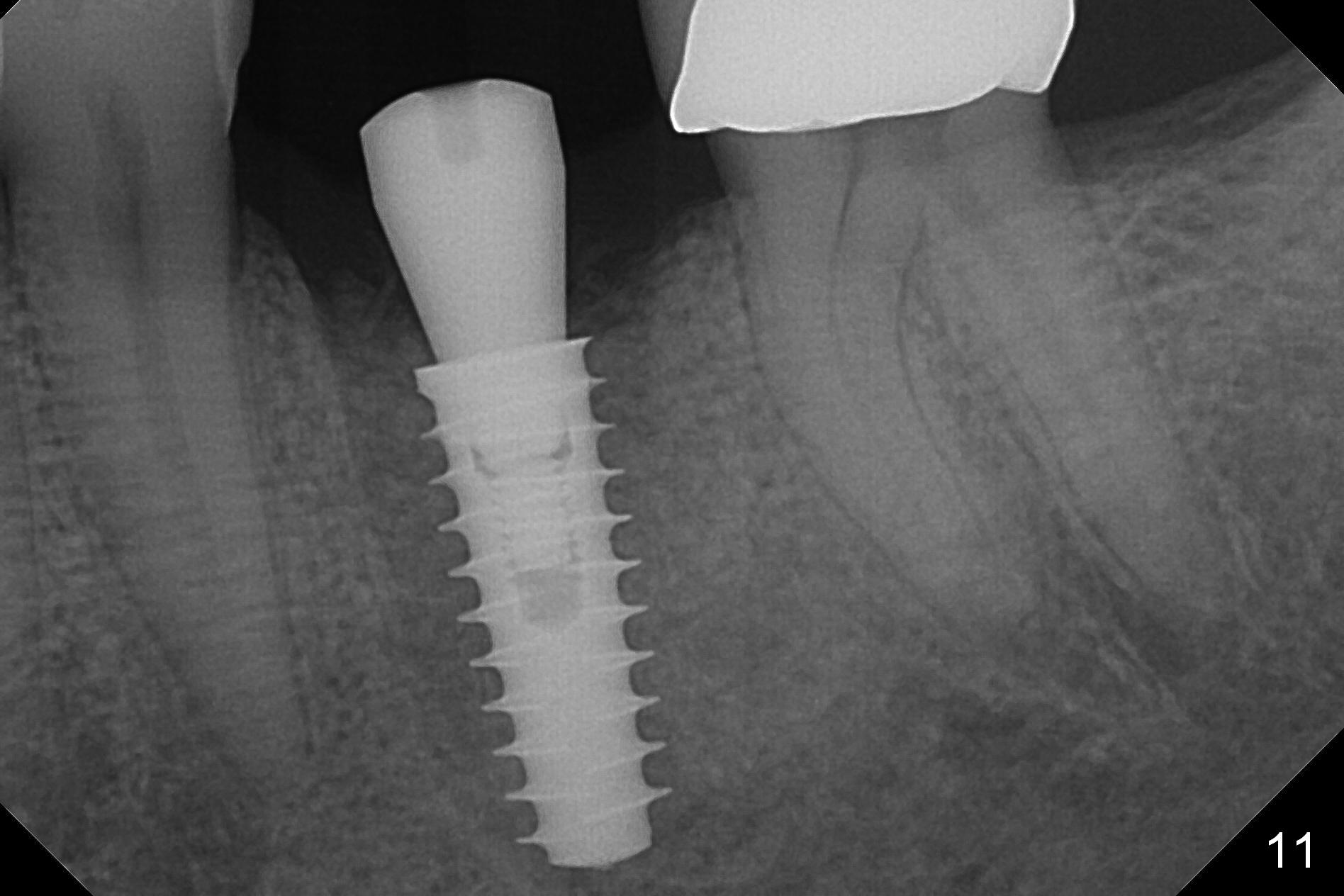
The tooth #19 is easy to get loose, but it cannot be luxated. After sectioning and extraction (Clindamycin), the septum is found to be thin (Fig.4). A surgical fissure bur is used to initiate osteotomy, followed by 1.6 mm pilot drill. It is difficult to use Marking bur (wobbling over the basically pointed septum). It is impossible to use 4.3 mm Magic Drill (MD, one drill system), since it jumps. The smallest MD has to be used (2.8 mm). When the next drill (3.3 mm) is being used for 13 mm with stopper (Fig.5), the patient experiences transient pain. The depth is suggested from the design in Fig.2. The thin septum appears not to be a reliable landmark. When block anesthesia is administered, the initial depth should be