

|
|
|
|
|
|
|
|
|
|
|
|
|||
Why Does Delayed Implant Fail So Easily?
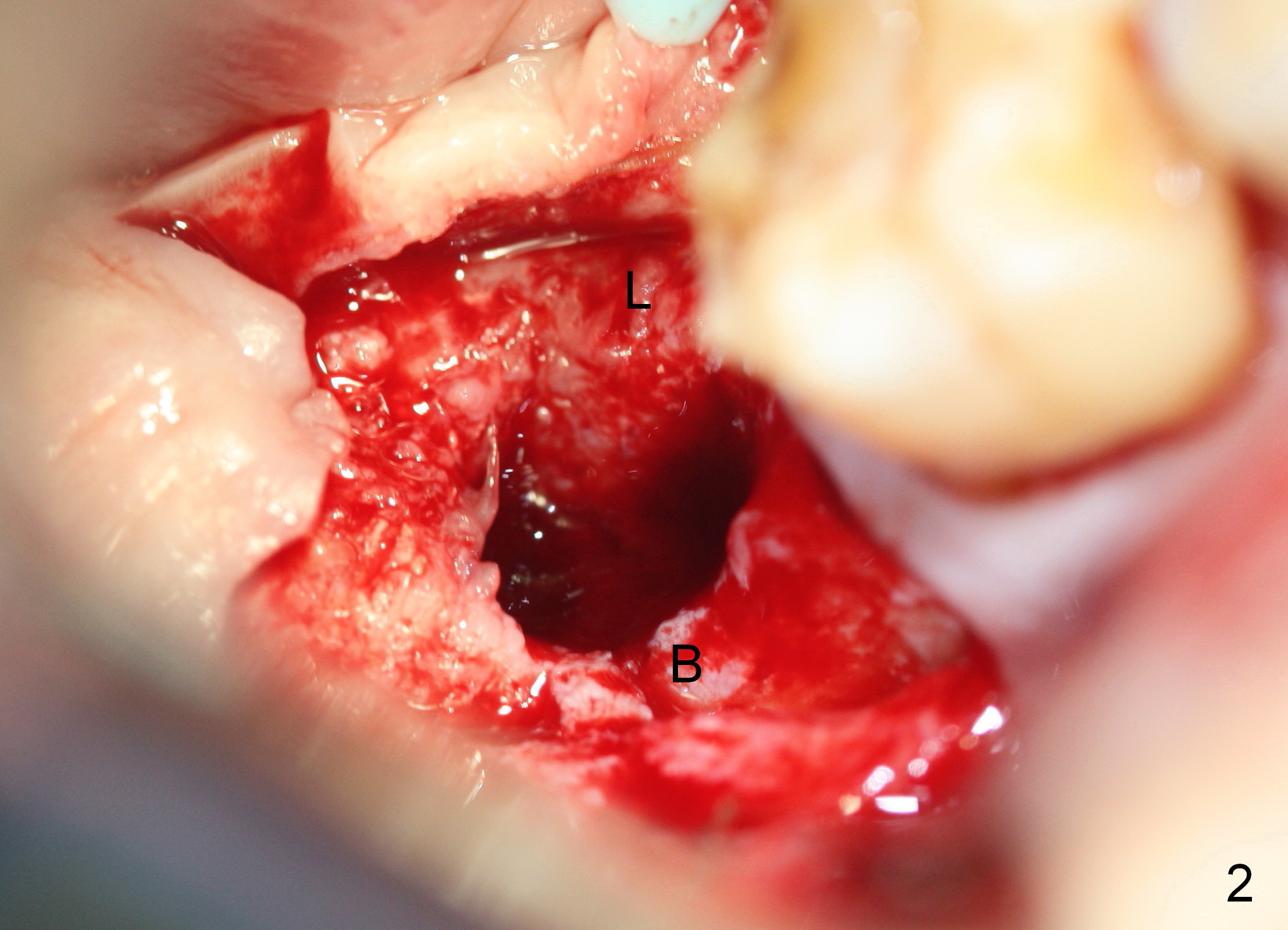
A delayed implant becomes loose 1 month post placement. There is purulent discharge from the implant sulcus. The implant is removed and the site is irrigated with normal saline. Smoking and poor oral hygiene are possible contributing factors. The patient returns 1.5 months post implant removal; a PA is taken (Fig.1). The site bone density is low. When the site is exposed half a month later, the buccal plate is found to be low and thin (Fig.2 B). It may be caused by the 1st flapless placement. The implant must have been placed buccally.
