
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
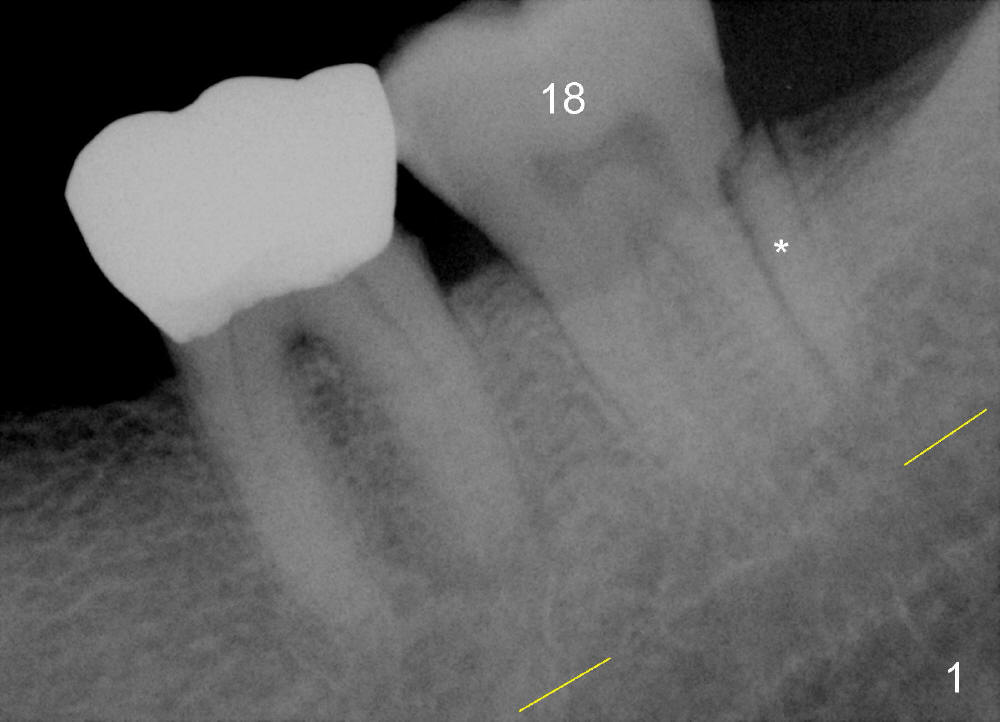
Immediate Implant Placed at Insidiously Infected Site
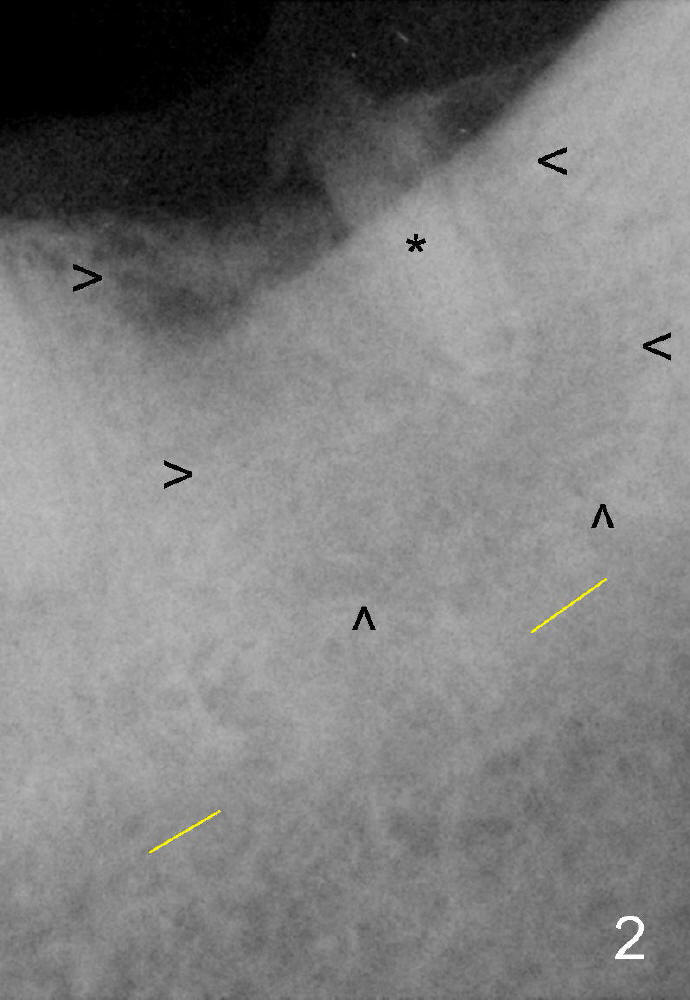
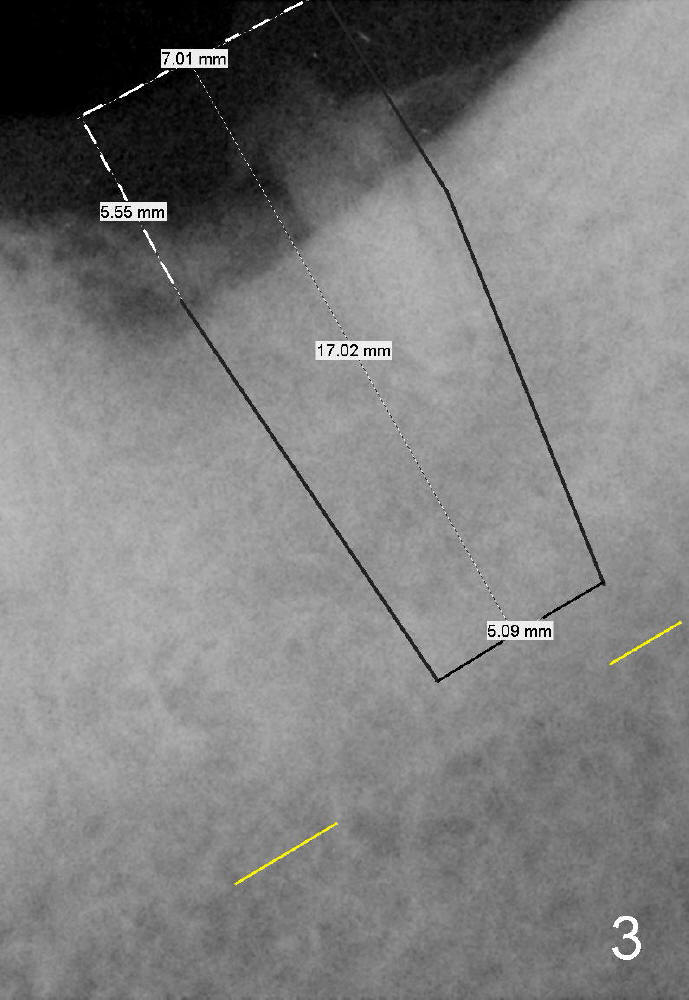
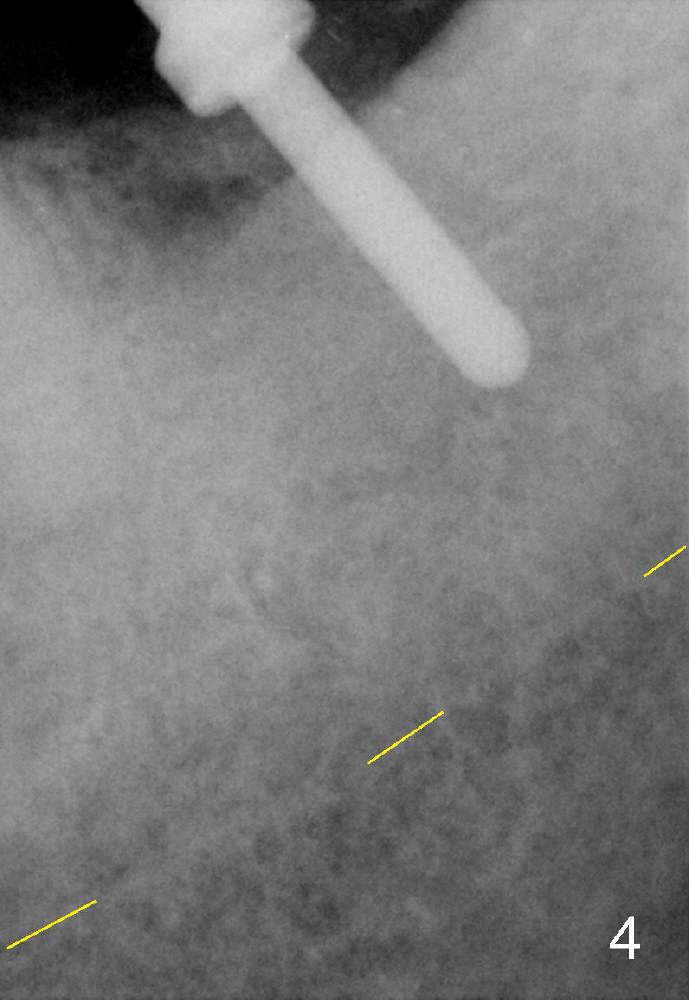
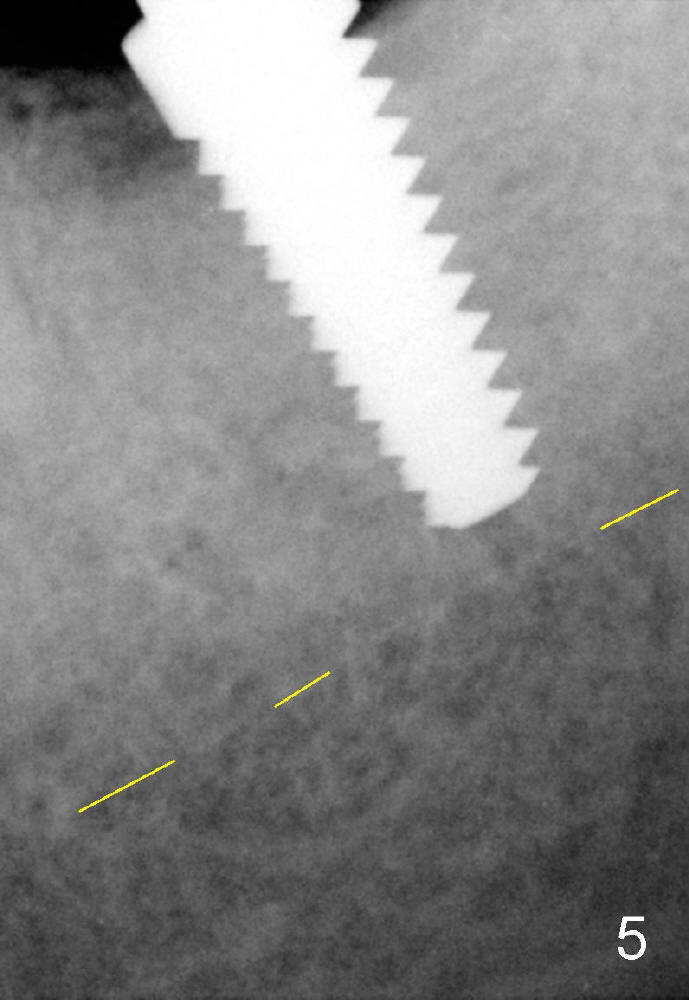
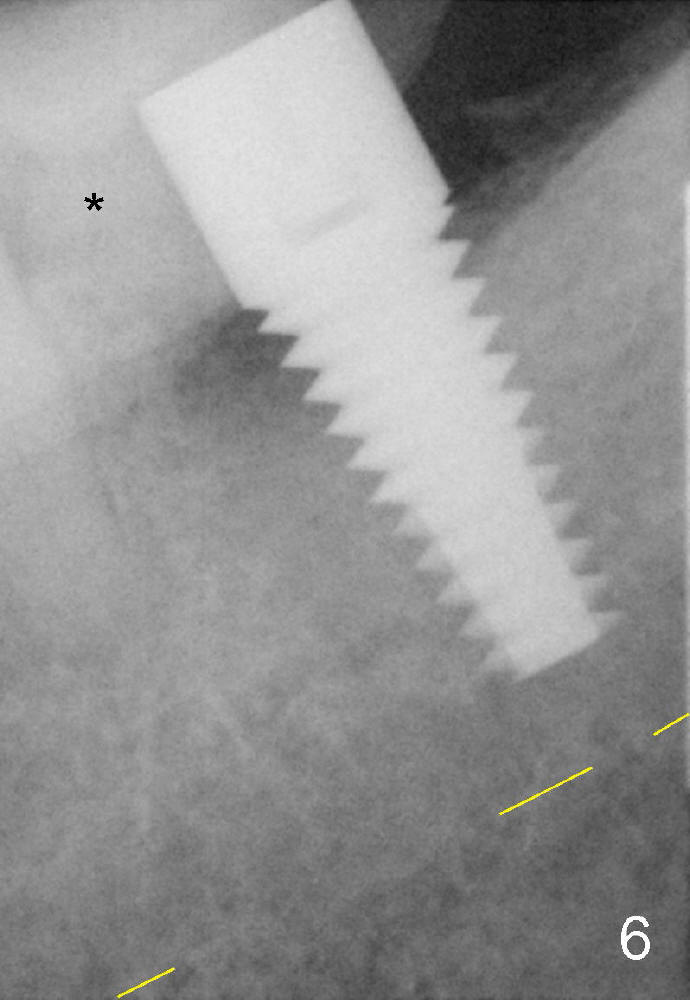
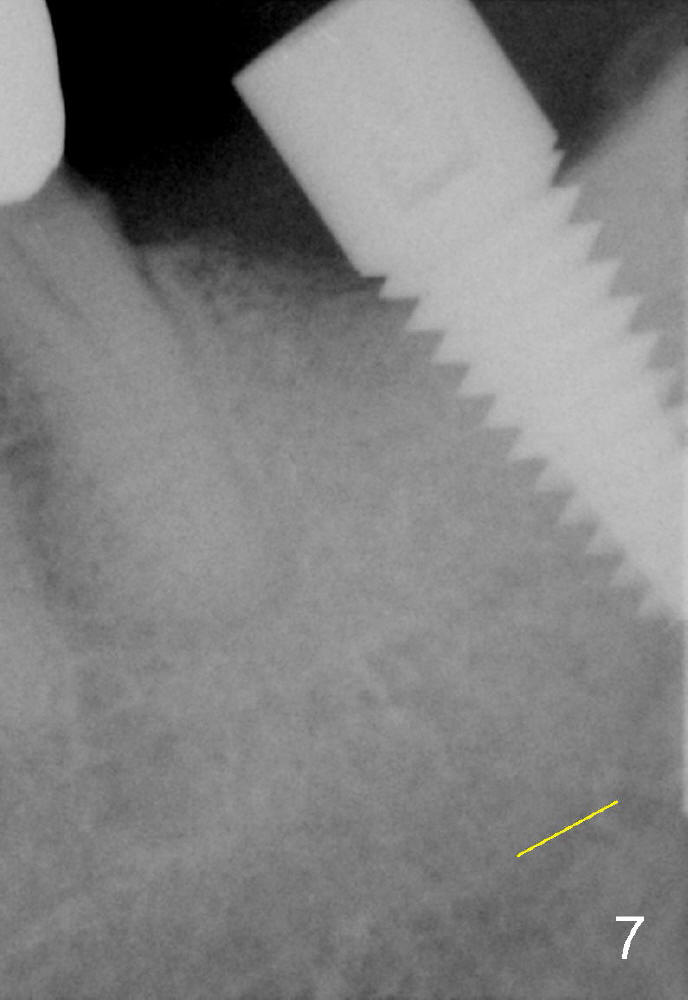
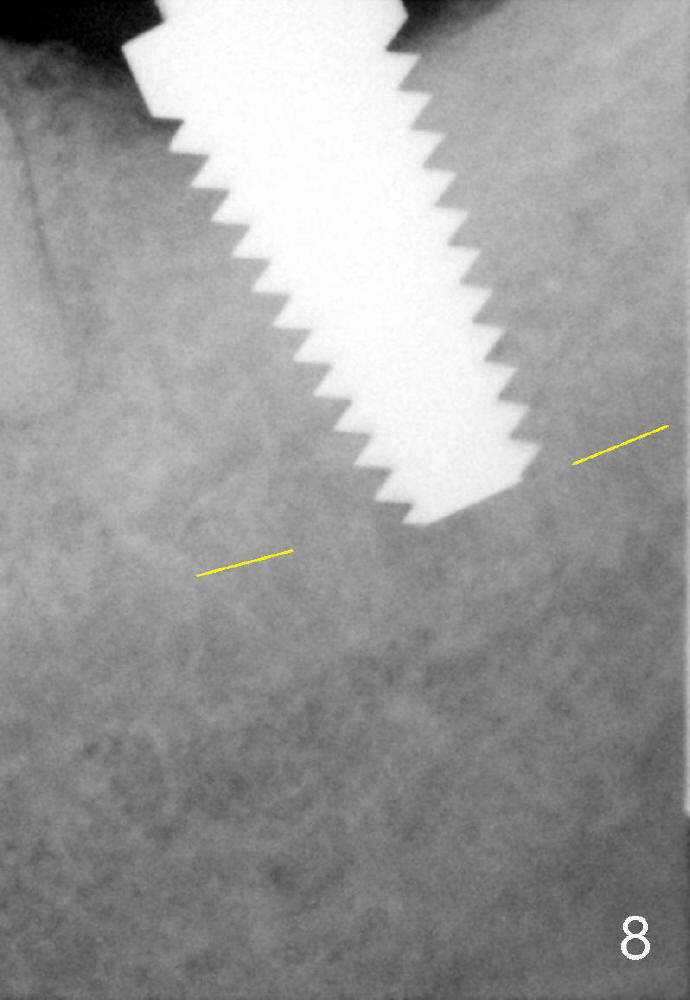
