




|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
||||
No Drill No Paresthesia
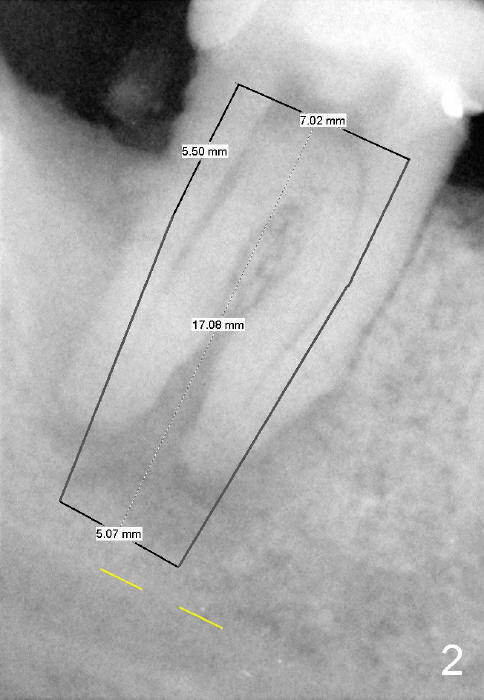
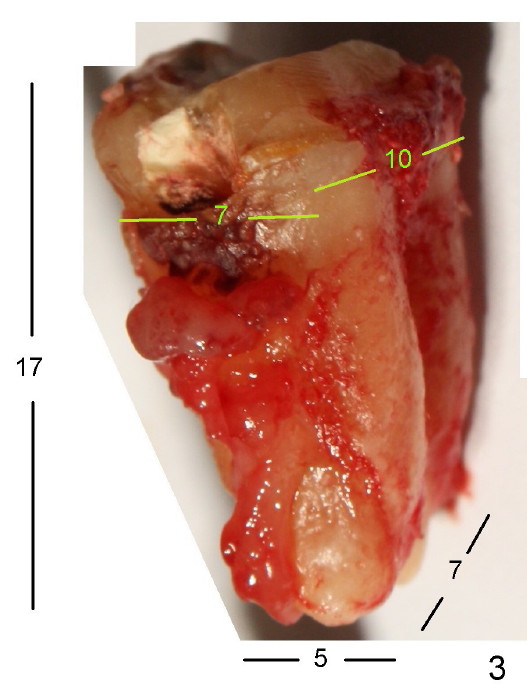
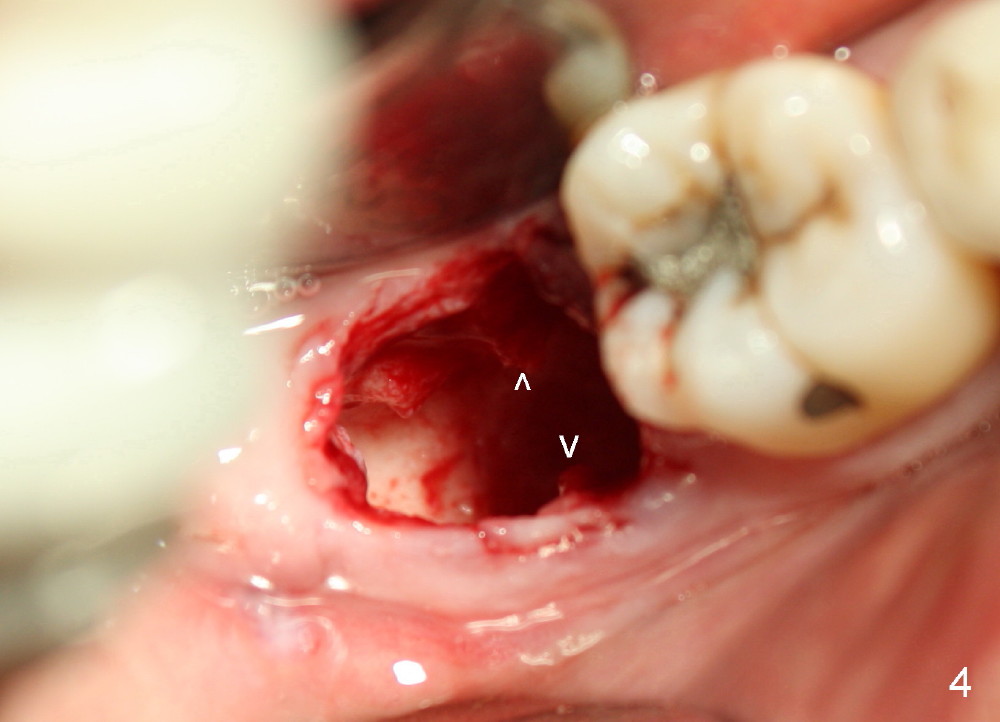
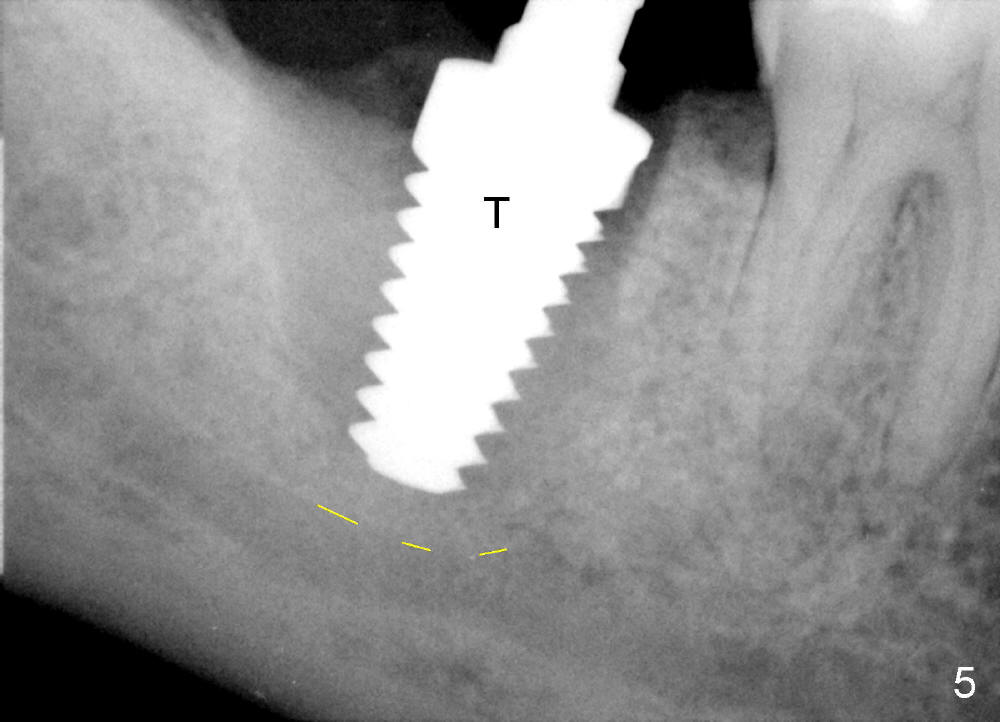
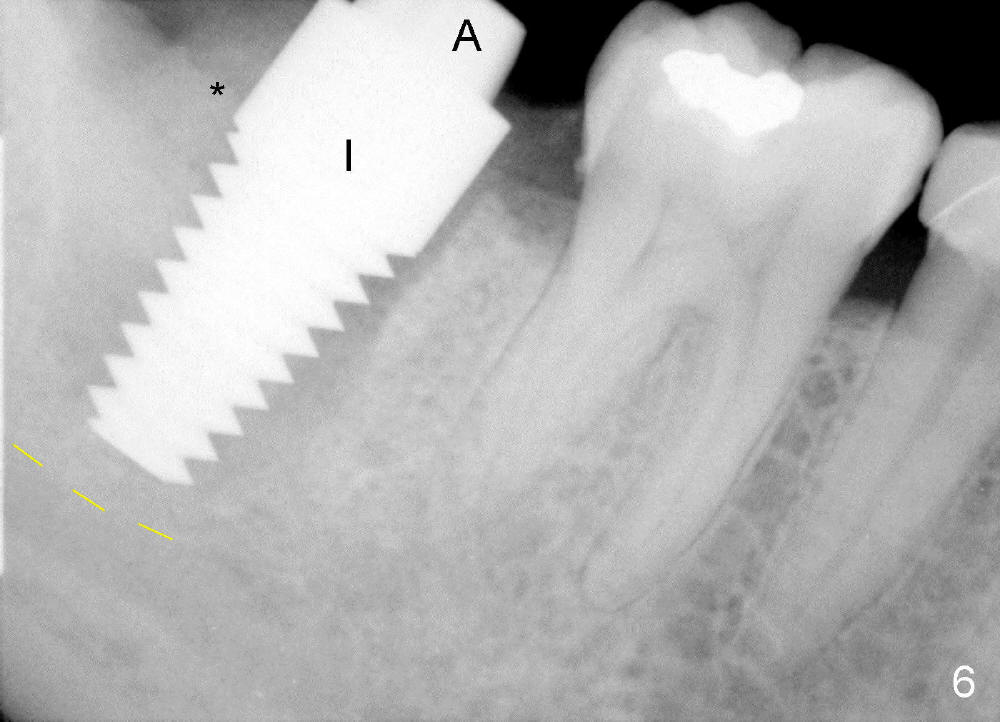
The tooth #31 of a 38-year-old lady has endo perio disease (Fig.1). Due to the large periapical lesion, there will be no solid (new) bone available for primary stability of an immediate implant (Fig.2: 7x17 