|
|
|
|
|
|
Change Position of 2 Molars Due to Shifting
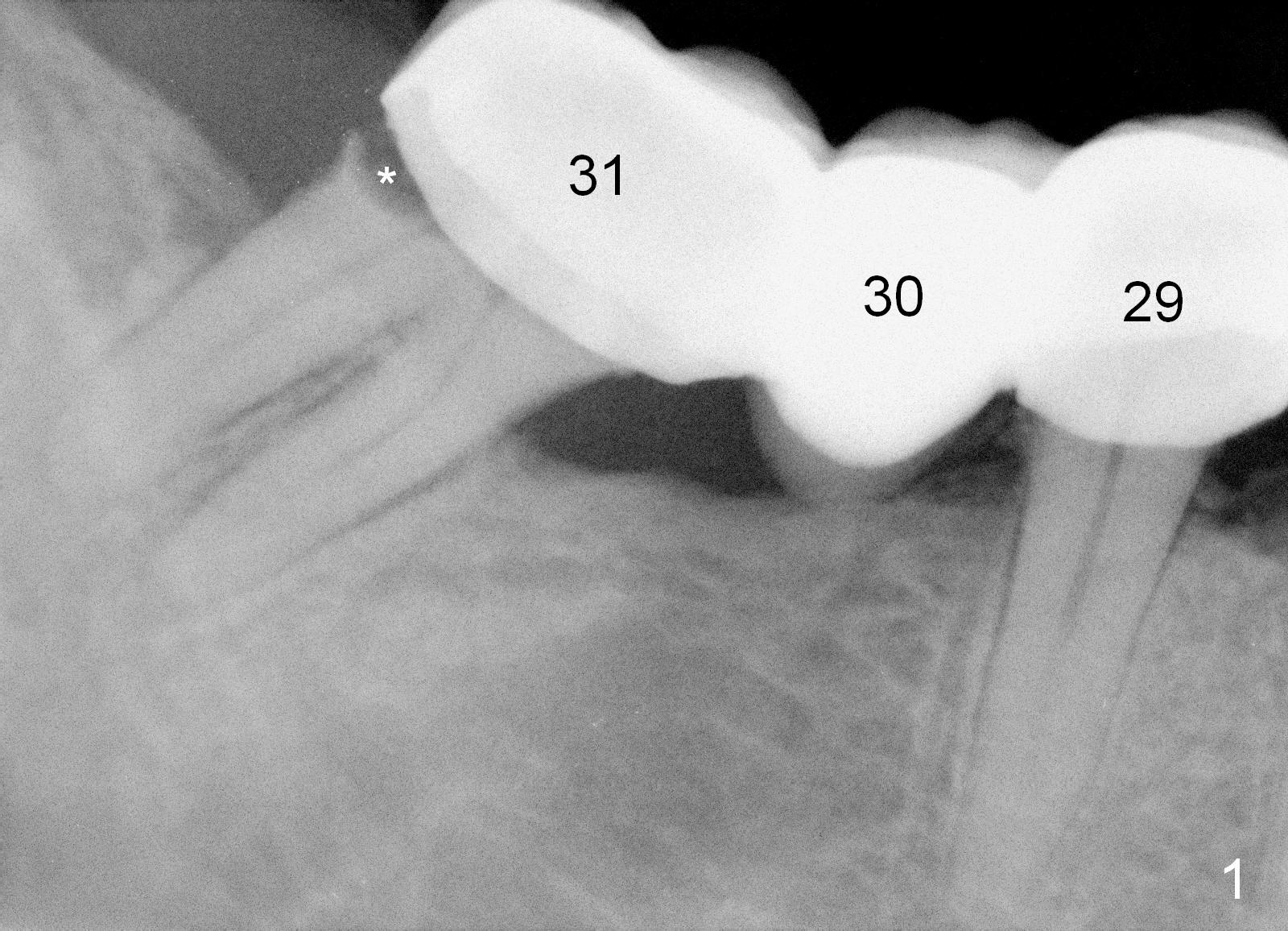
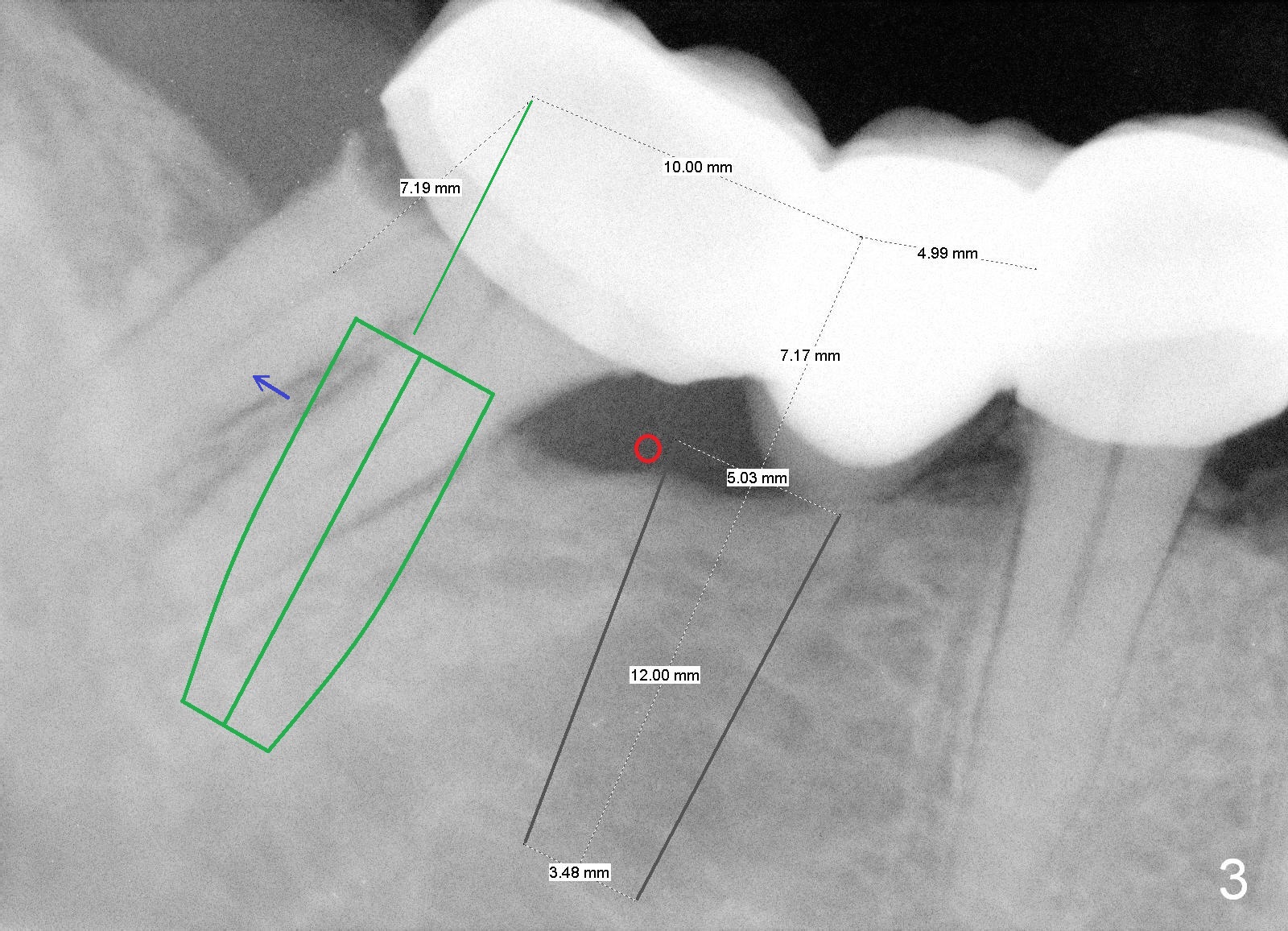
A 43-year-old man has a failed bridge (Fig.1: #29-31). The mesiodistal width of the pontic (#30) is pathologically narrow. When an implant is placed at the site, the osteotomy position should be moved distally, 5 mm from the distal surface of the tooth #29 (Fig.3), while the center of the osteotomy at the site of #31 should be 10 mm from the center of the osteotomy at the 1st molar.