shortened. The drill appears to be close to the Inferior Alveolar Canal (Fig.5). Then the depth changes to 11 mm with the following drills (3.8 and 4.3). The mesial and distal walls of the septum are gradually perforated. A 5x9 mm dummy implant is placed only after using 4.8 mm drill (Fig.6). The implant appears to be short. When a longer implant is placed (5x11 mm), it does not easily enter the osteotomy, either sliding into the mesial or distal socket with the implant separating from the implant driver. It appears that a premount implant is appropriate in this situation. When the 5x11 mm implant is finally seated with stability, it is 6 mm apical to the gingival margin. The longest cuff of IBS abutment is 4 mm. A longer implant is needed (Fig.7, 5x13 mm). Placement is not easy as mentioned above. Insertion torque is <20 Ncm when the patient experience a little discomfort. A 6.5x4(4) mm pair abutment is placed (A), apparently proper for restoration. Allograft is placed (Fig.8 *) prior to immediate provisional. The patient complains of bad smell from the site 24 days postop. When the provisional is removed, the abutment is found to be mobile. When the latter is removed with local anesthesia, bone graft granules are attached to the socket above the lightly mobile implant (Fig.9). In fact the latter appears to be stable after a few turns by finger. A healing screw is placed; the socket is closed with collagen plug and 4-0 Chromic gut sutures (Fig.10). It appears that a larger implant should have been used to achieve