






|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Close vs. Open Surgery
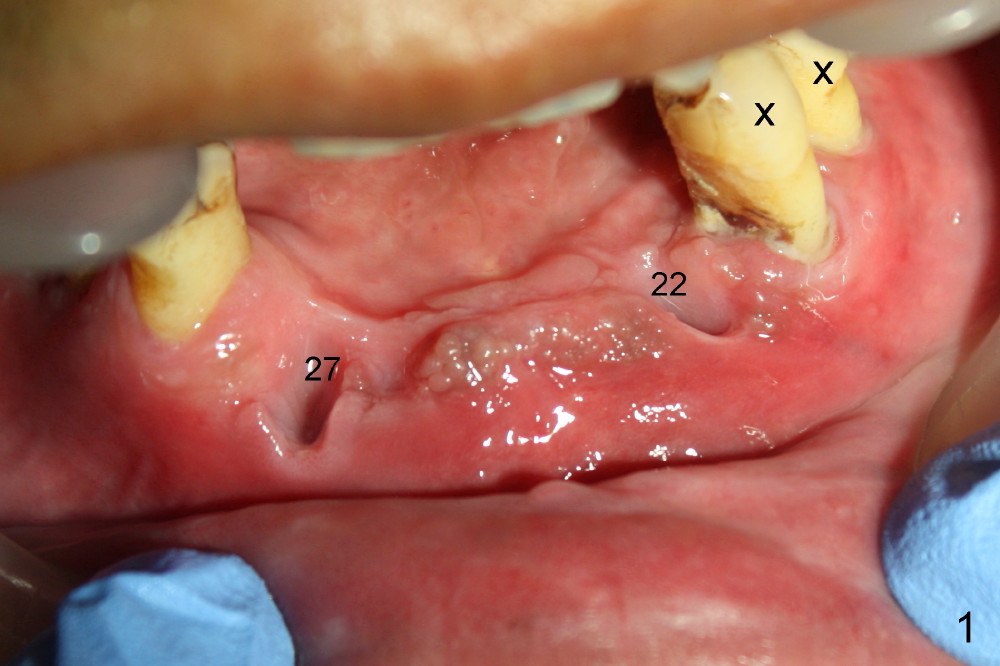
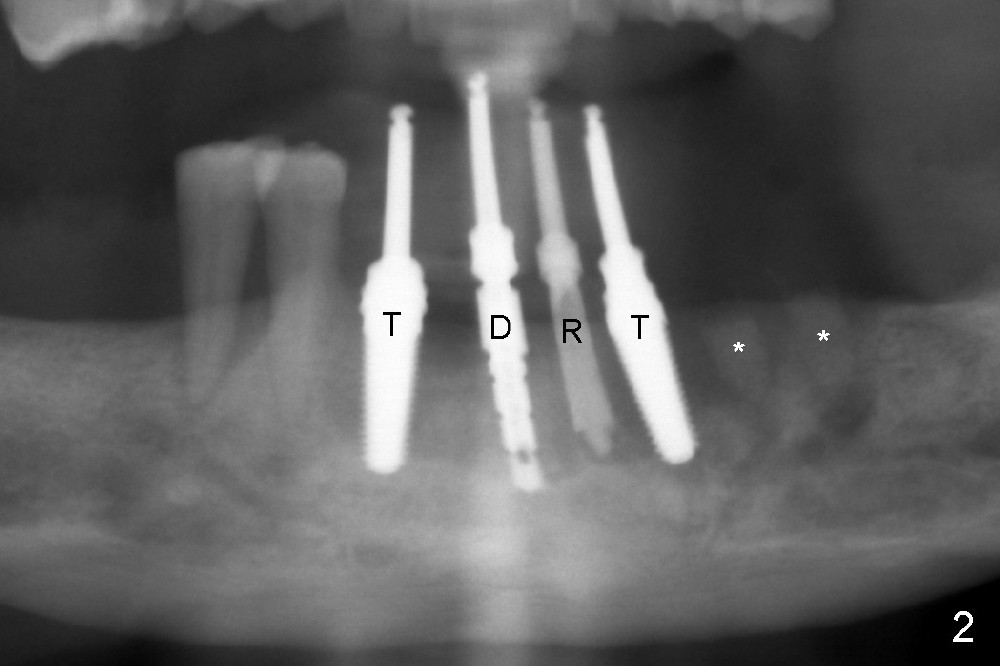
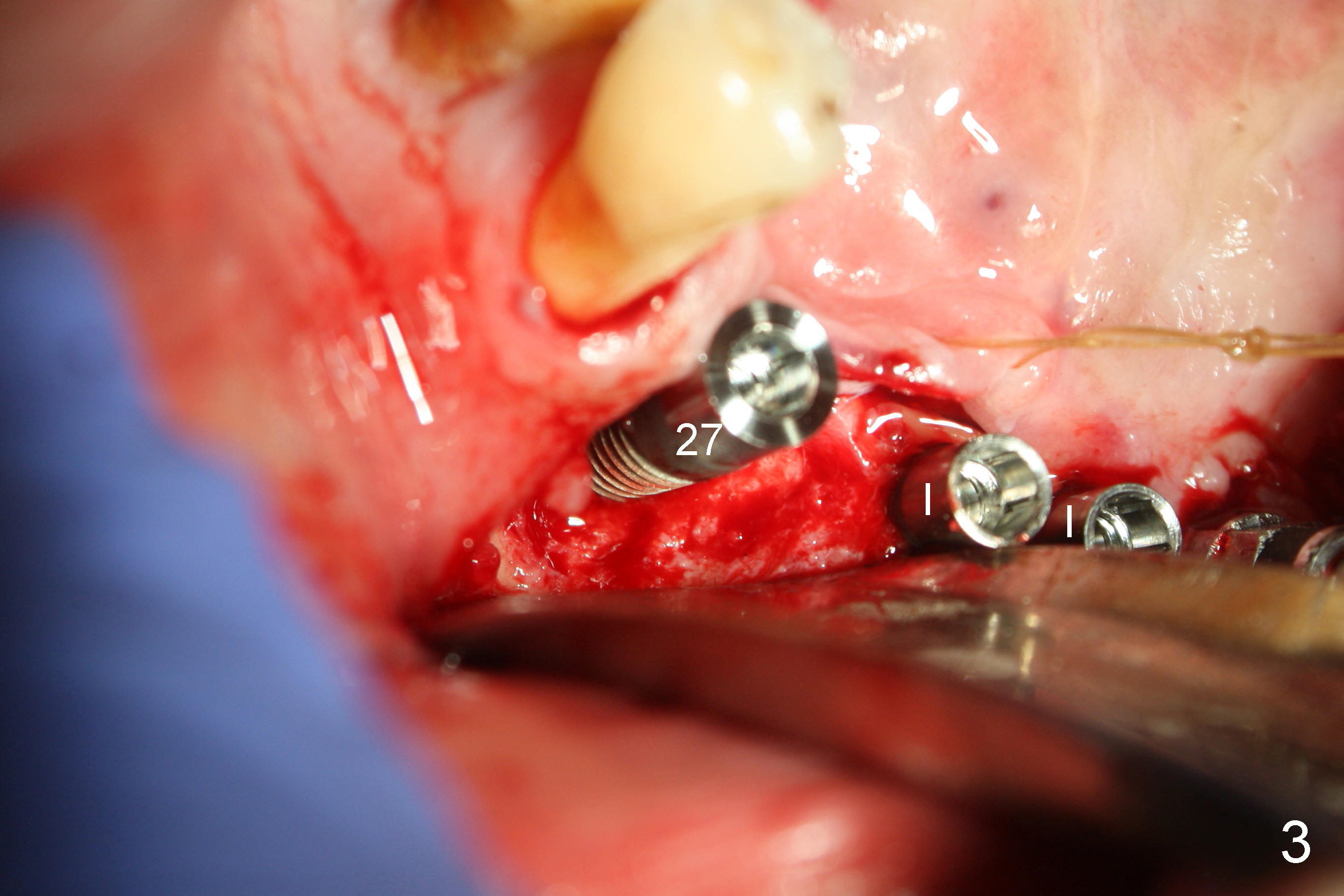
Treatment plan of the 1st surgery consists of extraction of #20 and 21/immediate implants (Fig.1 x), and placement of 4 implants between #22 and 27. Osteotomy at the extraction sites without incision (close surgery) turns out to be difficult; it appears to encroach the inferior alveolar nerve and mental loop. The sockets are subsequently bone grafted (Fig.2 *: mixture of autogenous bone and allograft). Incision is the made in the incisor edentulous region for placement of 3.5x17 mm implants (Fig.3 I).