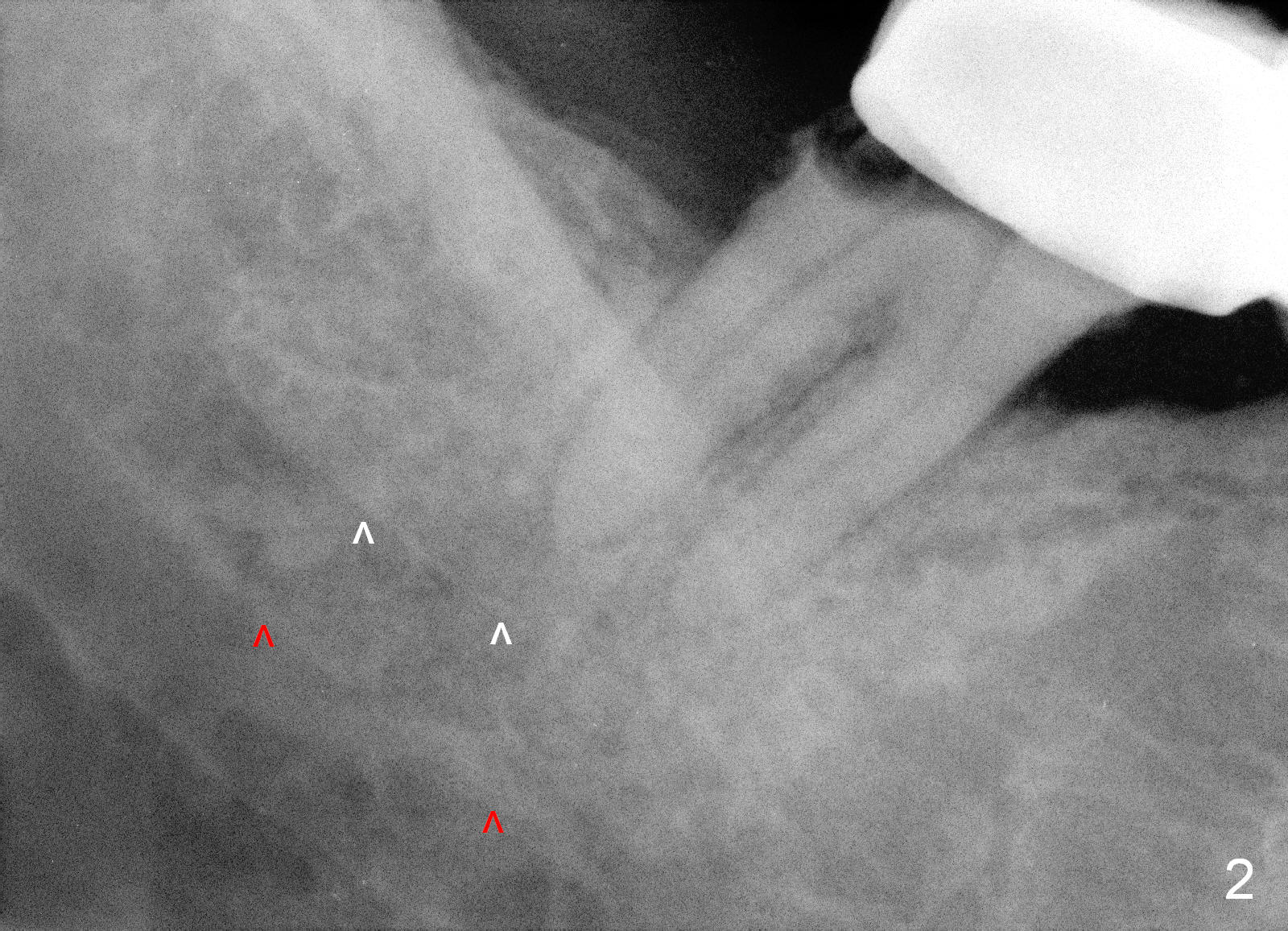
As to the depth of the osteotomy at the site of #31, it is difficult to differentiate the upper border of the Inferior Alveolar Canal (white vs. red arrowheads in Fig.2).
Therefore, it is safer to place an implant coronal to the white arrowheads, i.e., 2 mm apical to the apex of the mesial socket (compare Fig.2,3).
