




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
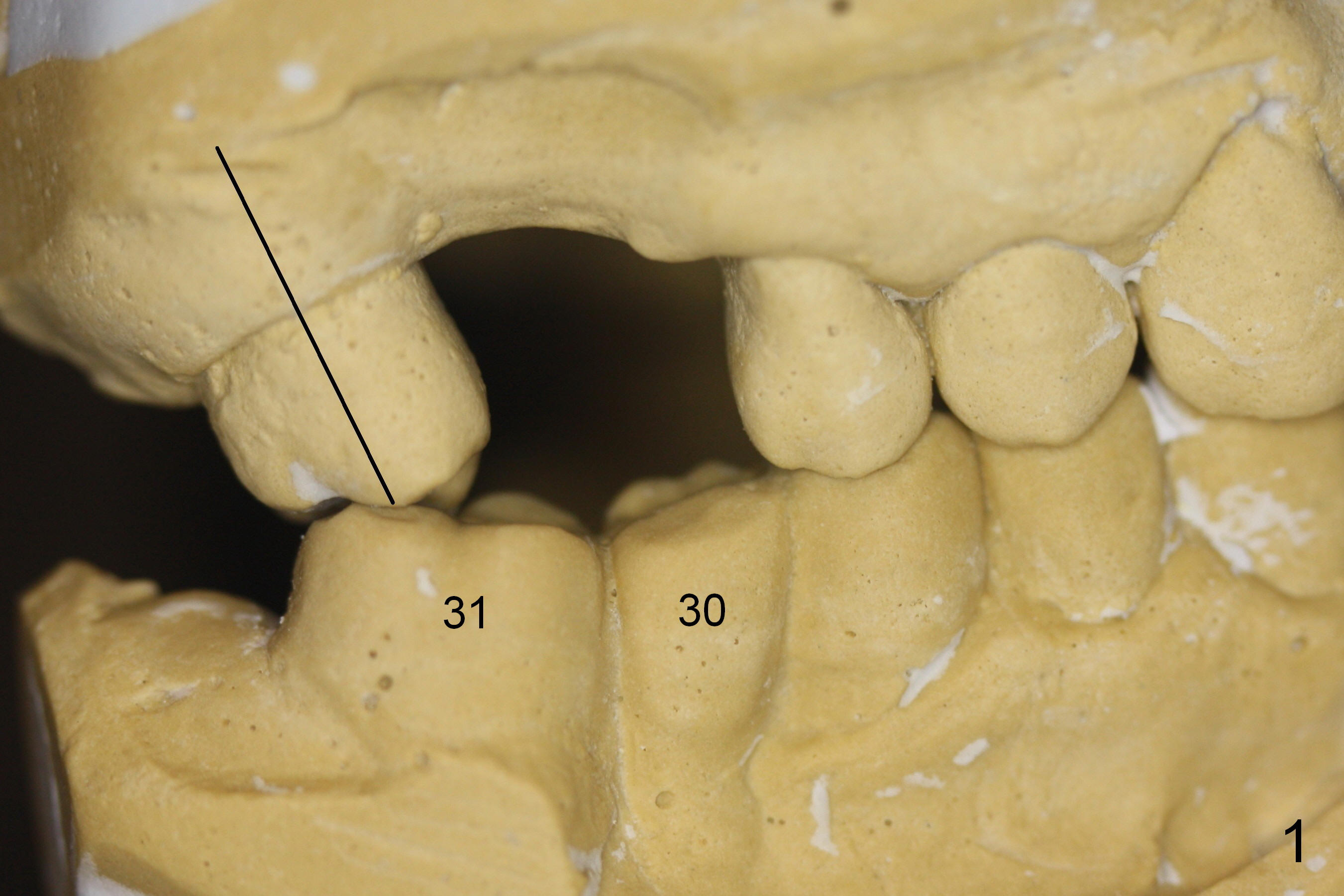
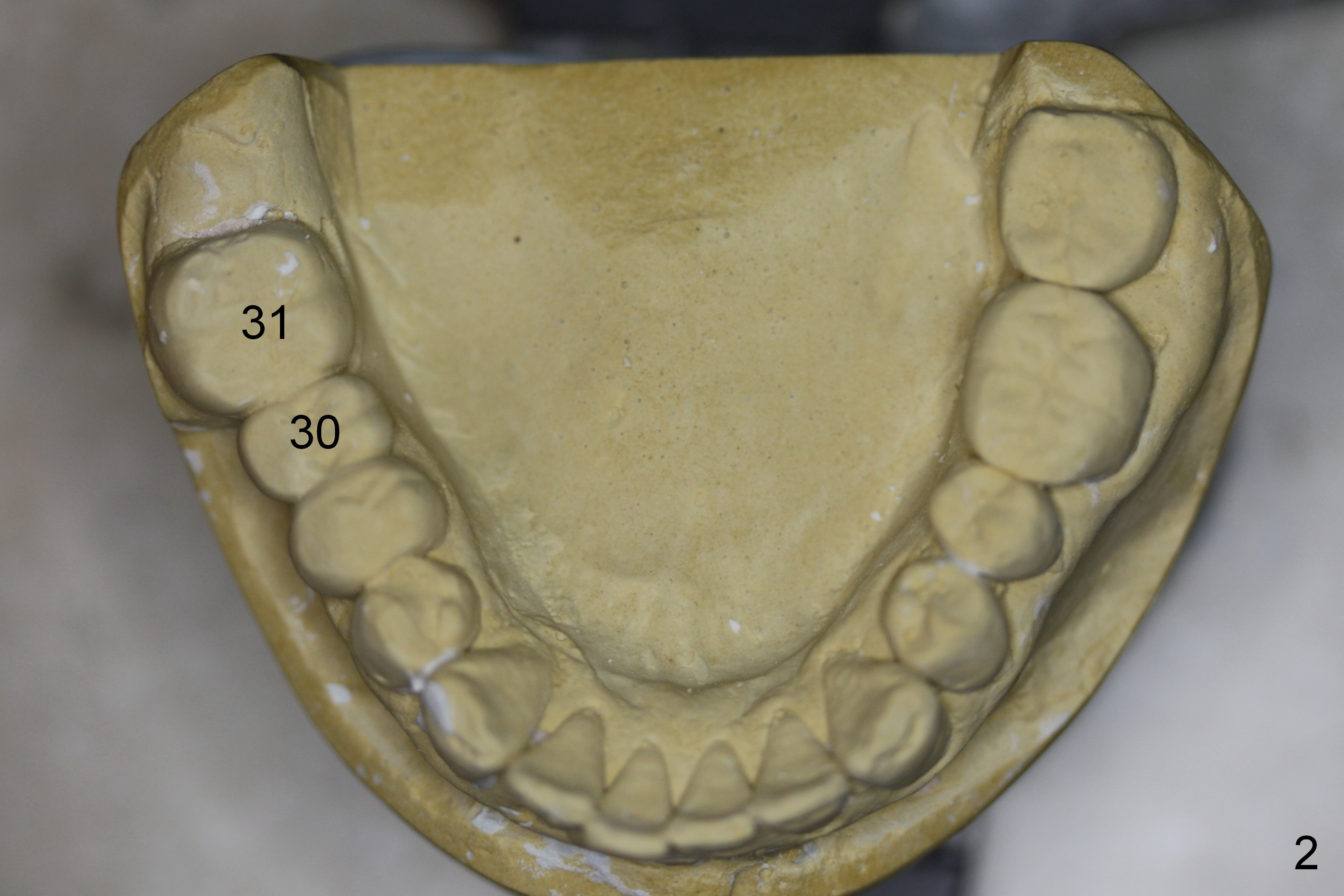
Wax Up and Surgical Stent
Prior to surgery, models are mounted to show tilting of #2 into #3 edentulous space (Fig.1). Wax up extends the lower right posterior sextant (Fig.2,3). A surgical stent is fabricated for determination