.jpg)
|
|
|
|
|
|
|
|
|
Treatment Planning for Long-Termed Missing Molars
A 44-year-old lady requests restoring missing teeth at #14 (Fig.1 *) and 30. There is no buccopalatal width deficiency at #14, but the mesiodistal space needs to be expanded by distalizing the tooth #15 (arrow) after extraction of the tooth #16 (x). Placement of a longest mini-implant at the tuberosity area after socket healing is anticipated.
At the site of #19, the biggest challenge is the buccolingual width. An incision will be made to determine the width. If it is less than 5 mm, consider Ridge Split. Otherwise, place a UF implant at restorative position and bone graft. Initial depth is 10 mm.
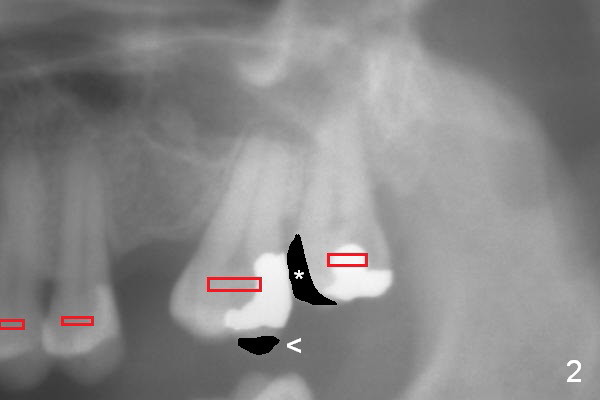
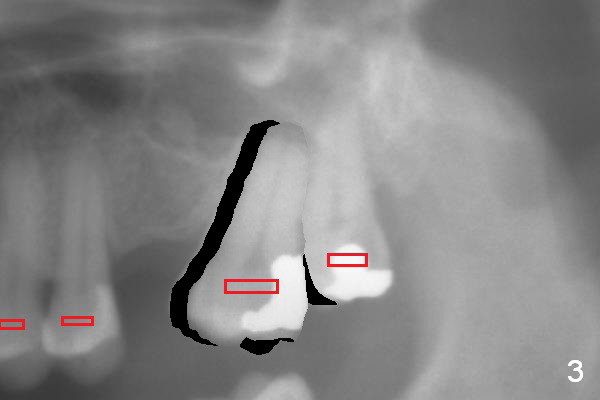
A second option for #14 is segmental orthodontic treatment. Initially keep the tooth #16 and mesial reduction (Fig.2 *). Place brackets between #11 and 16 (Fig.3 red) and open coil spring between #13 and 15.
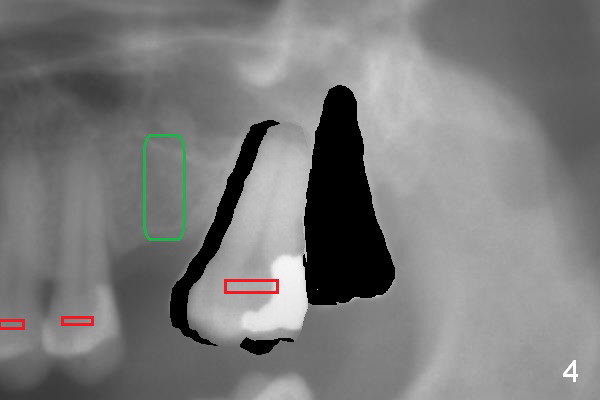
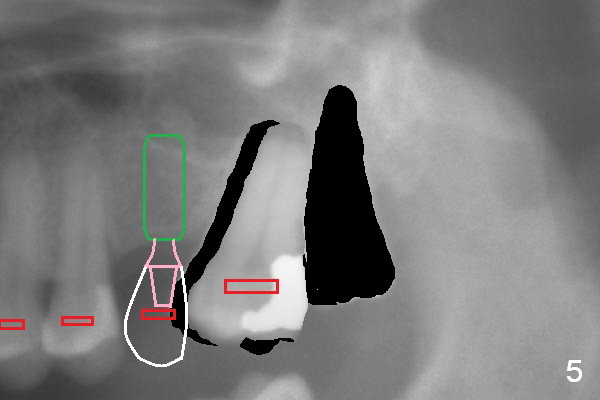
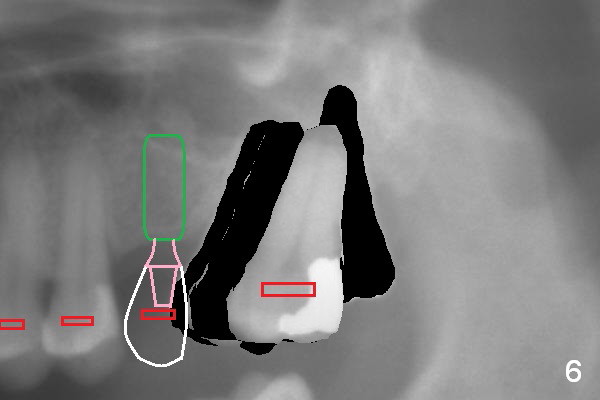
When the tooth #15 is distalized (Fig.3), place an implant at #14 (Fig.4 green), parallel to the tooth #13 and extract #16 (black). When the implant osteointegrates, place an abutment (Fig.5 pink), provisional (white) and bracket at #14. The implant is used as an anchorage to further distalize #15 until the latter reaches the normal position (Fig.6). CT study shows how much the tooth movement is needed prior to implantation.
Return to Lower Molar Immediate Implant, IBS
Xin Wei, DDS, PhD, MS 1st edition 11/22/2015, last revision 10/27/2016