|
|
|
|
|
|
|
|
|
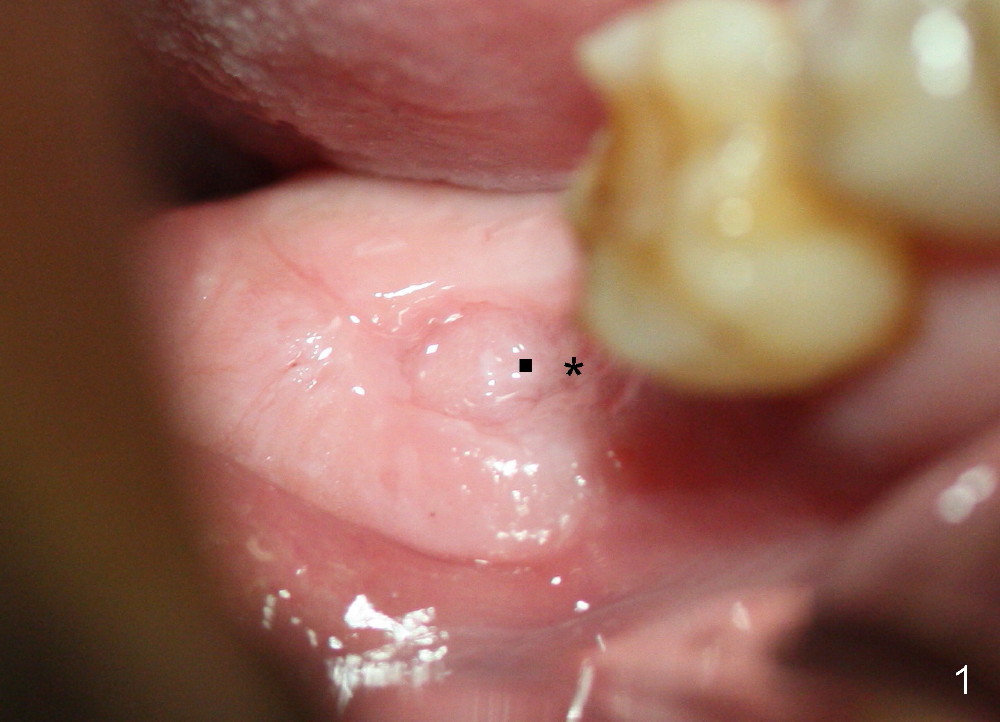
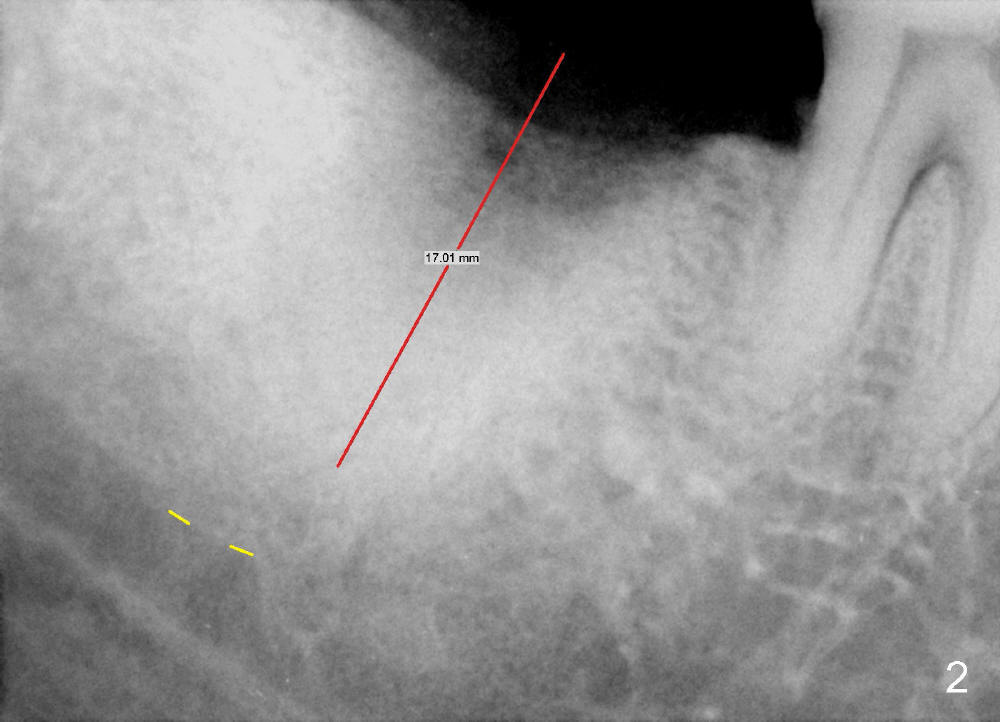
Why To Drill?