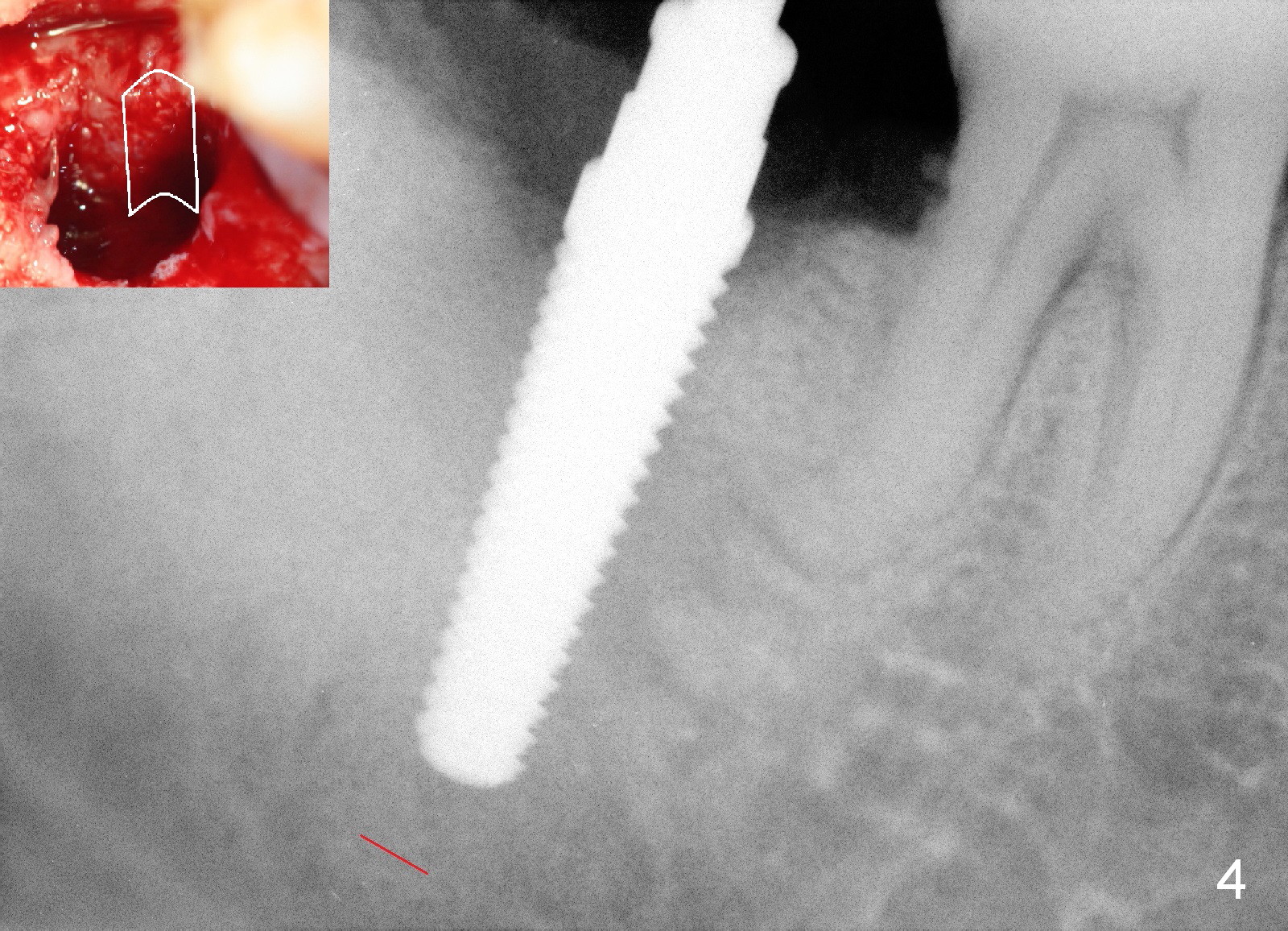
A 2nd problem is that a 2 mm pilot drill has to be 18 mm deep to get a "bite" into the bone. The apical end of the osteotomy is close to the upper border of the Inferior Alveolar Canal (red dashed line).