mm). Yellow dashed line represents the upper border of the Inferior Alveolar Canal (IAC). Infiltration anesthesia is administered first. The mesiodistal widths of the root of the extracted tooth are 10 and 7 mm at the coronal and apical ends, respectively; the buccolingual ones 7 and 5 mm; the length 17 mm (Fig.3). The socket appears much larger than the root (Fig.4). To prevent paresthesia, no drills are used. Instead, a series of tap drills (6,7,8x17 mm) are sequentially inserted into the socket. The largest tap (Fig.5 T; 8x17 mm) binds to the socket securely with separation from IAC. Block anesthesia has to be administered before removal of the tap. A tapered implant (8x17 mm) is placed with insertion torque greater than 60 Ncm (Fig.6 I); allograft mixed with Osteogen is placed around the implant (*). Collagen dressing covers the opening of the remaining socket. The wound is protected with perio dressing, which is partially secured by an abutment (A in Fig.6). No paresthesia is reported by the patient a few hours postop.
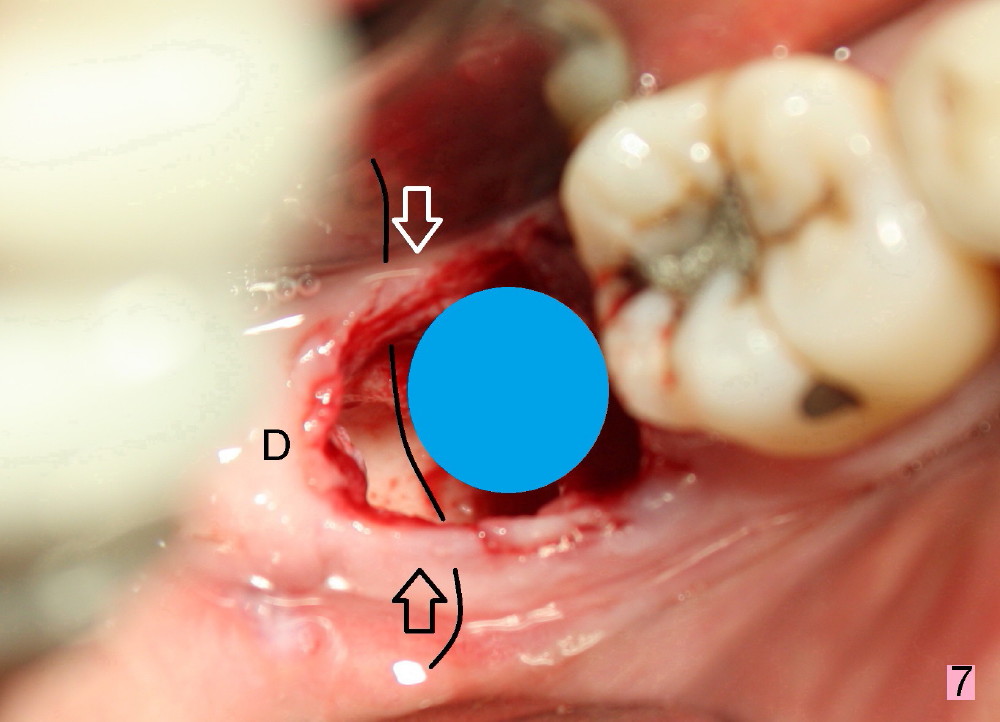
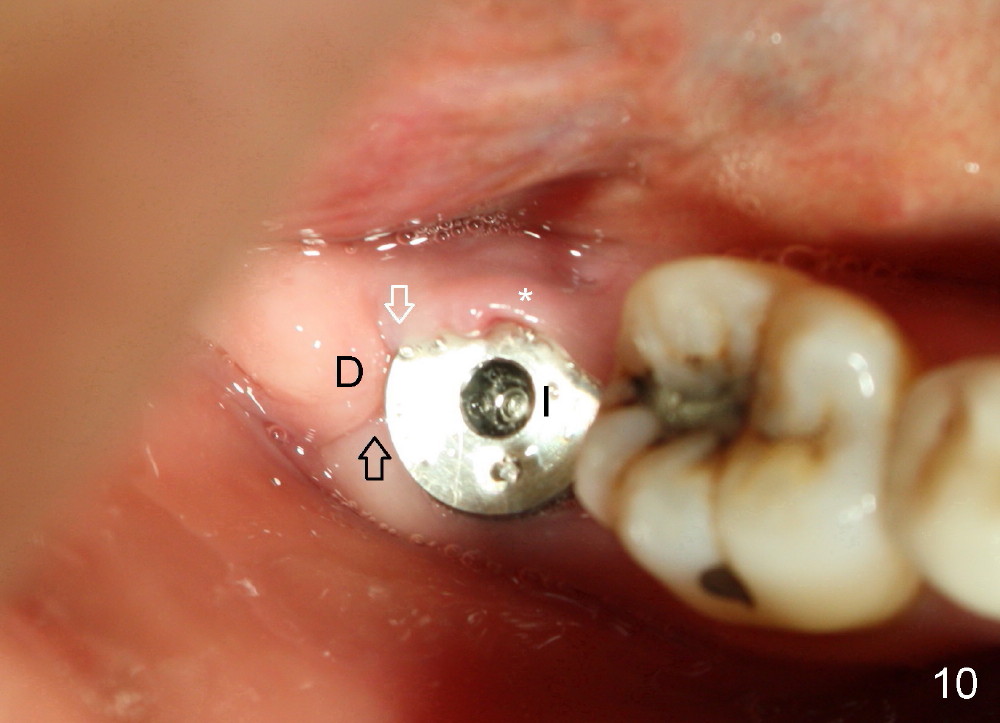
The patient returns 22 days postop (Fig.8-10). The gingiva heals around the implant. There is excess lingual gingiva (Fig.9,10 *), which should recede gradually. Fig.7 is an illustration (from Fig.4) to show how the socket is closed.. A suture is placed (black line) to approximate buccal (black arrow) and lingual (white arrow) gingiva distal to the implant (blue circle).