higher torque. Two months later (3 months postop), the coronal end of the implant is partially exposed. A 5x4 mm healing abutment is placed. It appears that the implant is stable. The implant appears to have osteointegrated 4 months postop (Fig.11). Impression is taken.
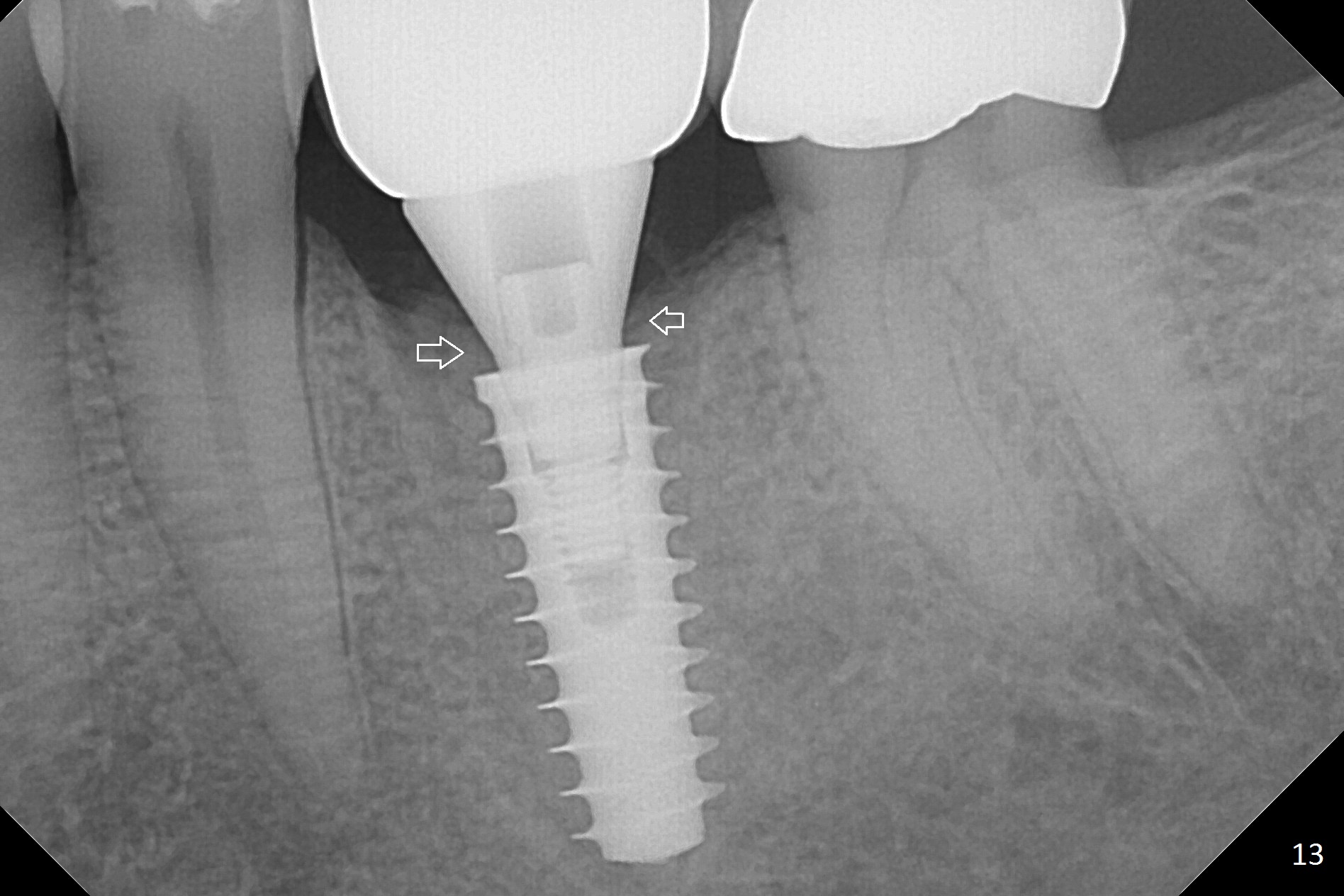
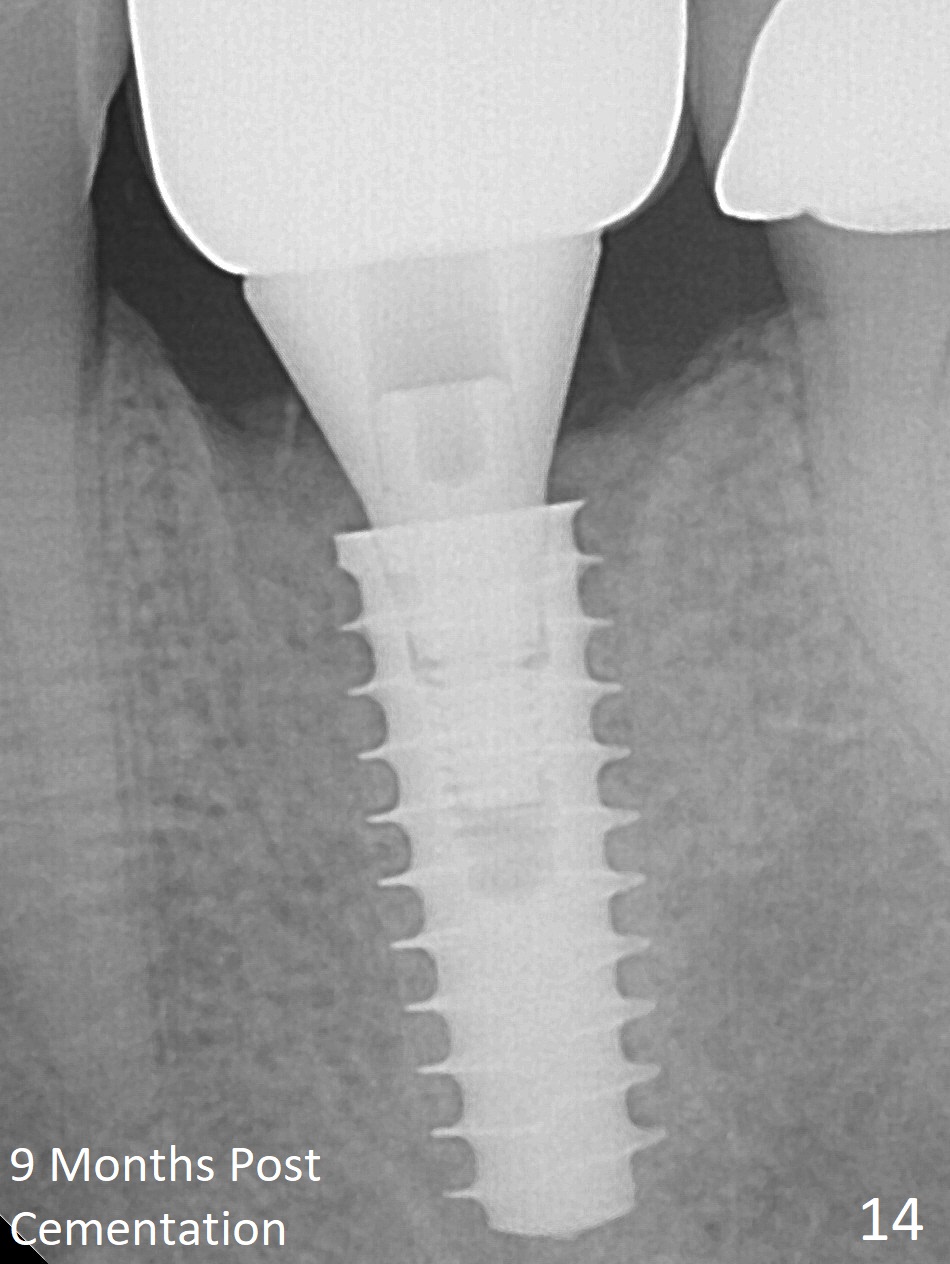
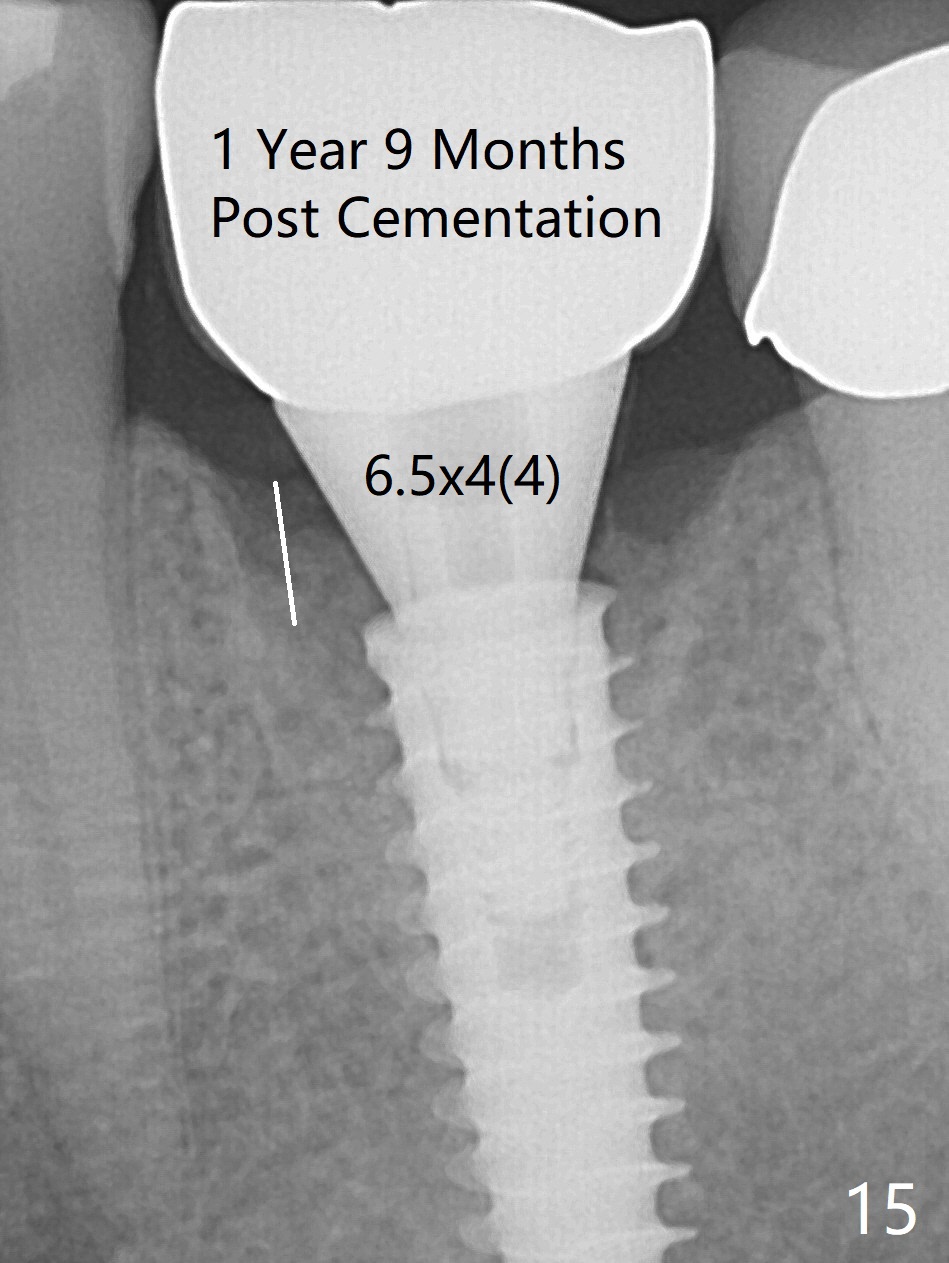
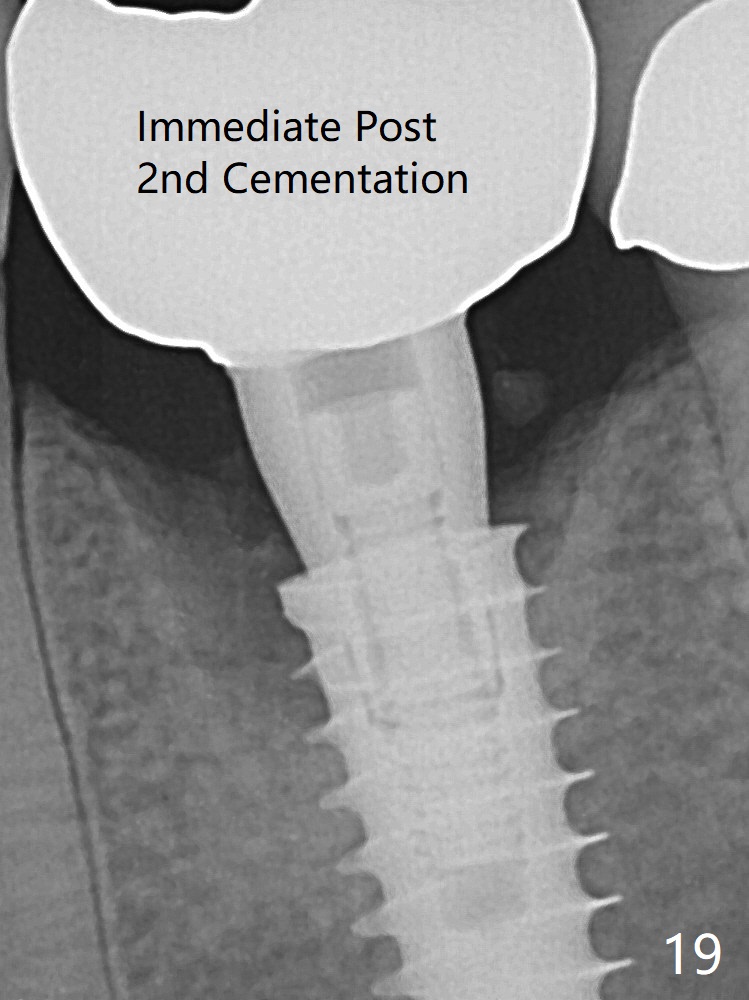
The gingiva looks healthy 8 months postop (3 months post cementation (after abutment screw retightening and addition of porcelain to proximal surfaces, Fig.12). New bone has apparently covered the implant plateau (Fig.13 arrows). Bone density between threads increases 9 months post cementation (Fig.14). There is 2 mm bone superior to the implant plateau mesial and distal 1 year 9 months post cementation (Fig.15,16). The crown/abutment is loose 3 times (3 months (Fig.14), 11 months (between Fig.14 and 15) and 2 years 3 months post cementation). In spite of being stable 3 years 10 months post cementation, a smaller abutment is placed (Fig.17 (PA), 18 (BW)) with impression for a new crown. After intraoral cementation, the new crown/abutment is removed for residual cement removal. When the complex is reseated, it is not smooth, probably due to proximal undercut. Fortunately the abutment appears to be completely seated, followed by 20 Ncm torque (Fig.19).
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
1st Year
Torque
Xin Wei, DDS, PhD, MS 1st edition 10/18/2016, last revision 05/20/2021