of osteotomy at the sites of #30 and 31 (Fig.7-10).
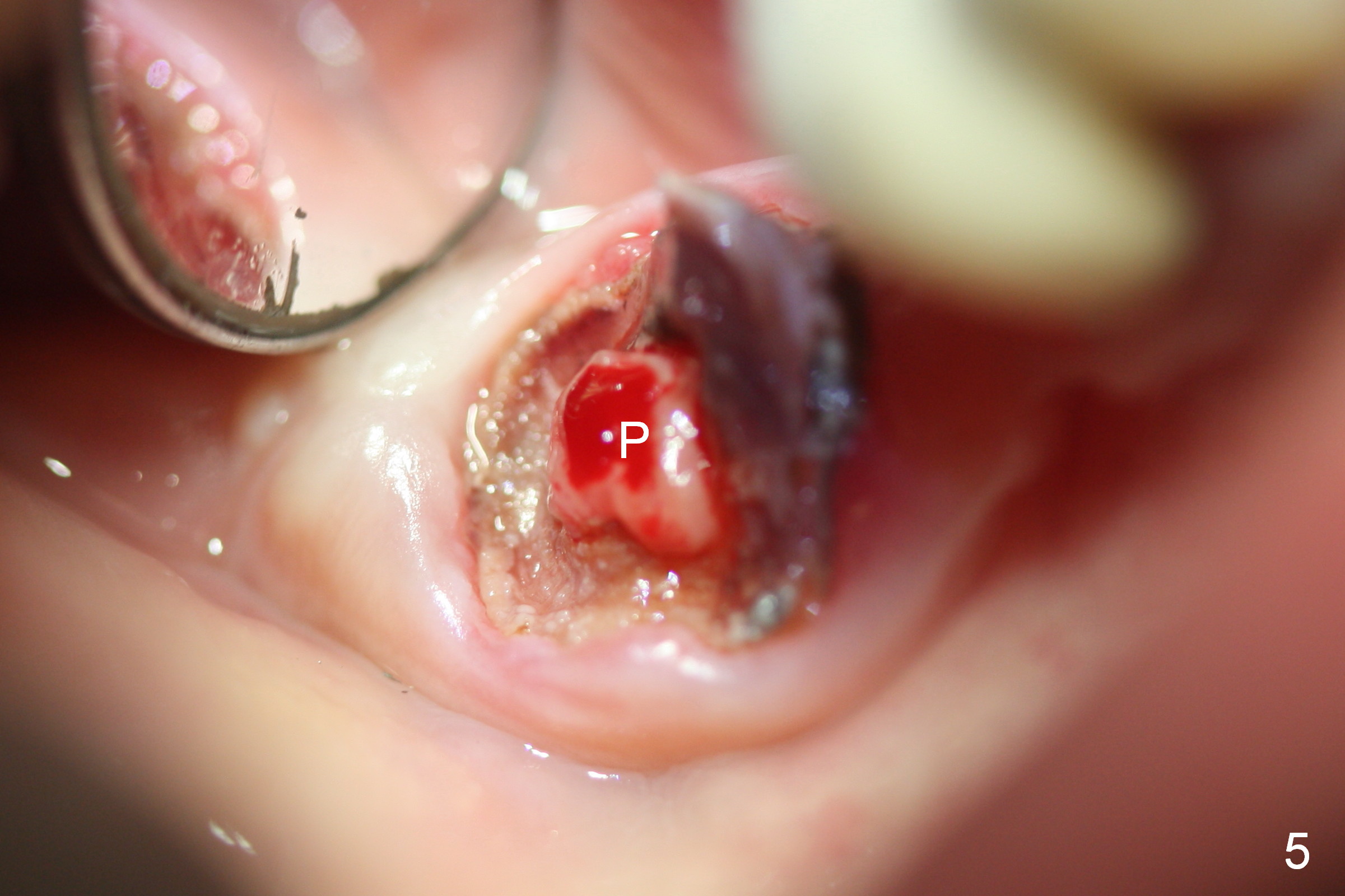
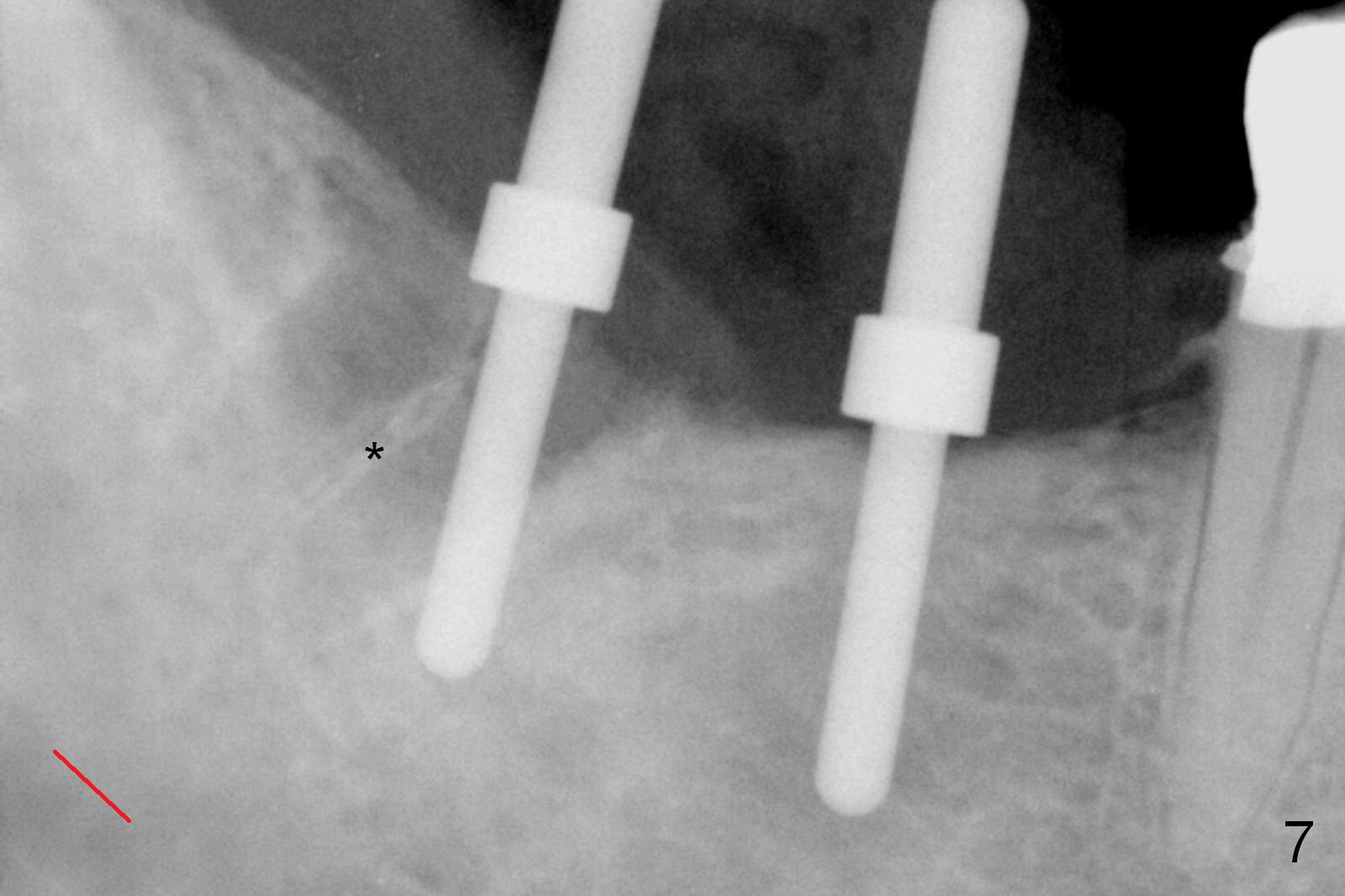
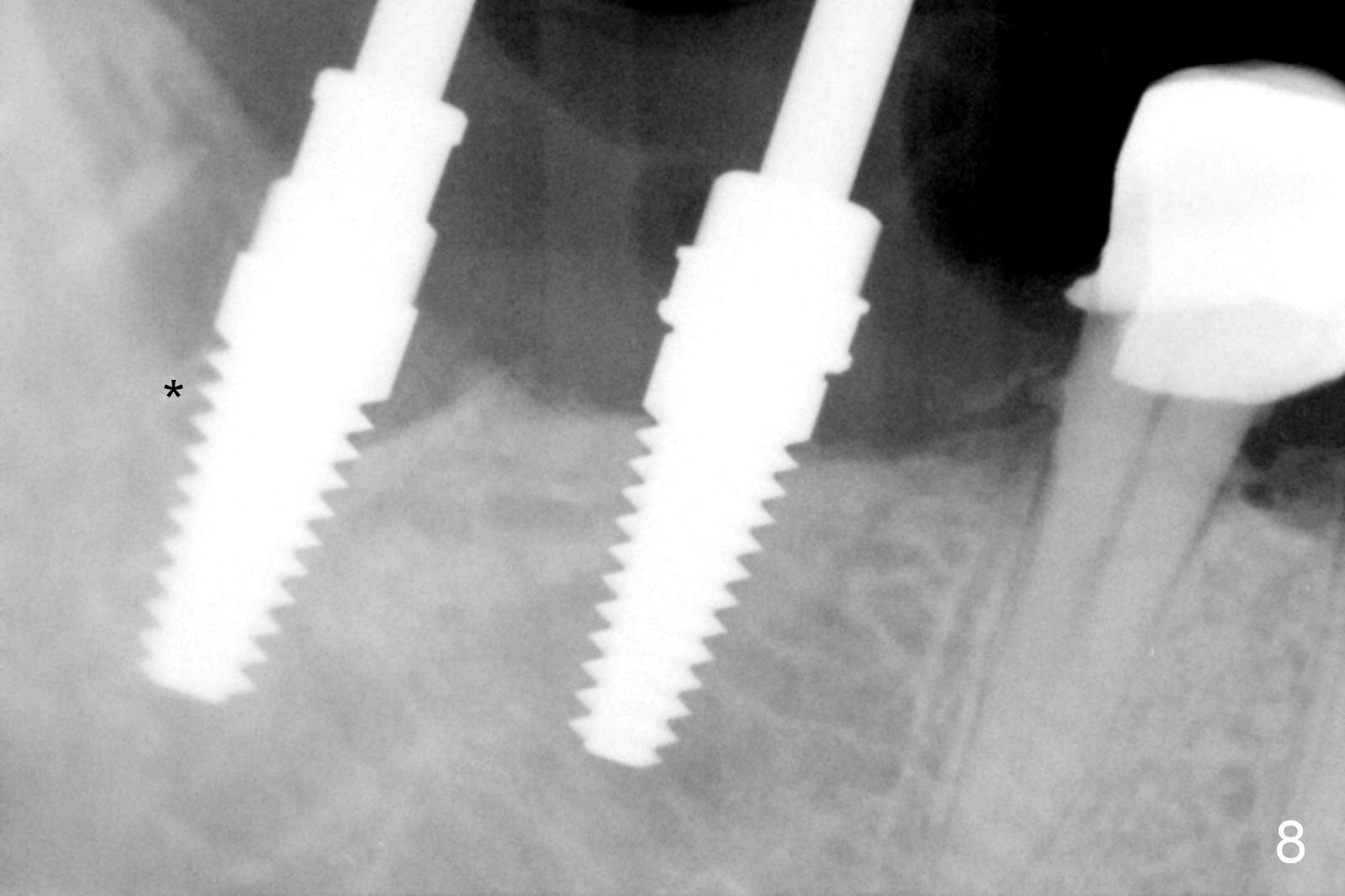
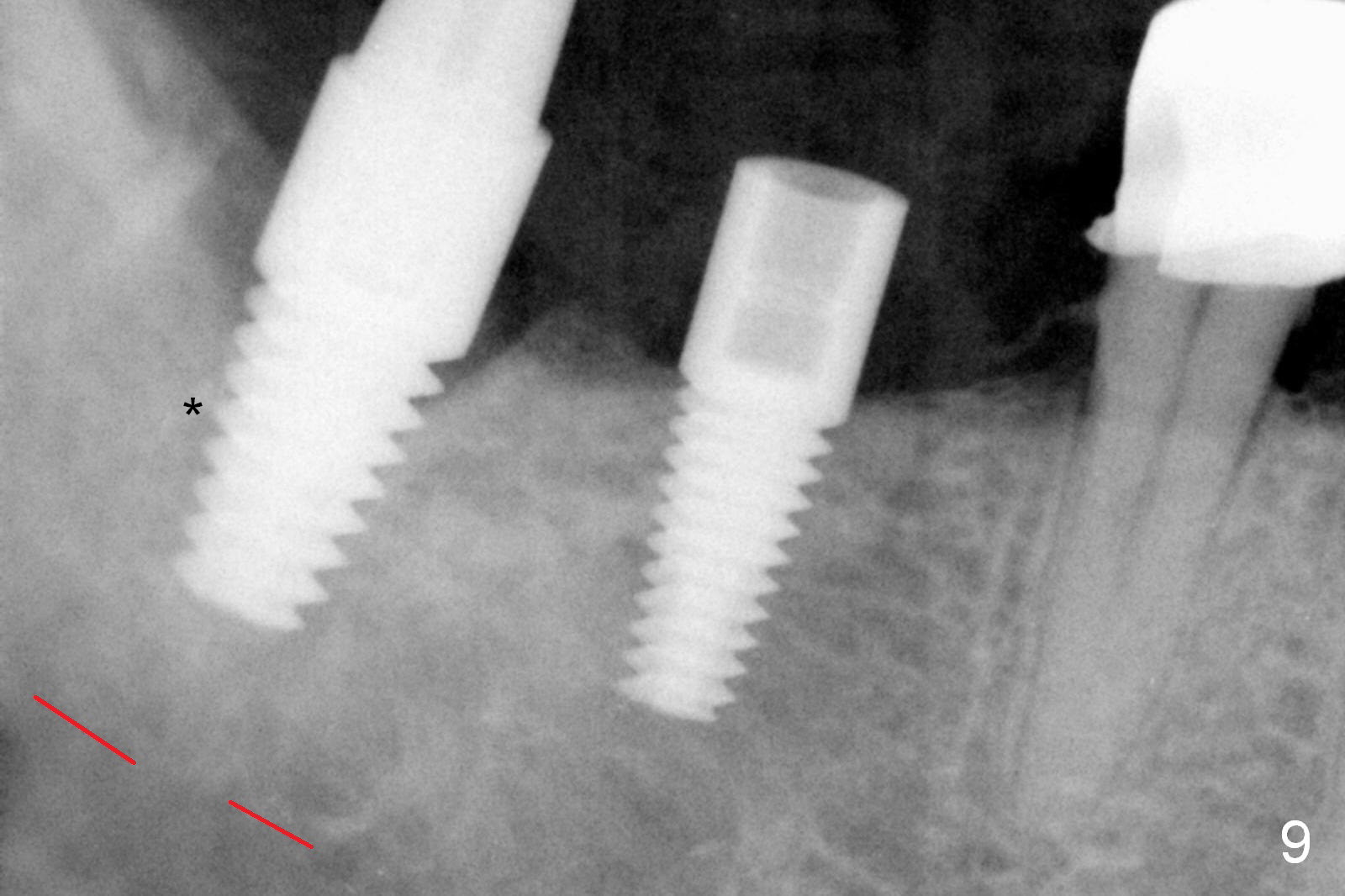
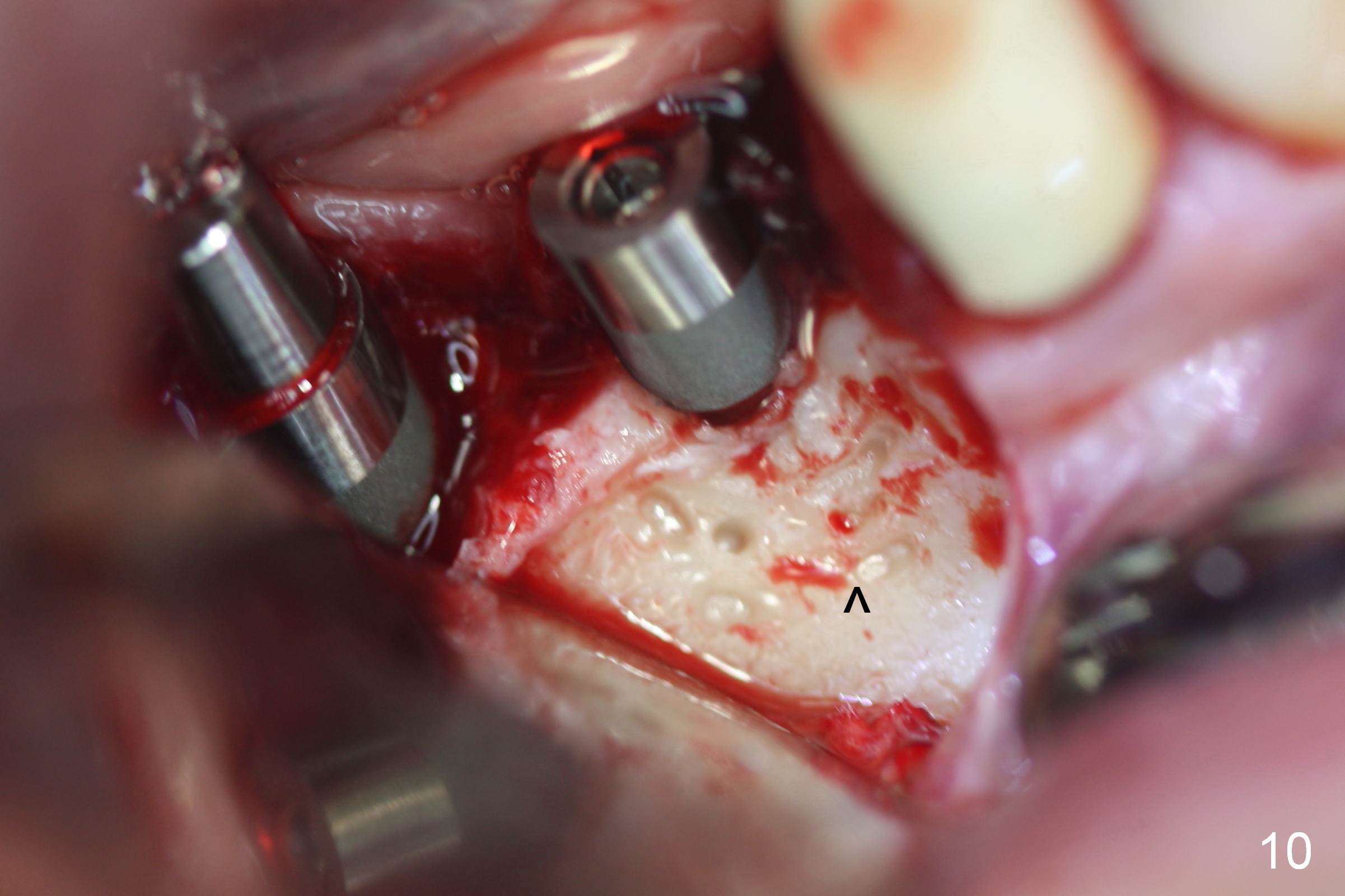
Sectioning the over-contoured bridge (Fig.4) reveals severe caries of the tooth #31 with pulpal polyp (Fig.5 P). There is a thin septum in the socket (Fig.6 *). The osteotomy at the site of #31 is established in the mesial slope of the mesial socket, while the coronal end of the osteotomy deviates distally (Fig.7: correcting tilting). The position and parallelism are being maintained at the later stage of the osteotomy thanks to repeated checking with the surgical stent (Fig.8,9). The buccal plate at the site of #30, thin after implant placement, is decorticated prior to bone graft and membrane (Fig.10 ^).
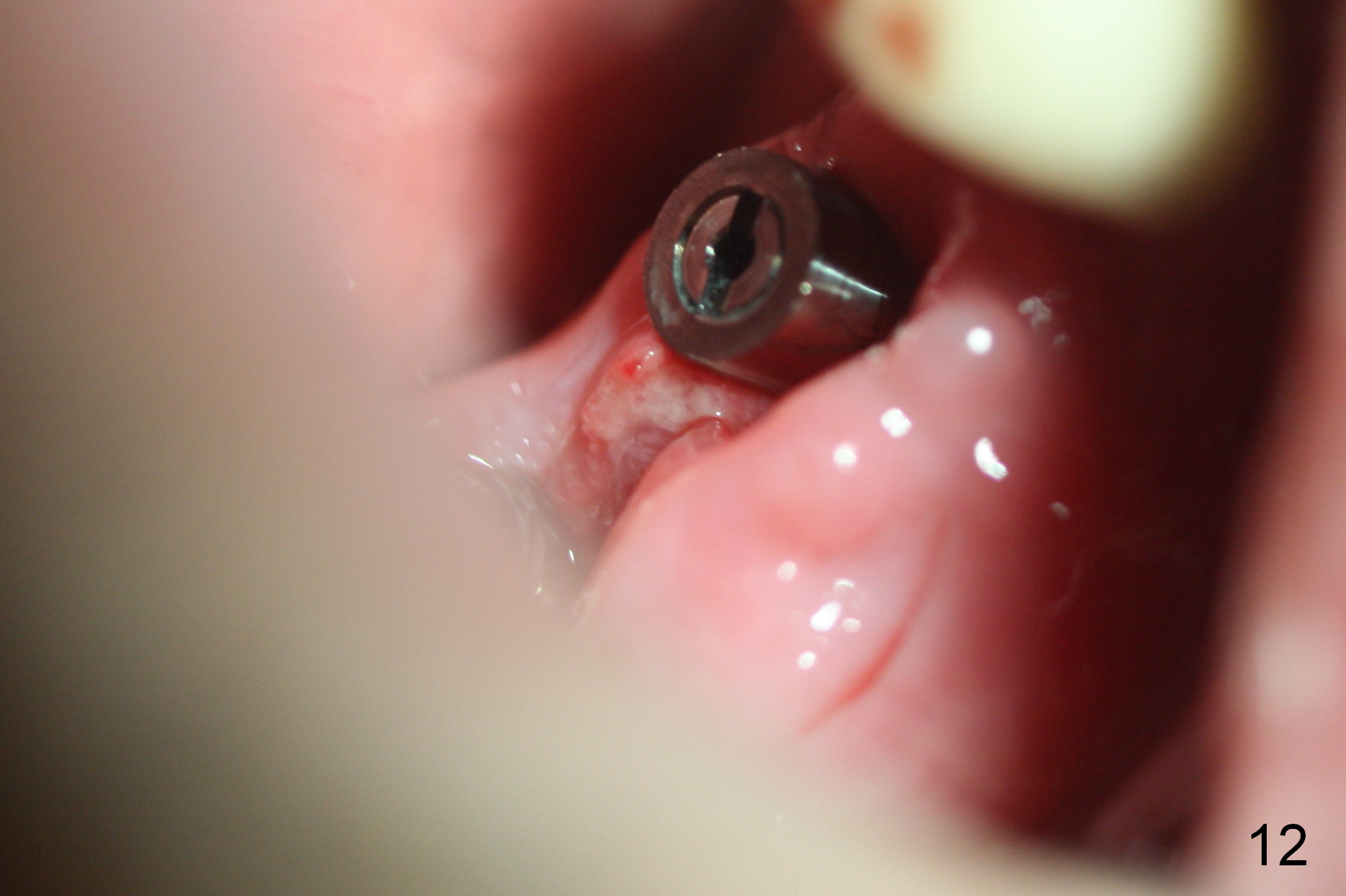
The patient returns for follow up 3 weeks postop (Fig.11). The splinted provisional has been removed by the patient because of discomfort. The wound heals normally around