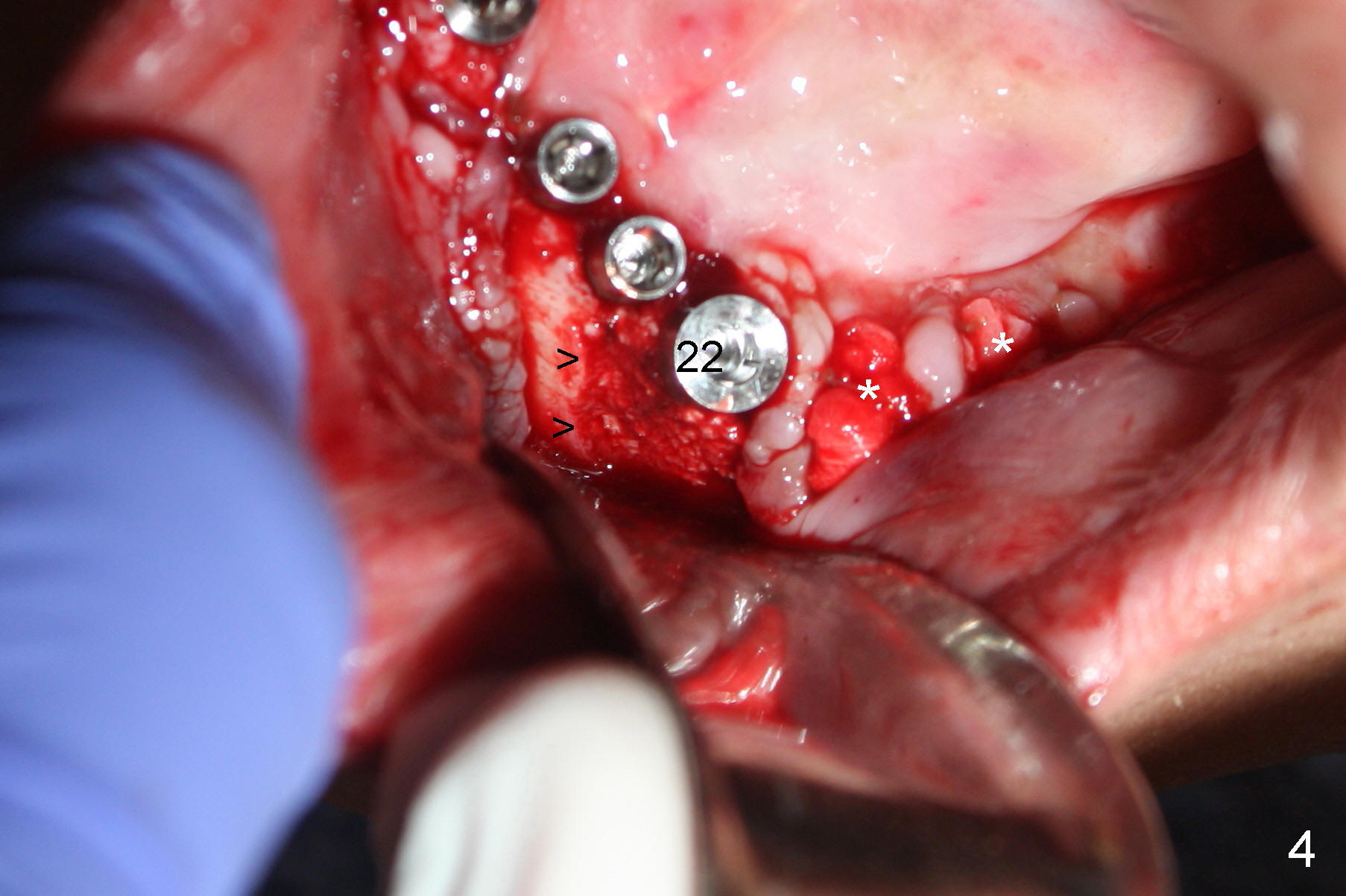
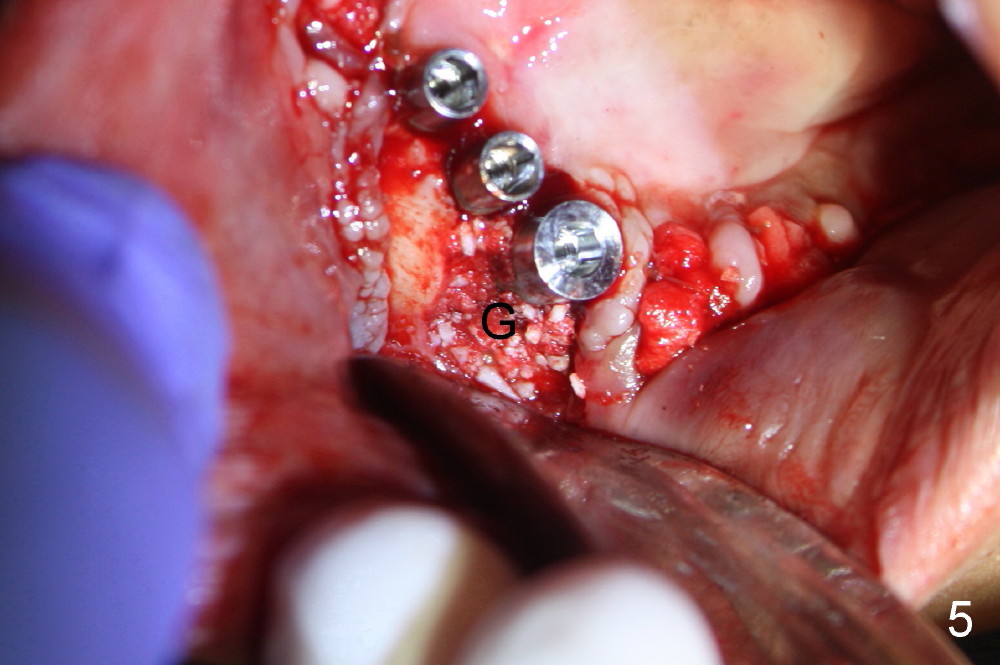
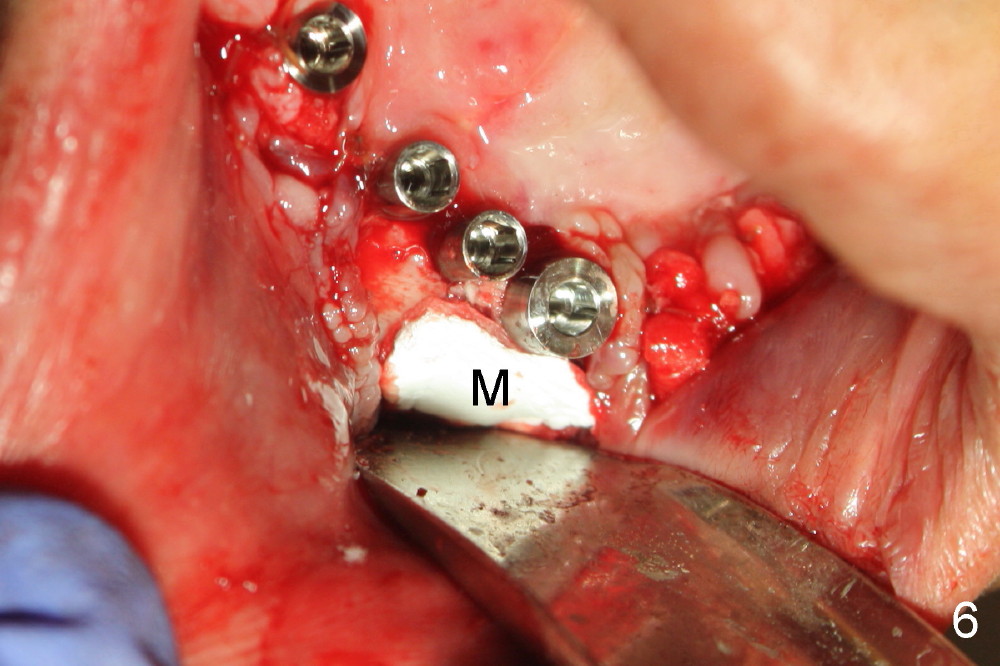
Osteotomy is initiated through the gingiva of the healing sockets at the sites of #22 and 27 (Fig.1) with difficulty (close surgery). The incisor crest incision is extended distal to the canine areas; an accessory oblique incision is supplemented to facilitate implantation (#22: 5x14 mm; #27: 4.5x17 mm) and expose the buccal defects (Fig.3,4, open surgery). The defects are grafted (Fig.5) and covered by collagen membrane (Fig.6). The incisions are closed and abutments are placed for immediate provisional (Fig.7).