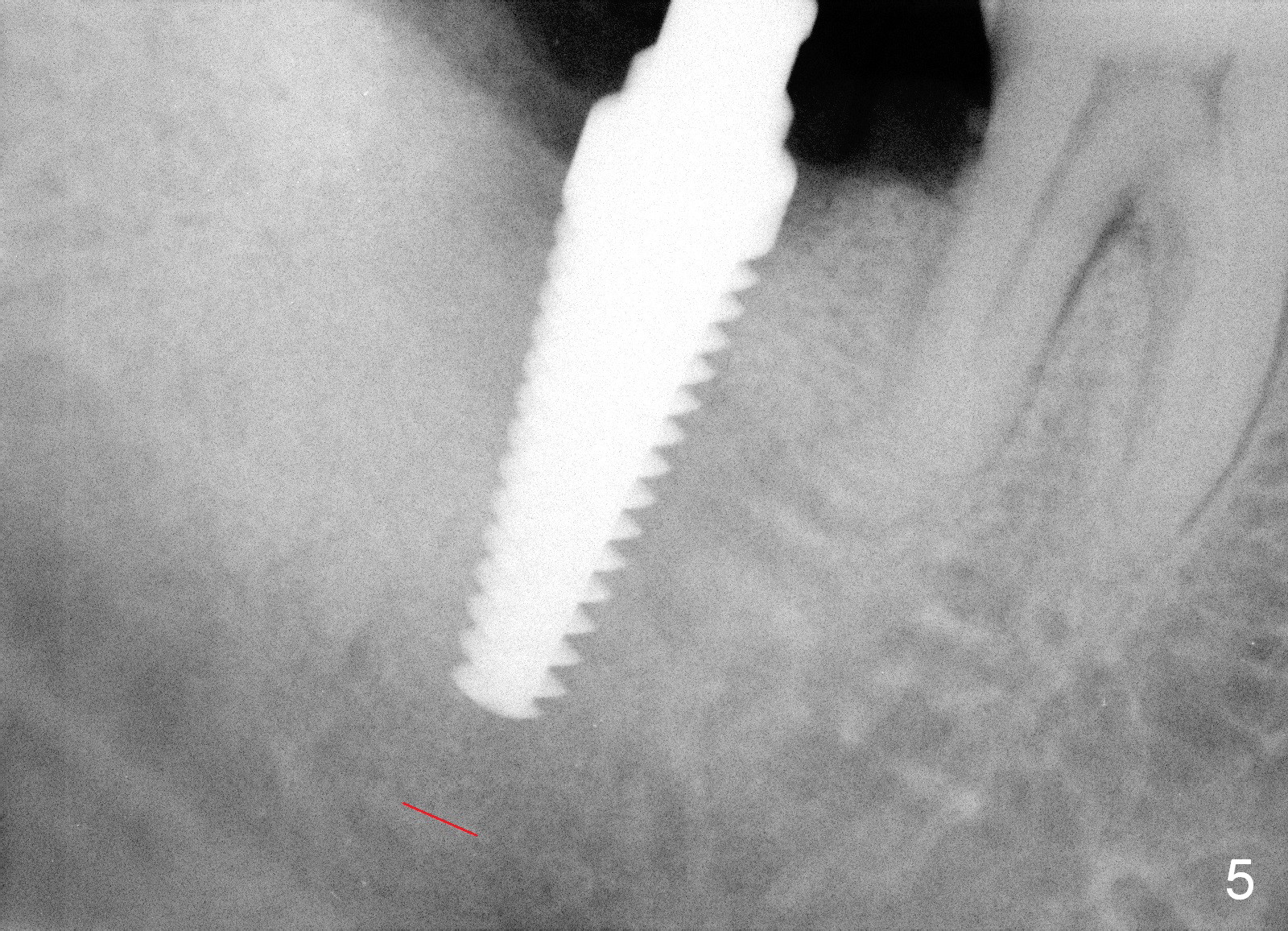
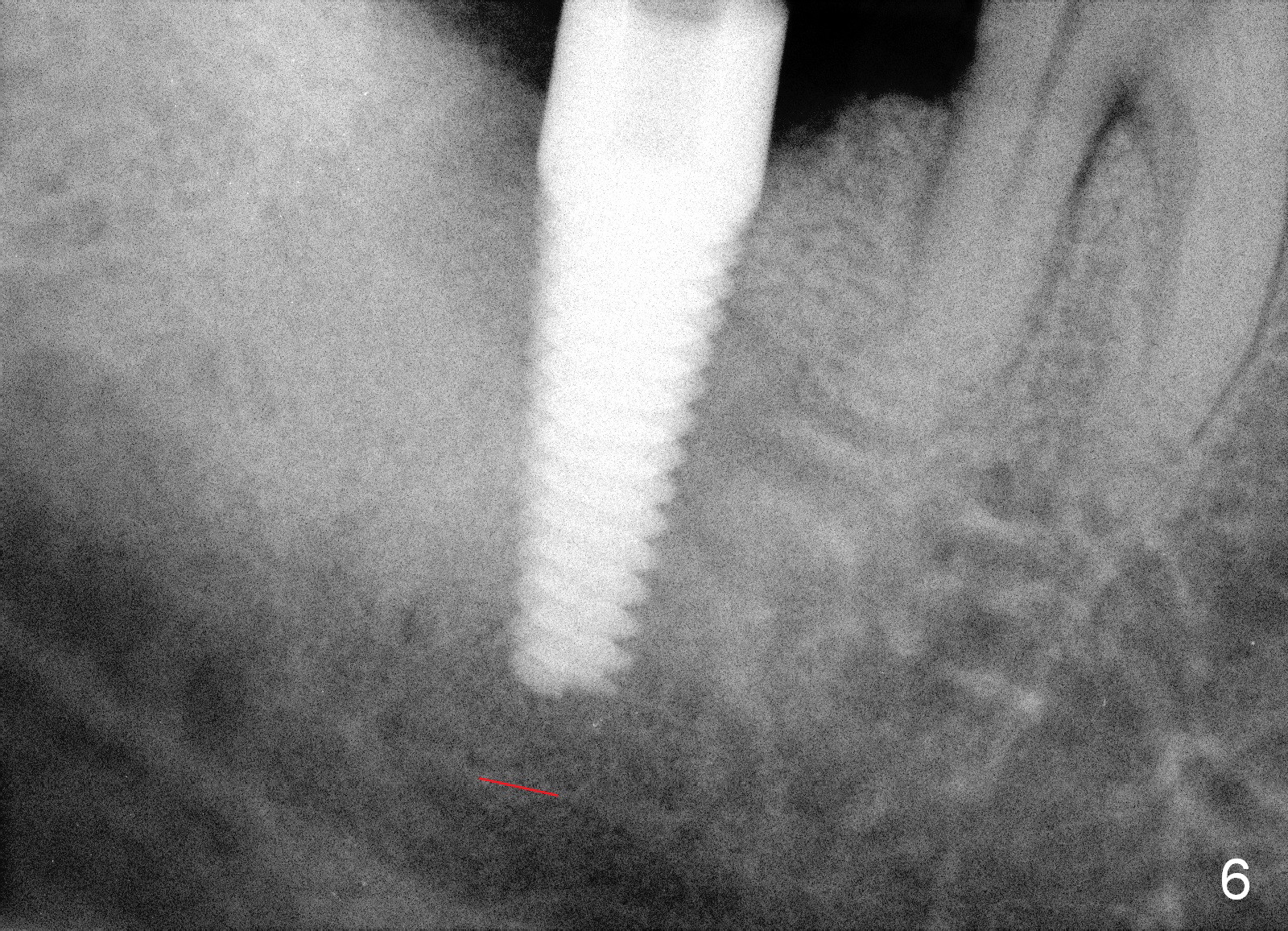
In order to reduce pressure against the buccal plate during late stage of osteotomy and implant placement, a Lindemann bur is used to remove bone from the lingual plate (Fig.4 Insert: white outline). Osteotomy depth is adjusted to 17 mm. When a 5x20 mm tap is inserted, there is distance to the underlying nerve (Fig.4) and stability is fair. Another PA is taken when a 6x20 mm tap is placed with improved stability (Fig.5). When a 7x17 mm tap is being inserted, the patient feels pain, possibly related to expanding the weakened buccal plate. A smaller, but longer implant is finally placed (6x20 mm with insertion torque 55 Ncm, Fig.6). The shortcoming is that primary closure cannot be achieved over the tissue-level implant, whereas bone-level implants available are too short. Allograft is placed buccodistal to the implant, followed by collagen dressing. A 4.5x5 mm abutment is placed; perio dressing is applied. The main reason for previous implant failure is too large an implant is placed too buccally due to poor surgical visibility. The latter is in turn socket healing. Either an incision should be made or an immediate implant should have been placed for a better field.