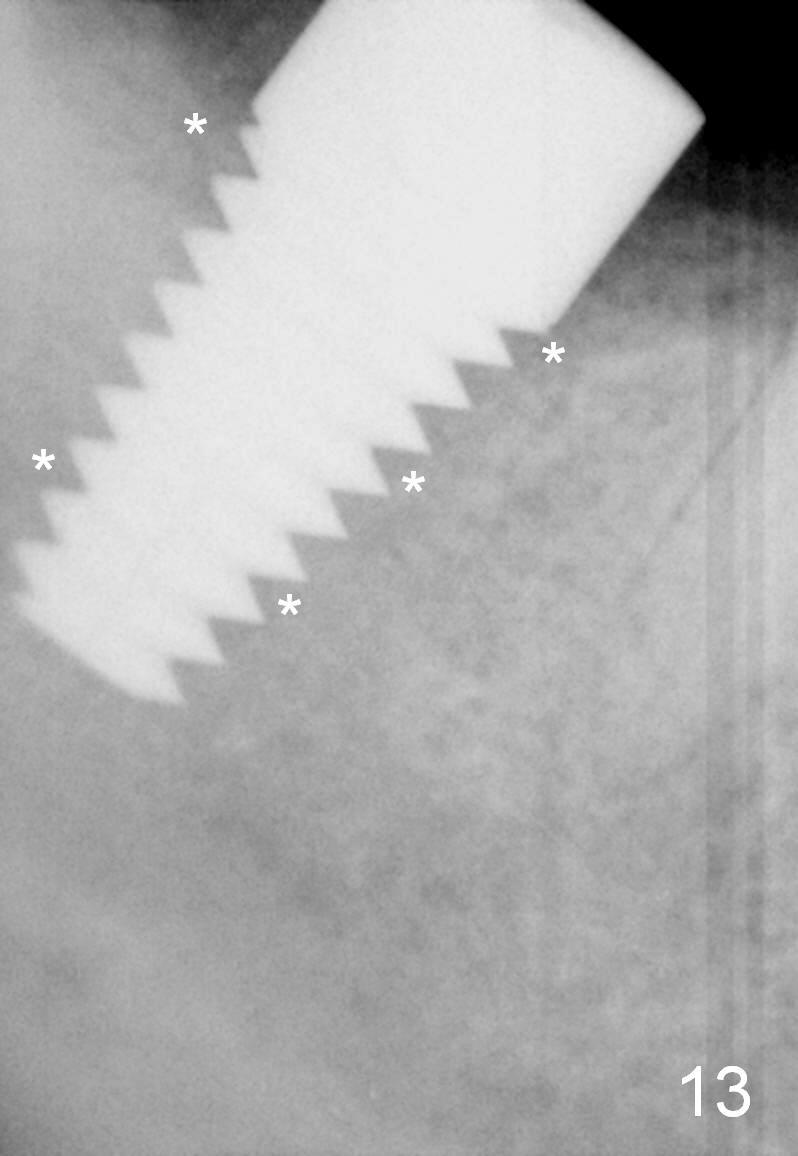
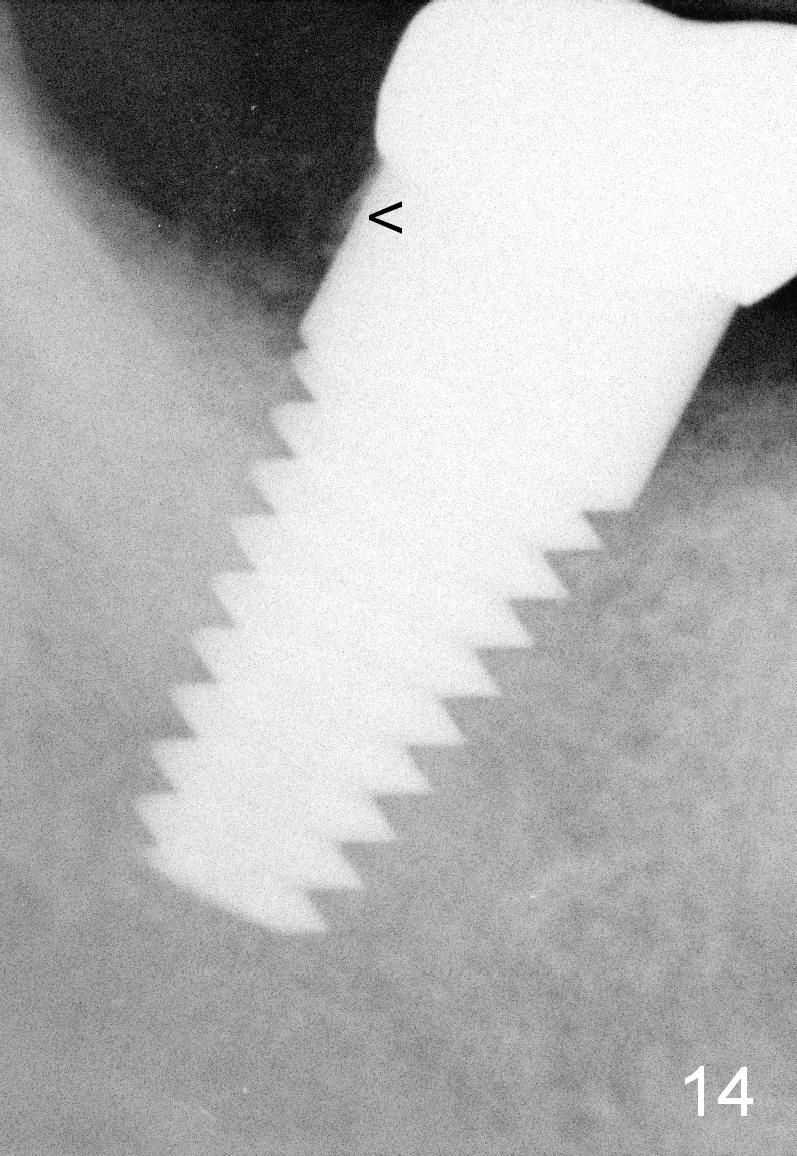
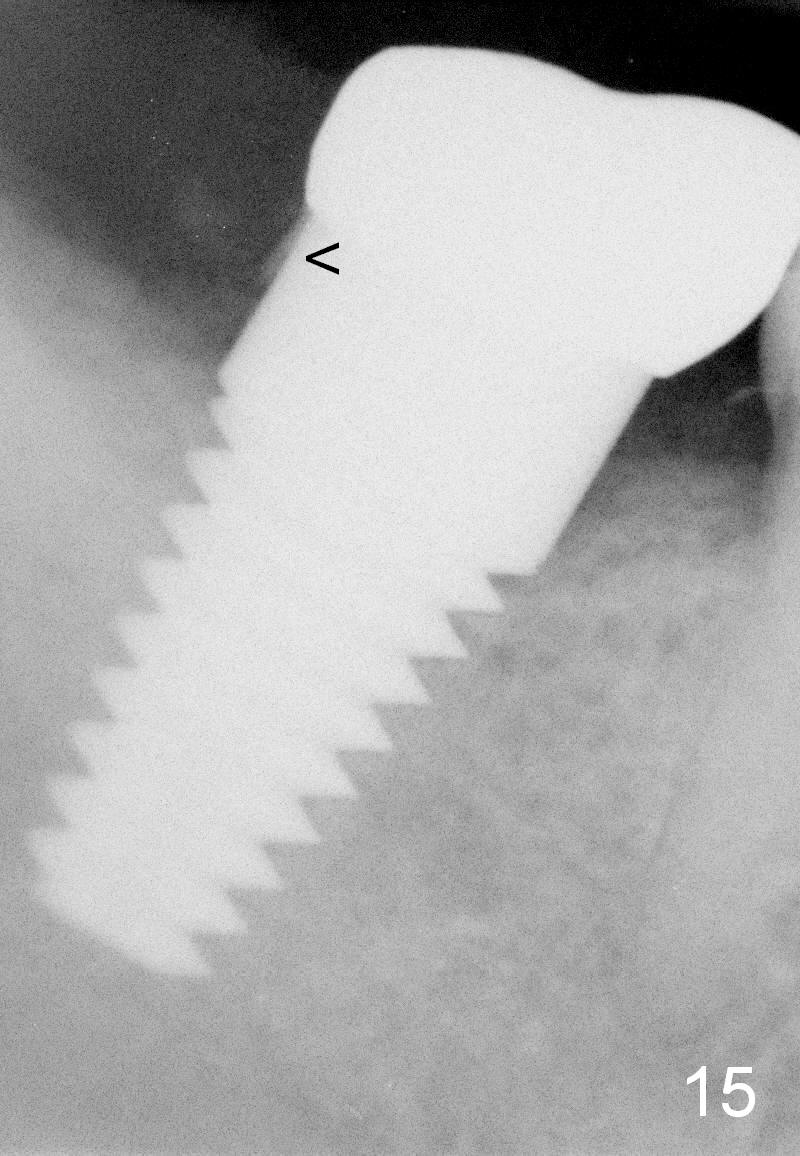
The gingiva forms a band (cuff) around the implant (Fig.11 *) and bone has apparently filled the peri-implant gap (Fig.13 *) 3.5 months postop. The gingival cuff is present immediately pre-crown cementation (Fig.12 *). The bone density around the implant continues to increase 2 and 7 months post cementation (Fig.14,15), in spite of retention of residual cement distally (<).
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 10/10/2014, last revision 09/13/2015