



|
|
|
|
|
|
|
|
|
|
|
|
Long Implant
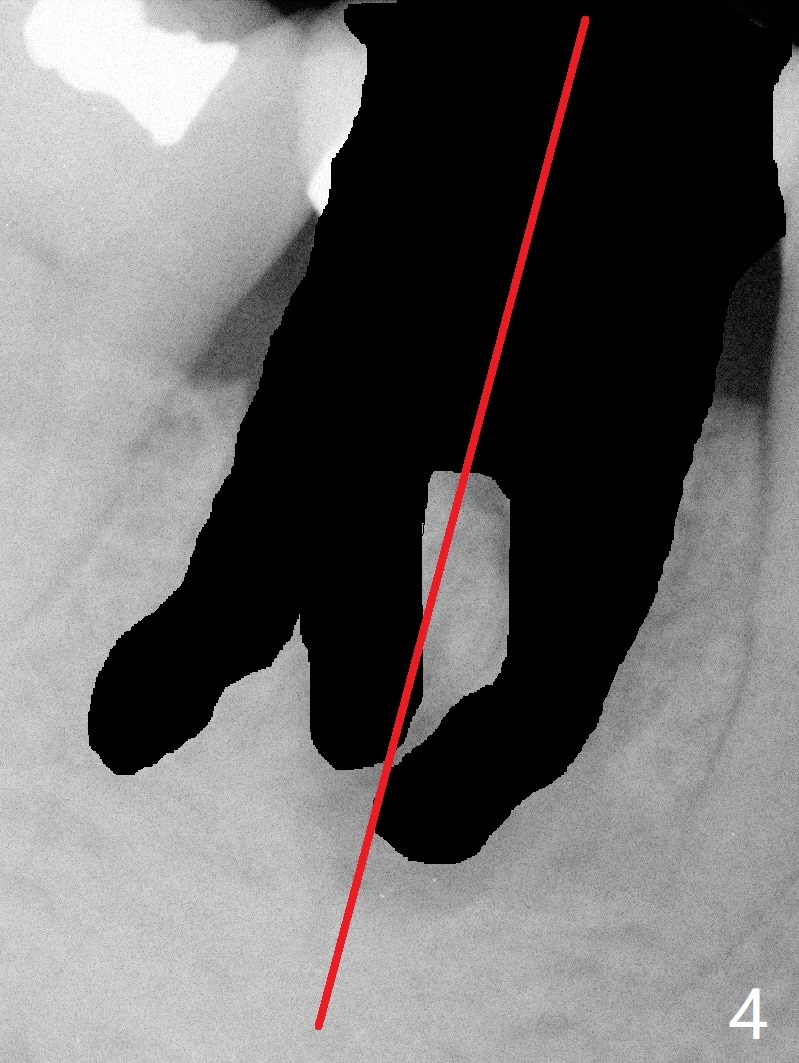
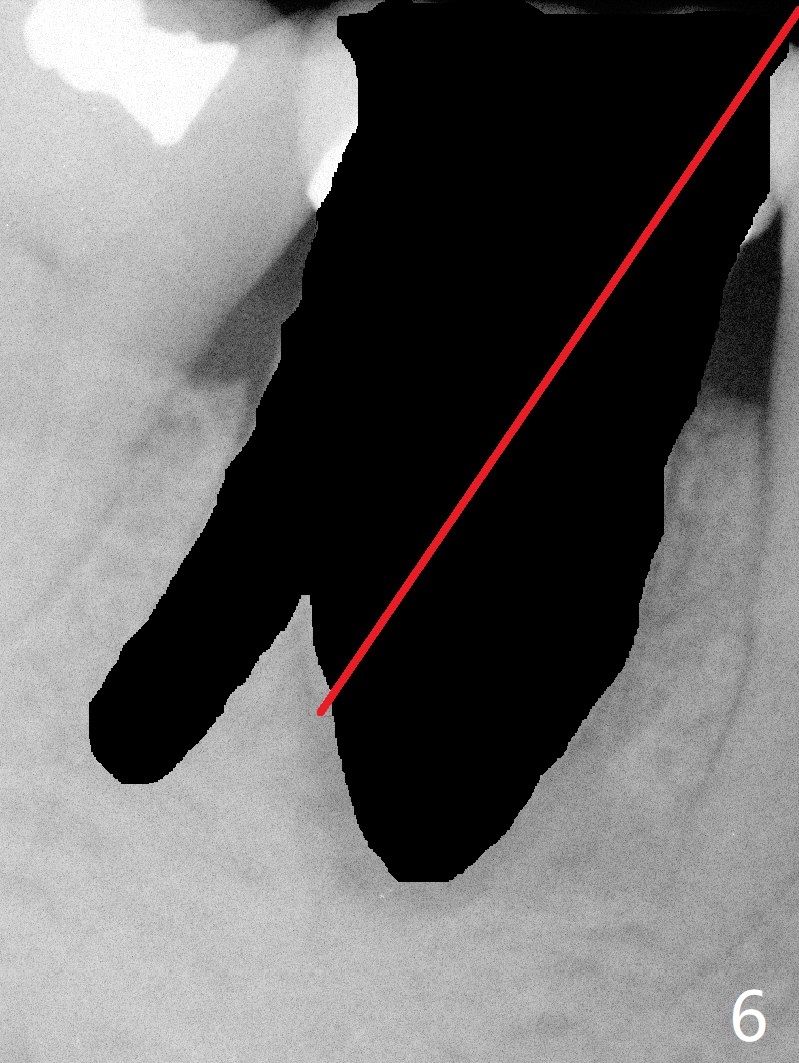
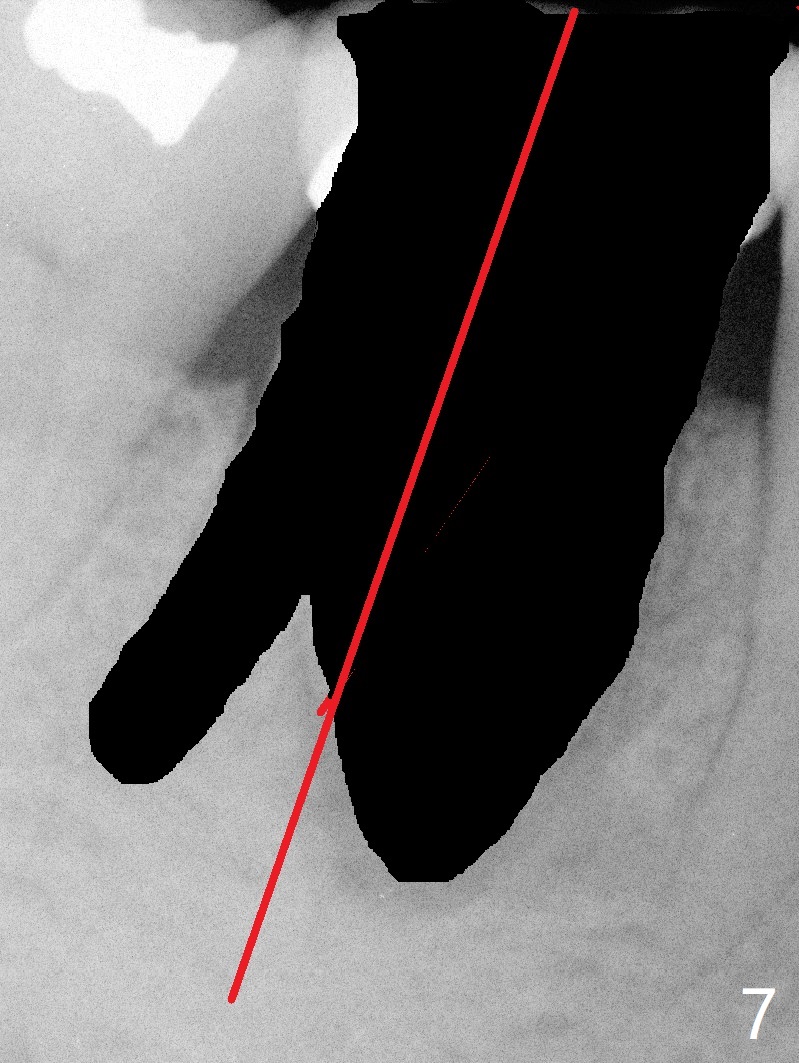
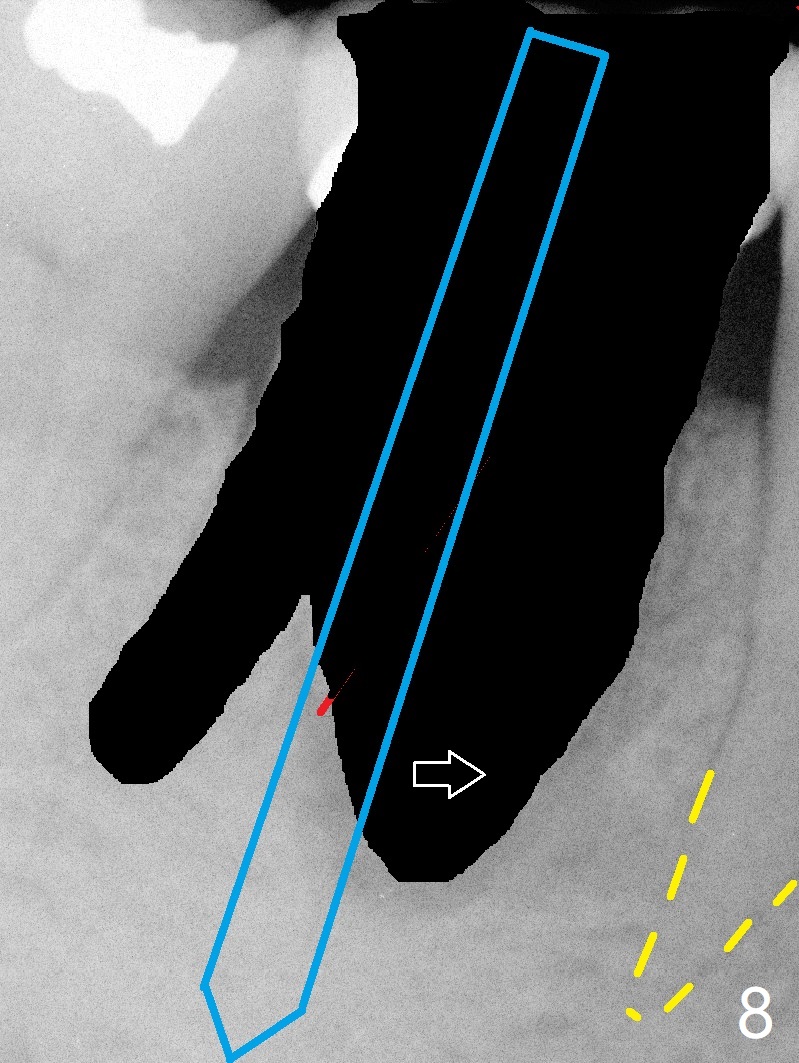
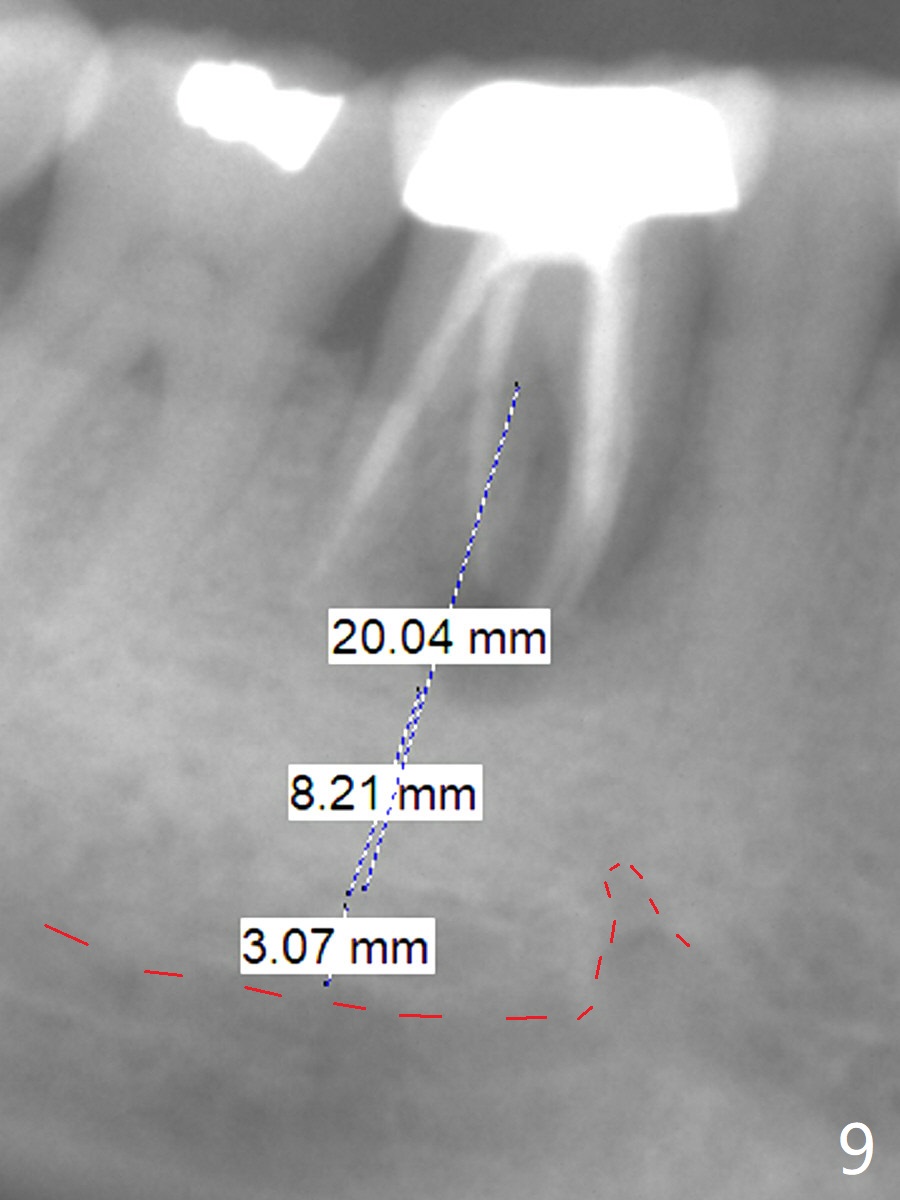
A 55-year-old woman has severe bone loss (Fig.1 with buccal and lingual fistulae) around the mesial (M in Fig.2) and distolingual (DL) roots. If there is a septum after extraction (Fig.3 S), osteotomy will be established in the septum to enhance primary stability (Fig.4). When the septum cannot be saved (Fig.5), osteotomy is to be initiated in the septal slope oblique (Fig.6 <). The osteotomy will be straightened once an entry is made (Fig.7). The initial osteotomy is slightly distal, since as osteotomy increases (Fig.8 blue), it tends to shift mesial (arrow). In addition, the apex of the 2nd bicuspid tilts distal (yellow dashed line). Depth of osteotomy is 20 mm (crest, Fig.9) or 18 mm (septum) so that 8 mm of the native bone can be obtained with 3 mm clearance from the Inferior Alveolar Canal (red dashed line). PRFx2 is required (seems not done).
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), IBS, No Antibiotic Xin Wei, DDS, PhD, MS 1st edition 10/07/2017, last revision 04/26/2020