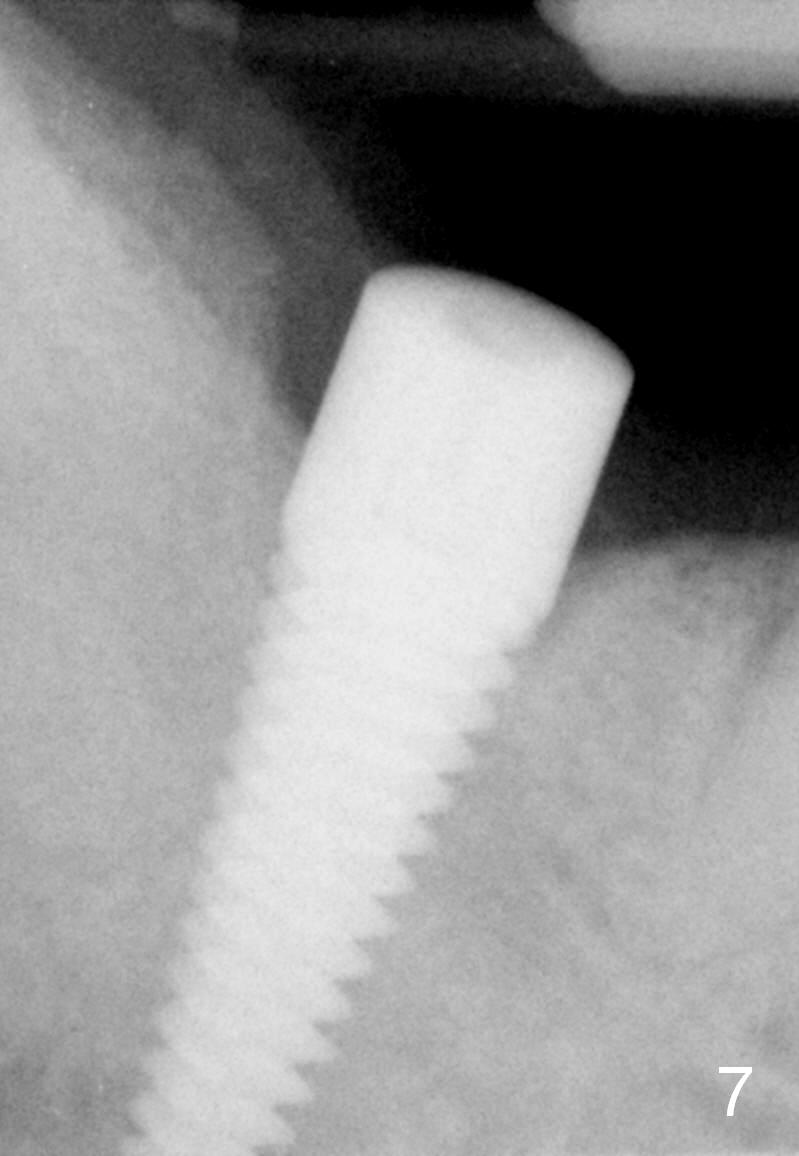
The patient returns 1 week postop. The perio dressing has partially dislodged. The gingiva has not healed. New dressing is applied. Two weeks postop, the dressing is lost. The wound appears not completely heal. The abutment is removed; a cover screw is placed. Smoking appears to retard soft tissue healing, but does not adversely affect implant/bone contact. The patient returns for restoration 8.5 months postop; it appears that the implant has osteointegrated (Fig.7).
Return to Lower Molar Immediate Implant,
Systemic Disease,
Immediate Implant Complications
Xin Wei, DDS, PhD, MS 1st edition 02/23/2015, last revision 12/20/2015