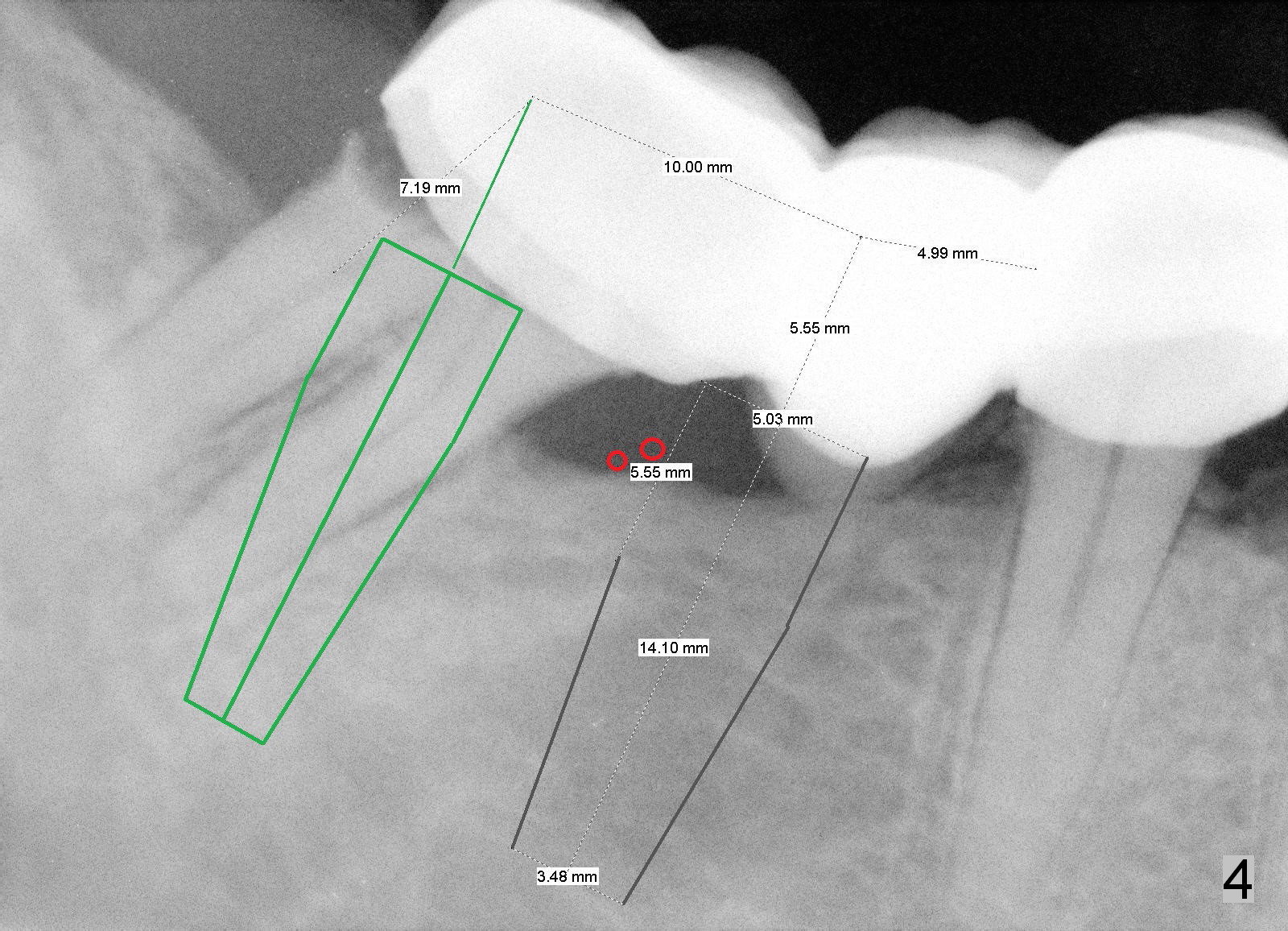
The length of tissue-level implants should be confined to 14 mm (Fig.4).
To ensure the position and trajectory of these 2 implants, impression will be taken prior to surgery for wax up and surgical stent fabrication.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/11/2015, last revision 01/19/2018