Incision (open surgery) appears to help increase surgery safety and avoid complication (nerve injury) associated with immediate implant.
The wound is gapping over the implants (Fig.8), while #20 and 21 sockets are healing one week postop (Fig.9).
Once the patient improves oral hygiene as instructed, the wound around the implants begins to heal (Fig.10,11) one week later, while that continues healing around guided tissue regeneration area (Fig.12).
How to avoid paresthesia on the right side when #29 is extracted with immediate implant? In fact the implant placement at the site of #29 is aborted due to difficulty in obtaining sufficient depth of osteotomy.
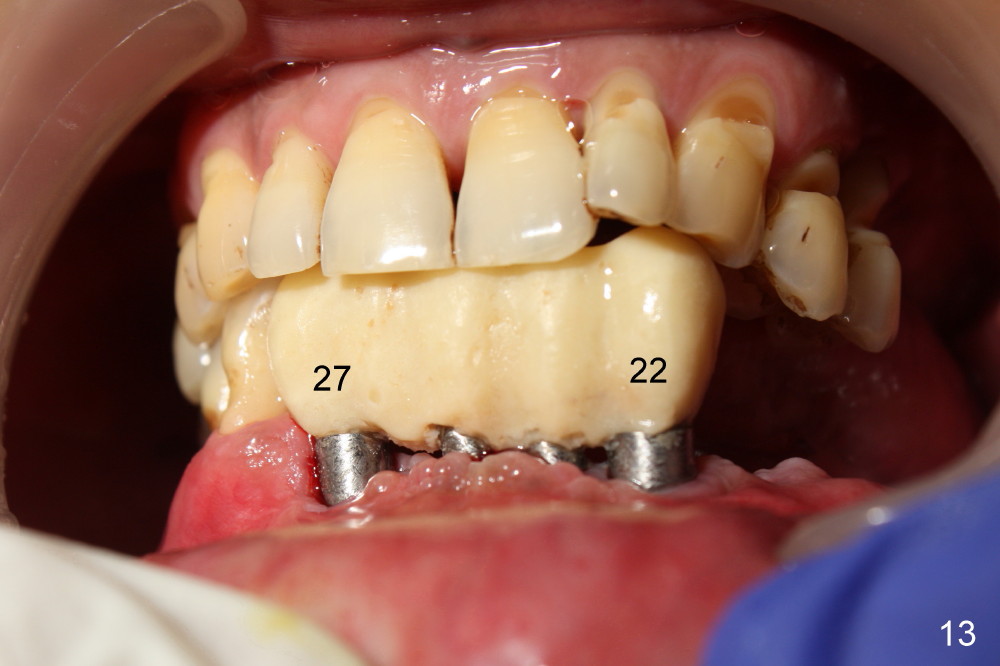
The rough surface of the implants at the sites of #22 and 27 is covered by the gingiva 2 months postop(Fig.13, as compared to Fig.10).
