
|
|
|
|
|
|
|
|
Posterior Stop
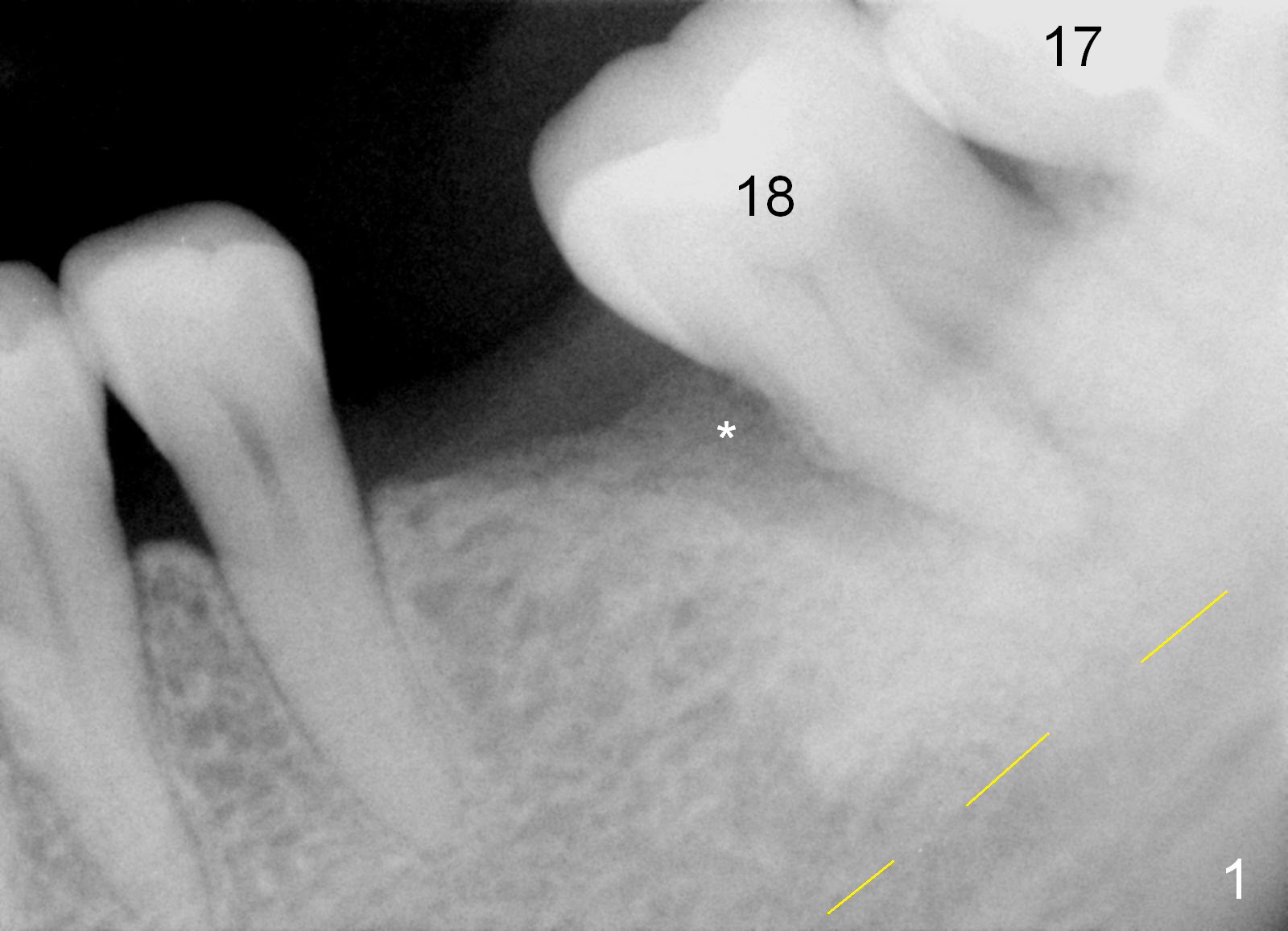
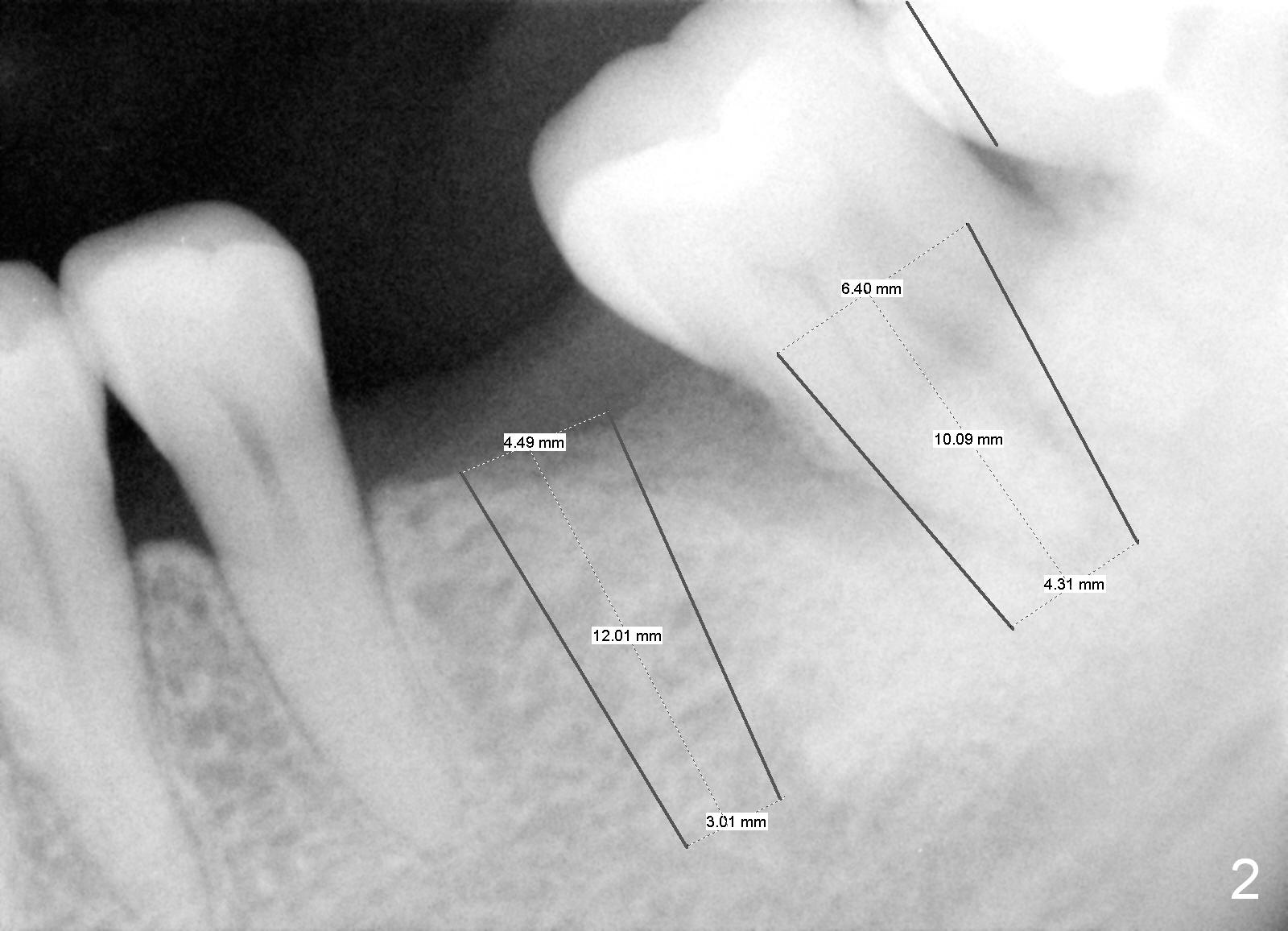
A 53-year-old lady (HL) is most likely a bruxer. The tooth #9 is labially shifted and mobile presumably under undue occlusion. The temporary abutment gets loose twice and the cemented abutment once. After retorque and heavy occlusal reduction, the incisal edge of the Zirconia crown chips (take photos). The teeth #17 and 18 have tilted mesially in association with #19 missing (Fig.1). The tooth #18 has severe bone loss, especially mesially (*). Immediately after #18 extraction (socket treated with 2% Xylocaine/1:50,000 Epinephrine), implants are to be placed at #18 and 19 (Fig.2). To accommodate the large implant at #18, the mesial surface of the tooth #17 will be reduced (Fig.2 black vertical line). Final restoration will be done together: #9, 18 and 19 with light occlusal contact at #9 and heavy one at #18 and 19. Night guard will be fabricated.
