

|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|||
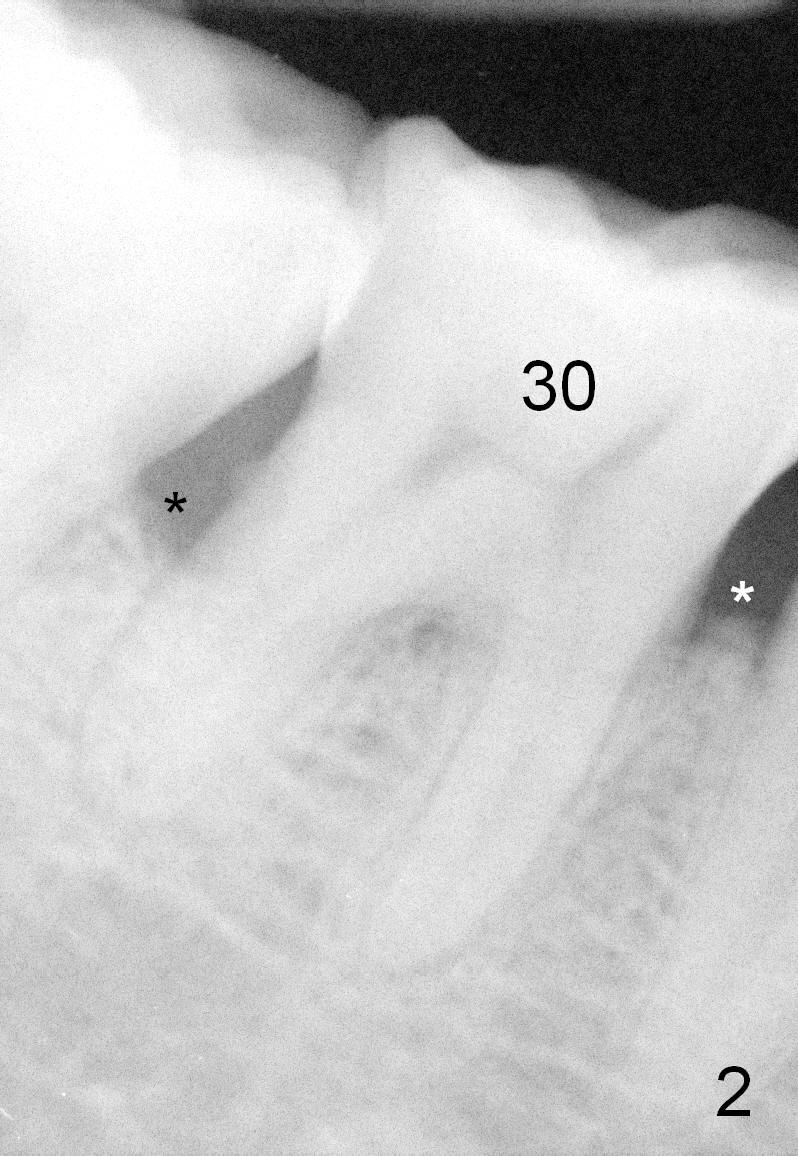
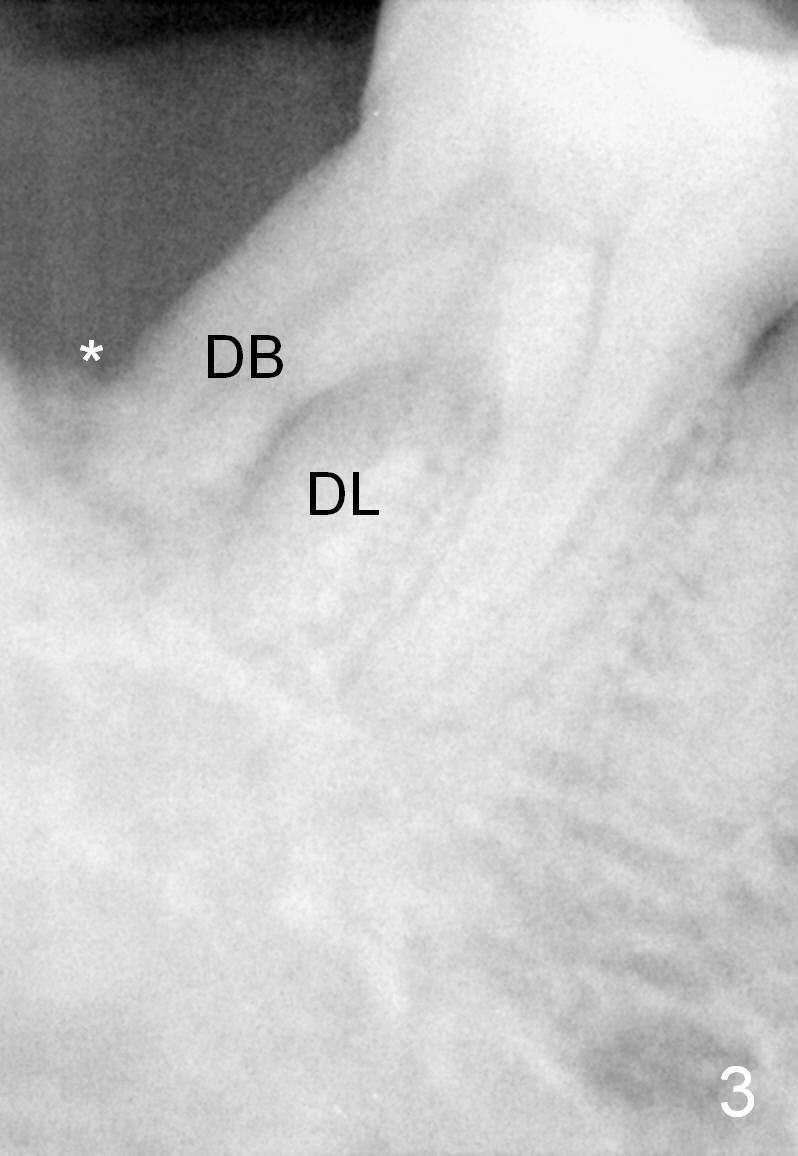
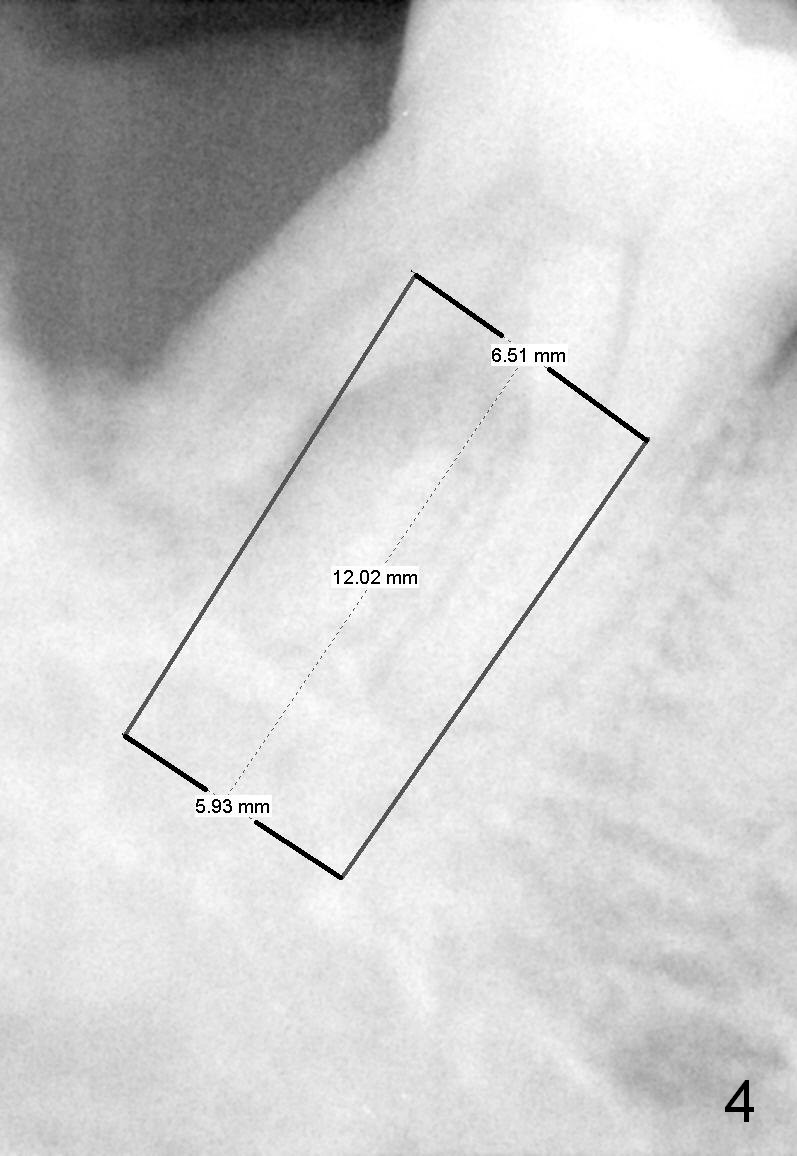
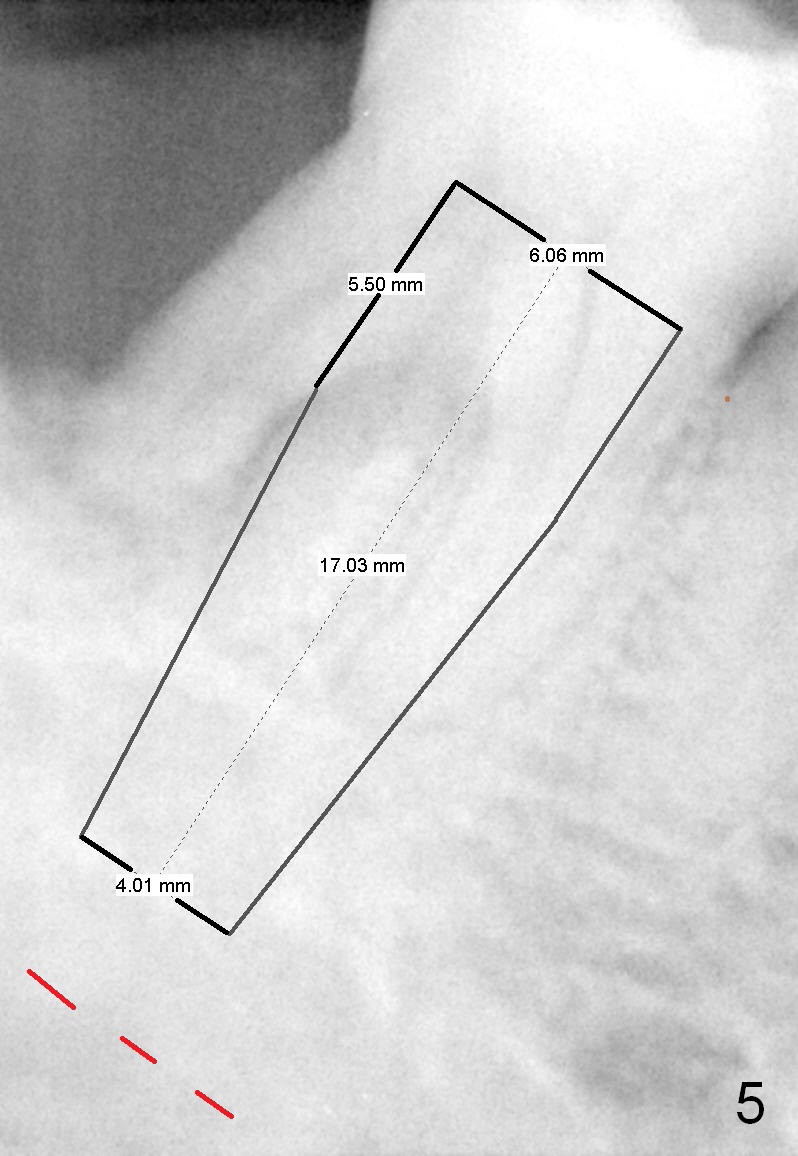
Uneven Mesiodistal Bone Level
One year and a half years ago, the tooth #31 of a 48-year-old man had infection (Fig.1 *) and was extracted without implant. There was more bone loss in the distal of #30 than in the mesial (Fig.2 *). Recently the patient returns with infection at #30 distally with severe bone loss (Fig.3 *). An immediate implant is to be placed mainly in the mesial socket (Fig.4 (bone-level), Fig.5 (tissue-level)).