the implant at the site of #31, although there is swelling buccal to the implant at the site of #30(Fig.11 *). For better oral hygiene maintenance and avoidance of occlusal interference, the abutment at #30 is changed to a healing screw, whereas the abutment at #31 is changed to a short one. The latter is due to the fact that there is thicker gingiva at the site of #31 or the implant is placed a little too deep. In fact, the assumption is not correct. The swelling is due to retention of a piece of gauze. Fig.12,13 show after removal of the gauze, 6 weeks postop.
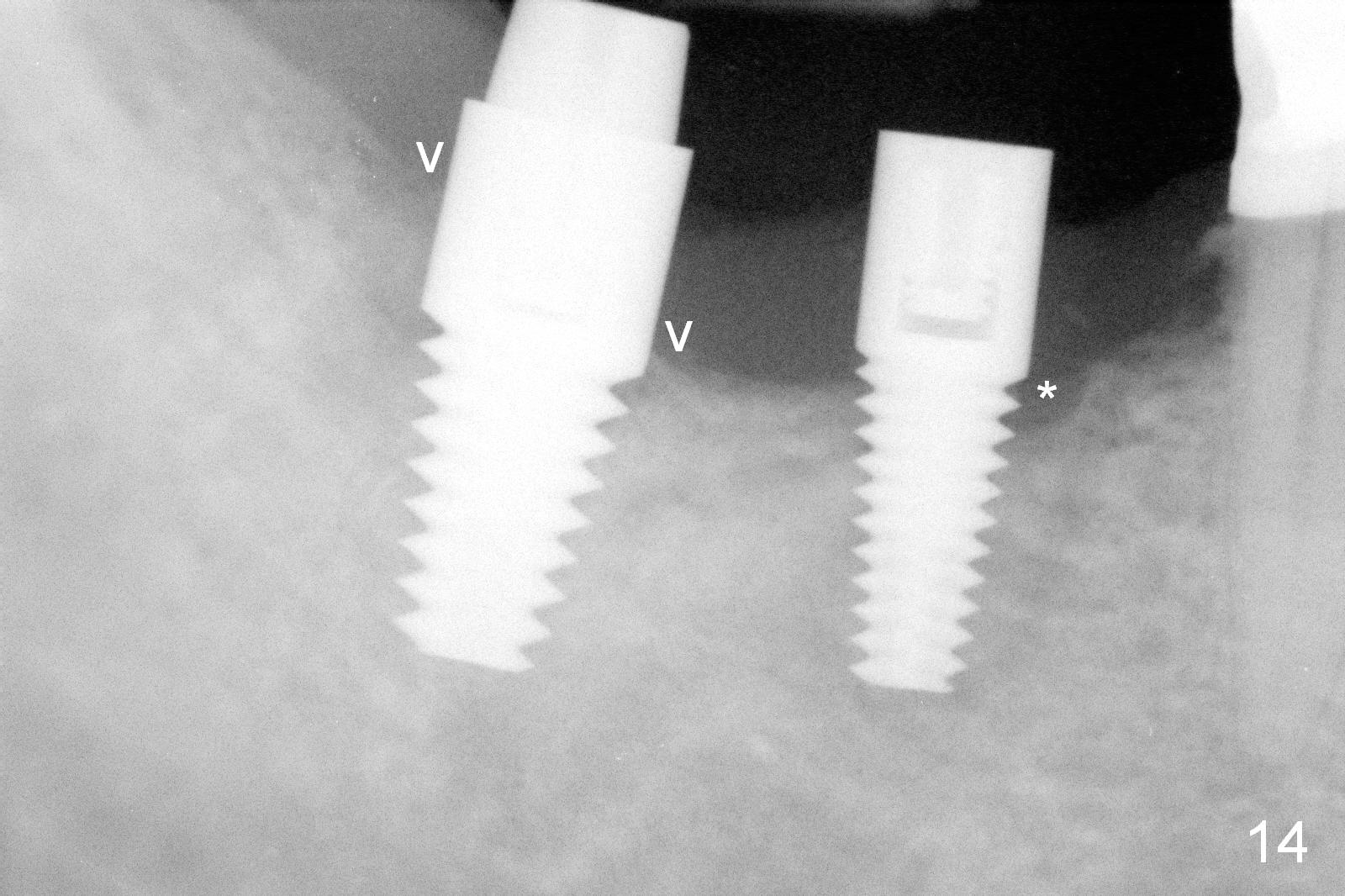
Three months postop, the mesial and distal gaps appear to have closed around the implant at the site of #31 (Fig.14 