A 62-year-old man has lost several teeth with possible history of bruxism. The tooth 18 was found to have root fracture 4 years ago (Fig.1 *). Finally the tooth was extracted without complication. Eleven months later, he agrees to have implant placement; PA shows that the fractured root fragment was not removed with apparently low bone density (Fig.2)! A 7x17 mm tissue-level implant is planned (Fig.3). Probably due to the guilt not removing the residual root and closeness to the Inferior Alveolar Nerve (yellow dashed line), a 6x17 mm implant was placed with insertion torque 15 Ncm (Fig.4-6). The bone is soft probably due to chronic insidious infection. The wound did not appear to heal normally initially, but finally it did. Three months postop, the implant was found unstable (Fig.7).
The implant was removed; a 7x17 mm tap was inserted immediately with stability (Fig.8). Insertion torque of the 7x17 mm implant is 35 Ncm (Fig.9). Retrospectively a larger implant should have been placed! The reason not doing so is most likely related to concern over the nearby nerve. Fortunately, no paresthesia occurs following the 2 placements. There is a chance for 3rd placement if the last implant is found to loose again. The patient is returning next Monday, 2.5 months post 2nd placement. In fact, the implant is stable (Fig.10). A crown is cemented 4 months postop. Three months later, the patient returns for cleaning and reports that the implant helps his mastication (Fig.11 (BW)). He wants to have a 2nd implant (#3) soon. Because of low bone density and premature loading, the implant fails.
Return to Lower Molar Immediate Implant,
Implant
Failure,
Implant
Complications, Implant
Dislodgement
Xin Wei, DDS, PhD, MS 1st edition 12/25/2014, last revision 12/20/2015