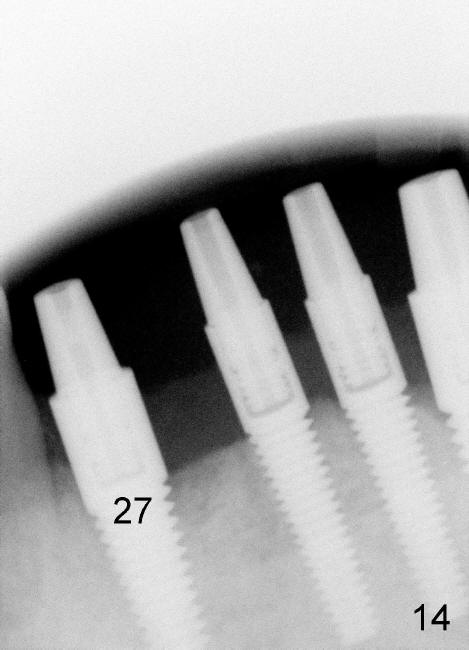
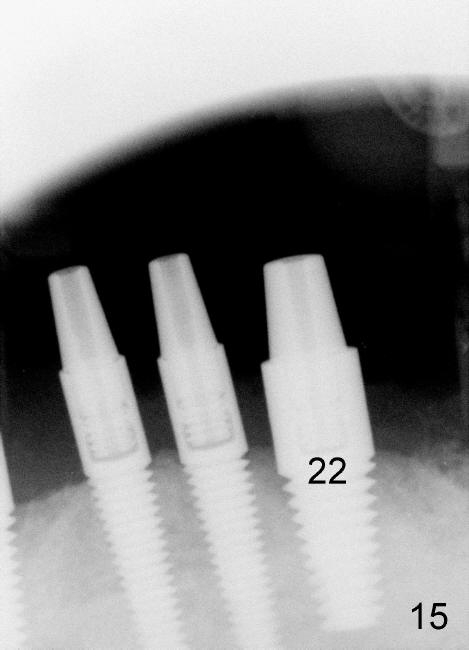
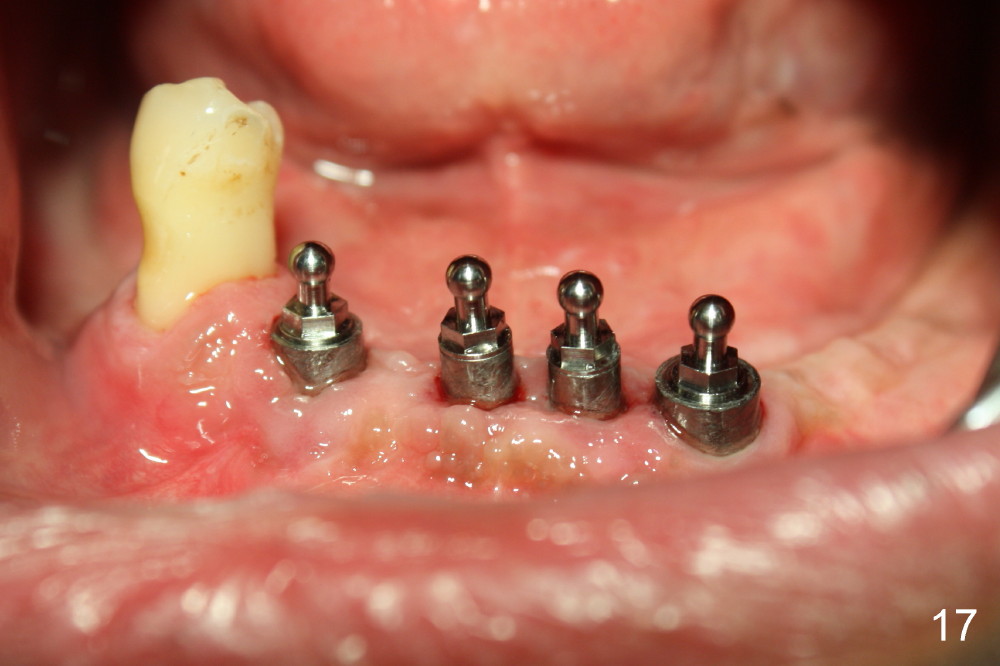
The 4 anterior implants appear to have been osteointegrated 5 months postop (Fig.14,15). More gingiva has covered the top portion of the implants (Fig.16). Ball abutments are placed for an overdenture (Fig.17).
Lower Arch Reconstruction,
Dr.
Wu
Xin Wei, DDS, PhD, MS 1st edition 09/05/2014, last revision 04/12/2015