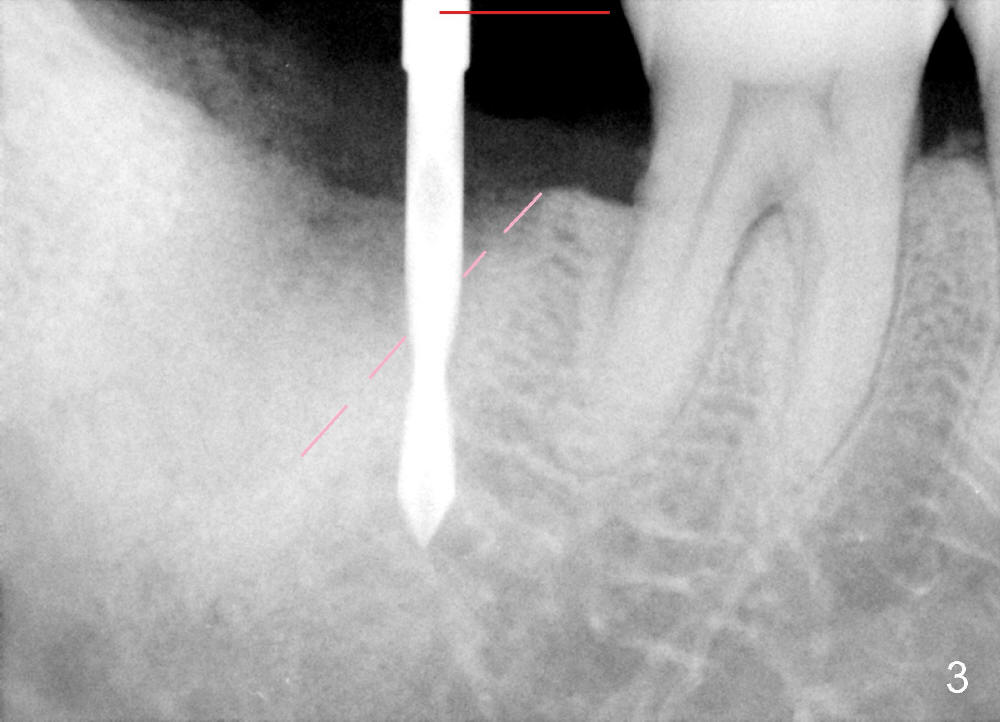
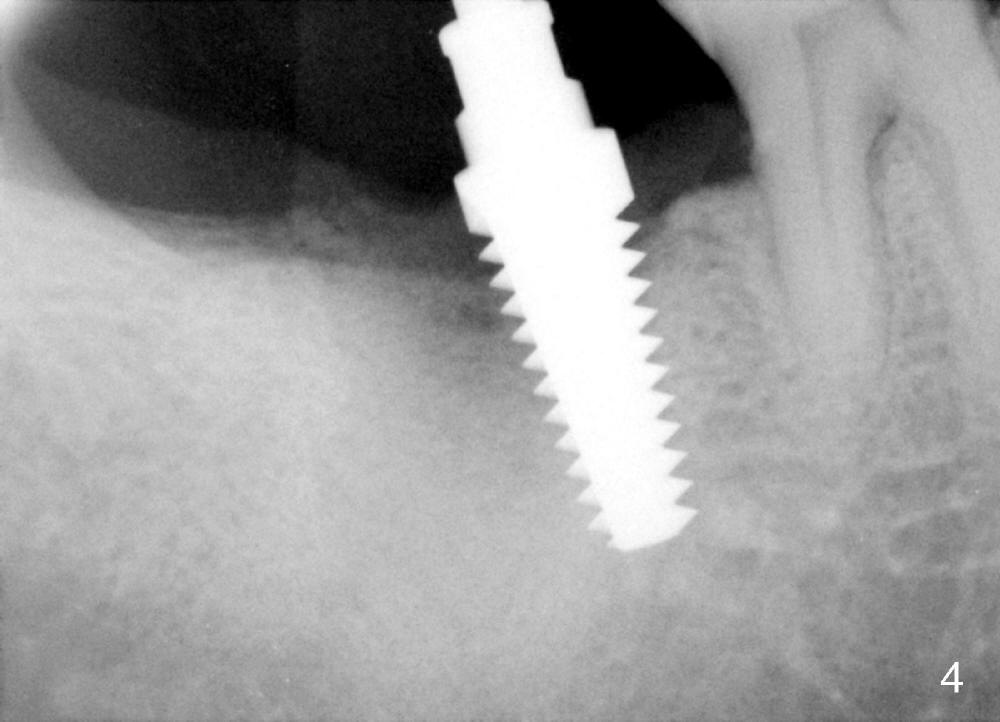
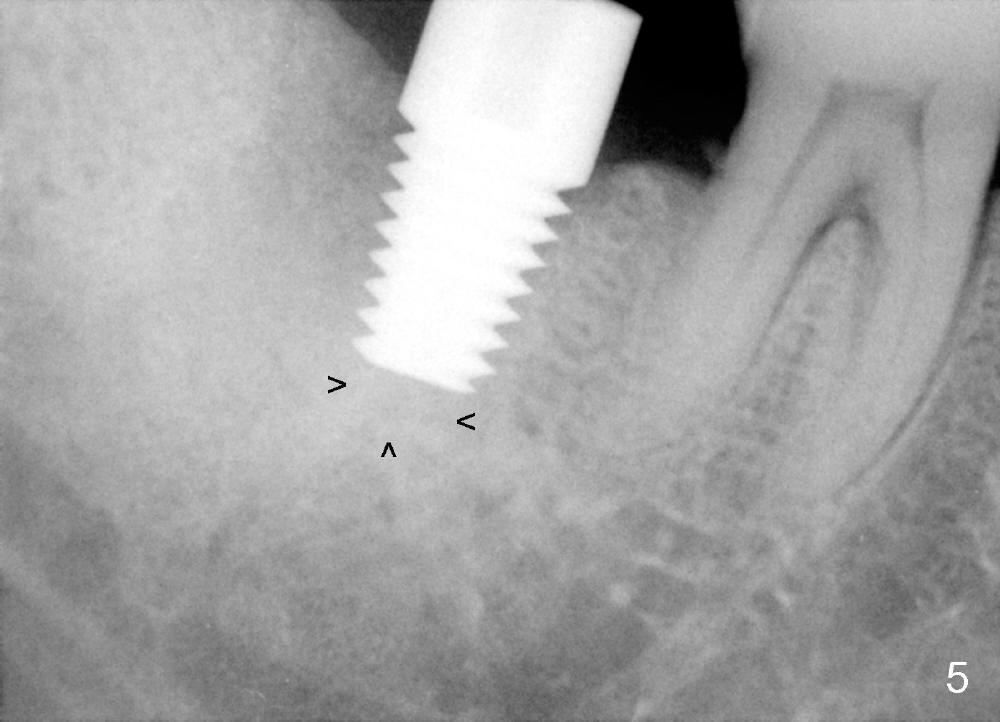
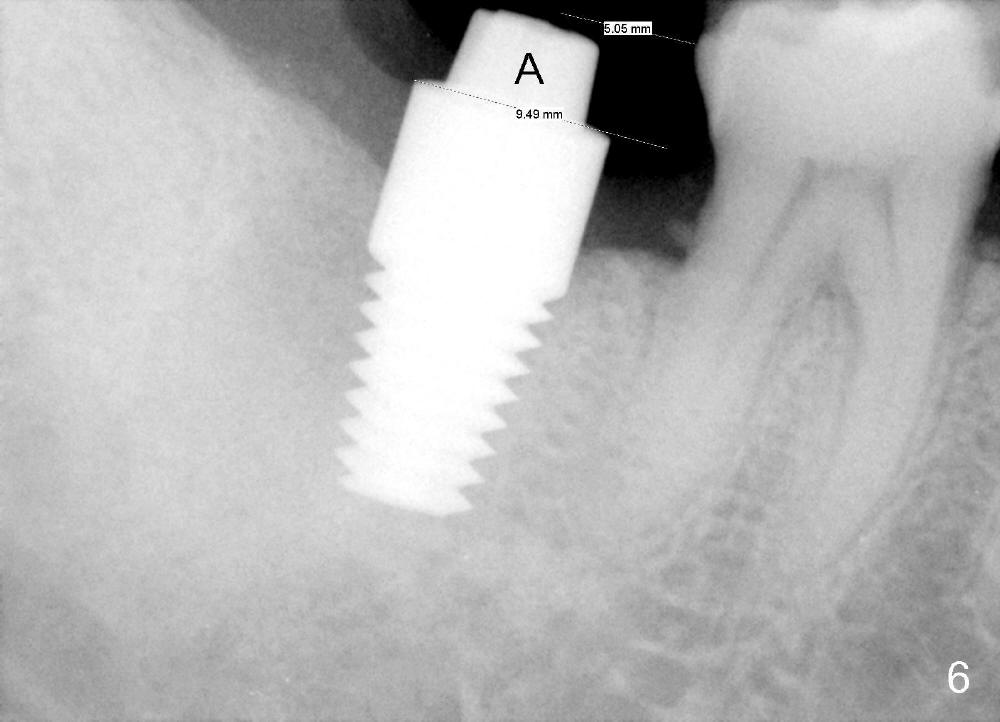
The patient returns for implant placement 2.5 months after socket preservation at the site of #31. The socket has healed (Fig.1). The plan is to place an implant along the long axis of the socket (Fig.2 red line) at the center of the healed socket (Fig.1 dot) with osteotomes. But it cannot be done with osteotomes starting at the mesial portion of the socket (Fig.1 *). A 2 mm pilot drill has to be used (Fig.3); the latter happens to have penetrated the mesial slope of the socket (pink dashed line). The advantage is to obtain higher primary stability in the mature bone than that in the middle of the socket. Therefore the length of the osteotomy can be shorter (14 mm instead of 17 mm). After sequential osteotomy, a 6x17 mm tap is inserted at the depth of 14 mm (Fig.4). Before a 7x14 mm implant is placed, autogenous bone is placed in the distal aspect of the socket. The implant is not placed as deep as expected. It is possible that the bone graft is inadvertently pushed to the apex of the osteotomy (Fig.5 arrowheads) when the implant is being placed. After removal of the graft from the apex of the osteotomy, the implant is seated normally (Fig.6). In fact the implant fails. Can you guess what is the main reason? Smoking?
Return to Lower Molar Immediate Implant,
Systemic Disease
Xin Wei, DDS, PhD, MS 1st edition 12/10/2014, last revision 03/11/2015