arrowheads, as compared to Fig.9), while there is bone resoprtion mesial to the implant at #30 (*). This suggests that lack of bone width is associated with bone loss. In contrast, there is ample bone around the immediate implant when it is placed, which is related to bone deposit (with bone graft).
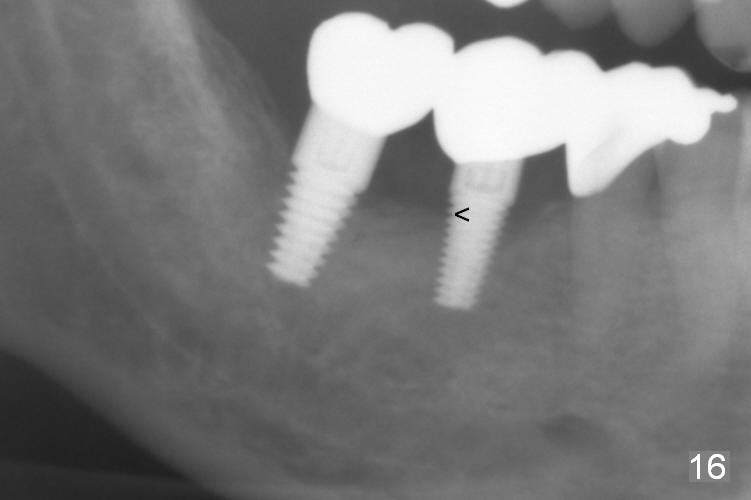
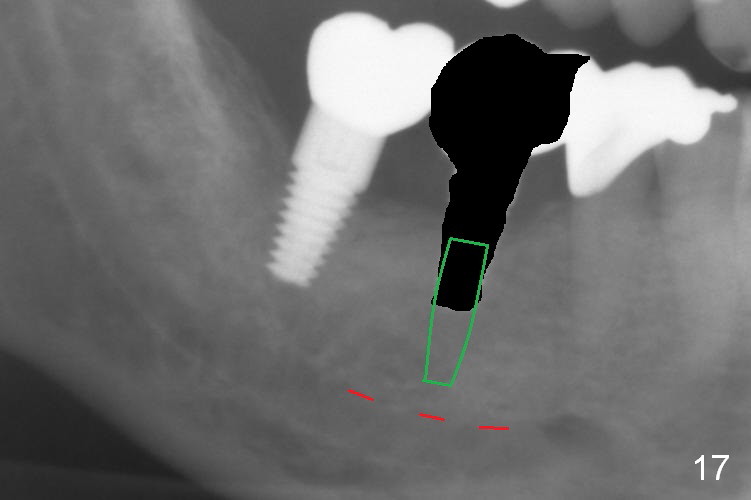
A few of the coronal threads at #30 appear not to be covered by the bone 6 months post cementation (15 months postop, Fig.16). If peri-implantitis develops, either remove the exposed threads or place a narrower implant deeper (Fig.17).
Return to Lower Molar Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 05/14/2015, last revision 08/10/2016