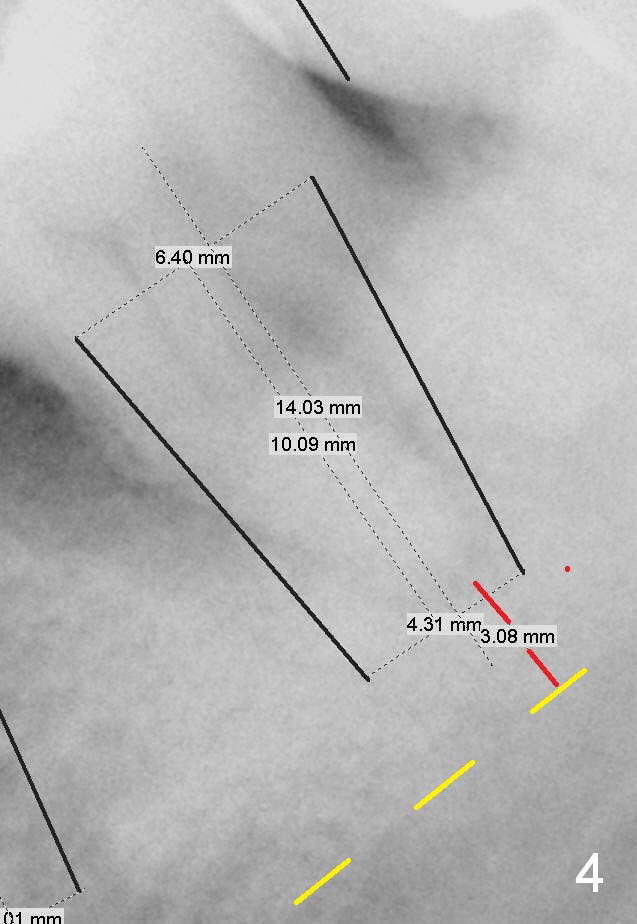
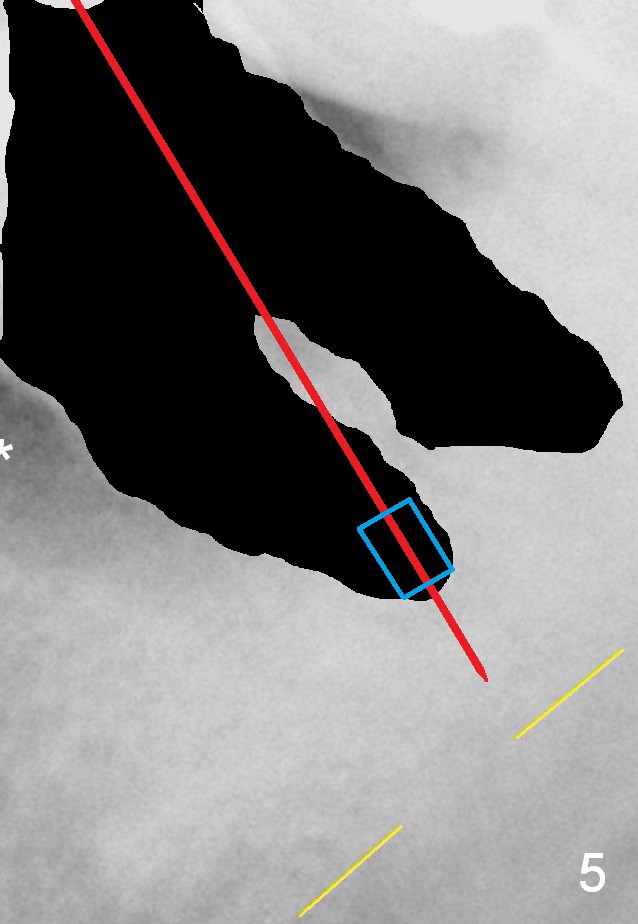
Panoramic X-ray shows that the apex of the tooth #18 is close to the Inferior Alveolar Canal (Fig.3), approximately 3 mm (Fig.4 red line). A 2 mm pilot drill (Fig.5 red line) with 2 mm stopper (blue box, from Sinus Master Kit) will be used to initiate osteotomy in the mesial after extraction (black area), followed by 2.8 and 3.6 mm round burs. This can avoid injury to the Inferior Alveolar Nerve. Take several intraop PAs if necessary.
To prevent periimplantitis at #18, the implant should be placed as lingual (assume more bone loss buccally) and deep (6 or 8 mm instead of 10 mm long (Fig.2,4)) as possible. Any portion of exposed implant threads should be covered by bone graft and collagen membrane. If socket visibility is poor, extend #19 incision distally.
If bone condition at #18 is poor, finish socket preservation and extend an immediate provisional from #19 to cover #18 socket opening.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/13/2016, last revision 02/18/2016