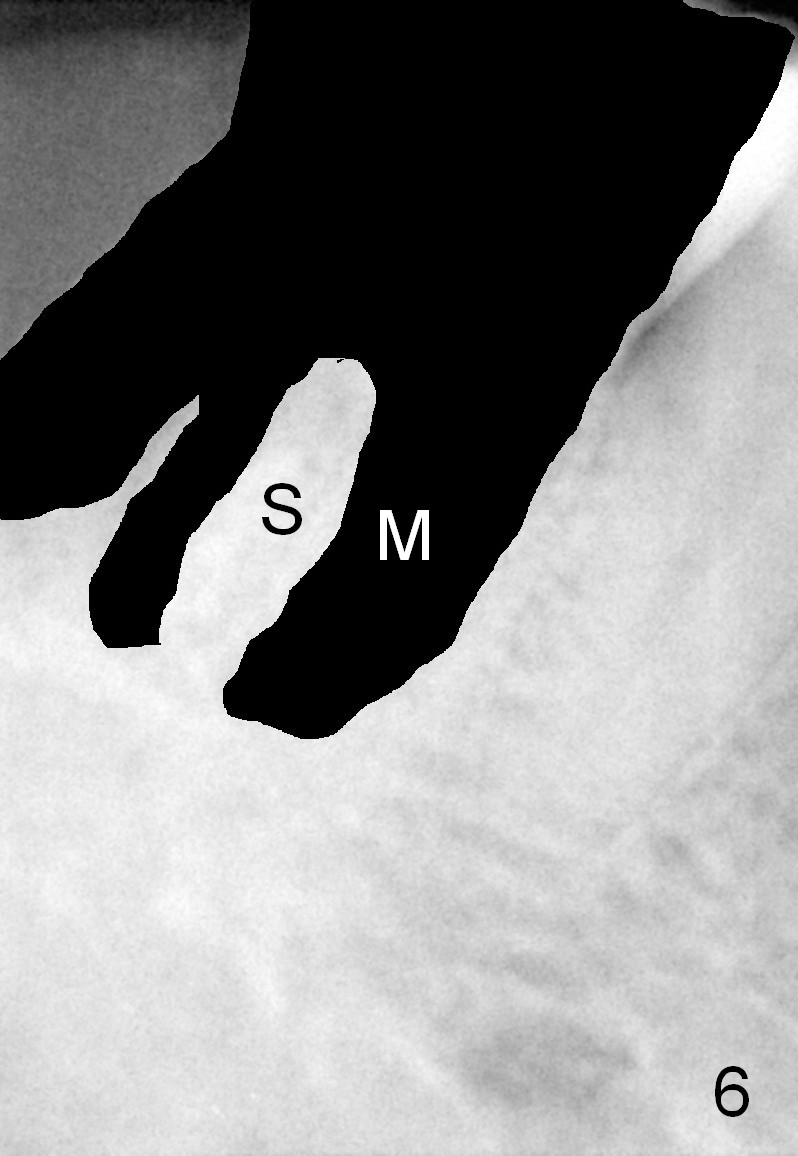
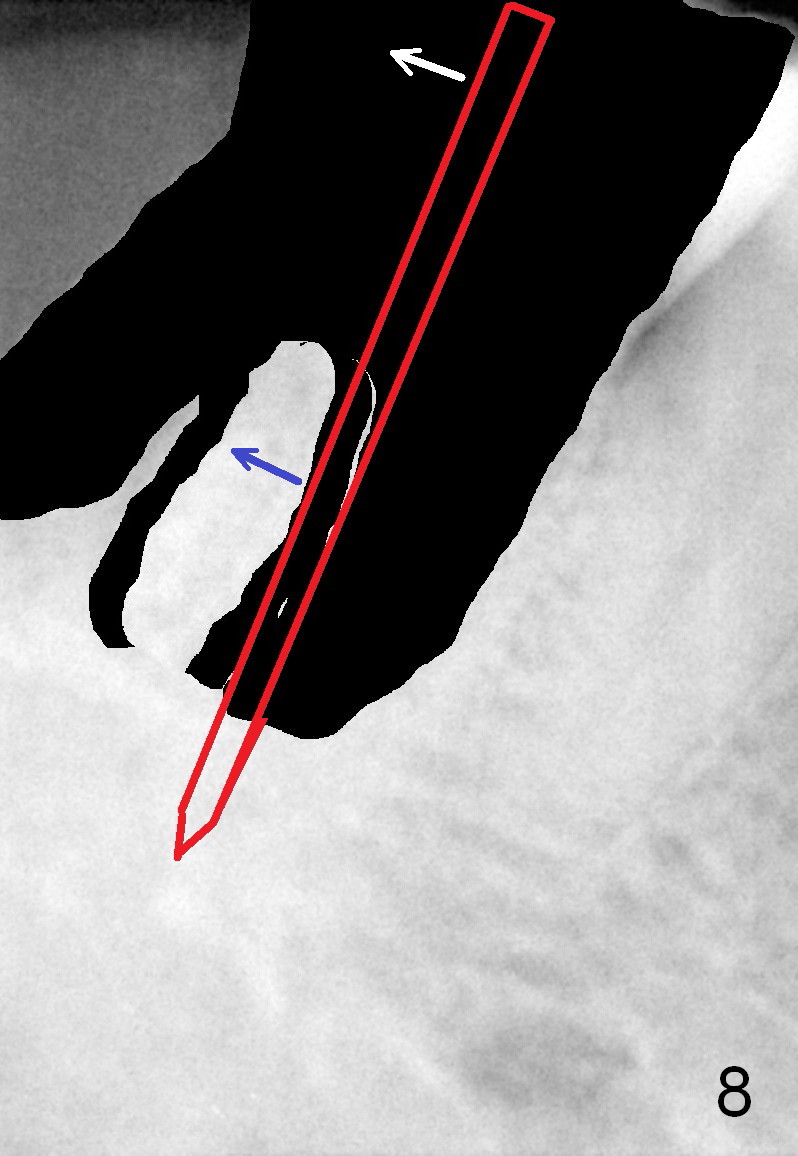
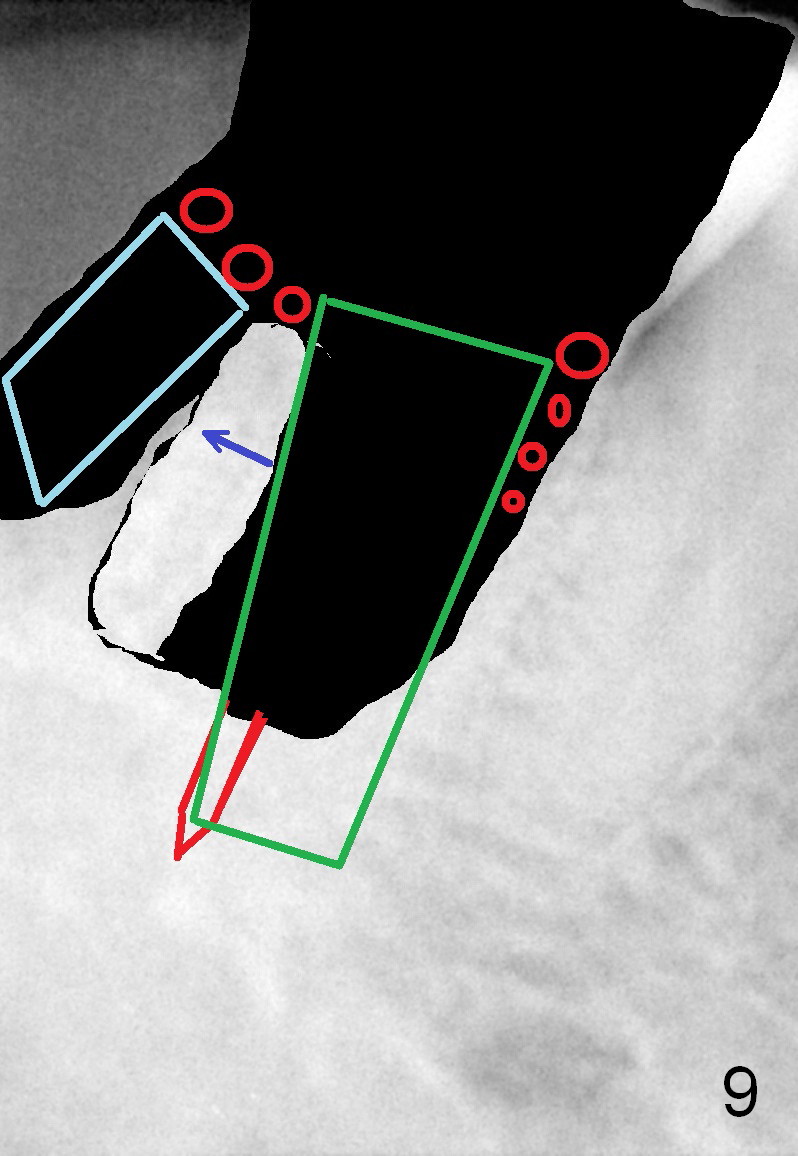
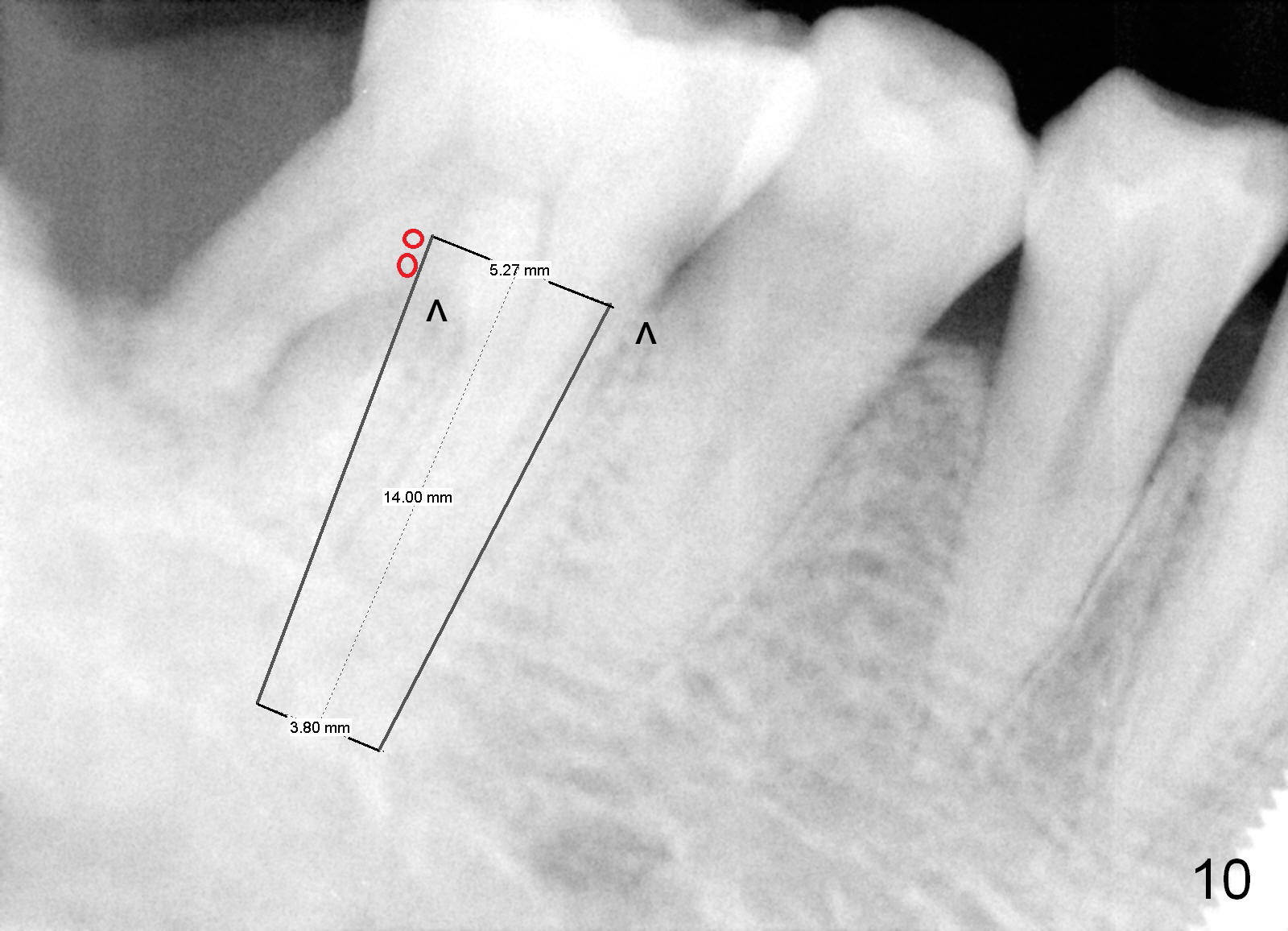
Fig.6 is an illustration after extraction (S: septum; M: mesial socket). Osteotomy is initiated with a pilot drill in the distal aspect of the mesial socket or the mesial aspect of the septum (Fig.7). The osteotomy is enlarged with osteotomes; at the same time the septum is being pushed distally (Fig.8 blue arrow) with leaning the osteotomes distally (white arrow). When an implant is placed, the apex is mainly seated in the mesial socket, while the coronal end is more or less inclined distally for restoration. The apical half of the distal sockets is packed with collagen plug or dressing, whereas the remaining sockets and coronal exposed threads are filled with bone graft (Fig.9,10 red circles). An incision is made if needed for better visibility. The most coronal socket is going to be obliterated by a cemented or healing abutment. Does the treatment planning help surgery?
Return to Lower Molar Immediate Implant,
Dr.
Wu
Xin Wei, DDS, PhD, MS 1st edition 03/21/2015, last revision 04/04/2015