.jpg)
.jpg)

,%20post.jpg)
|
|
|
|
|
|
|
|
|
|
Healing
Abutment Seating
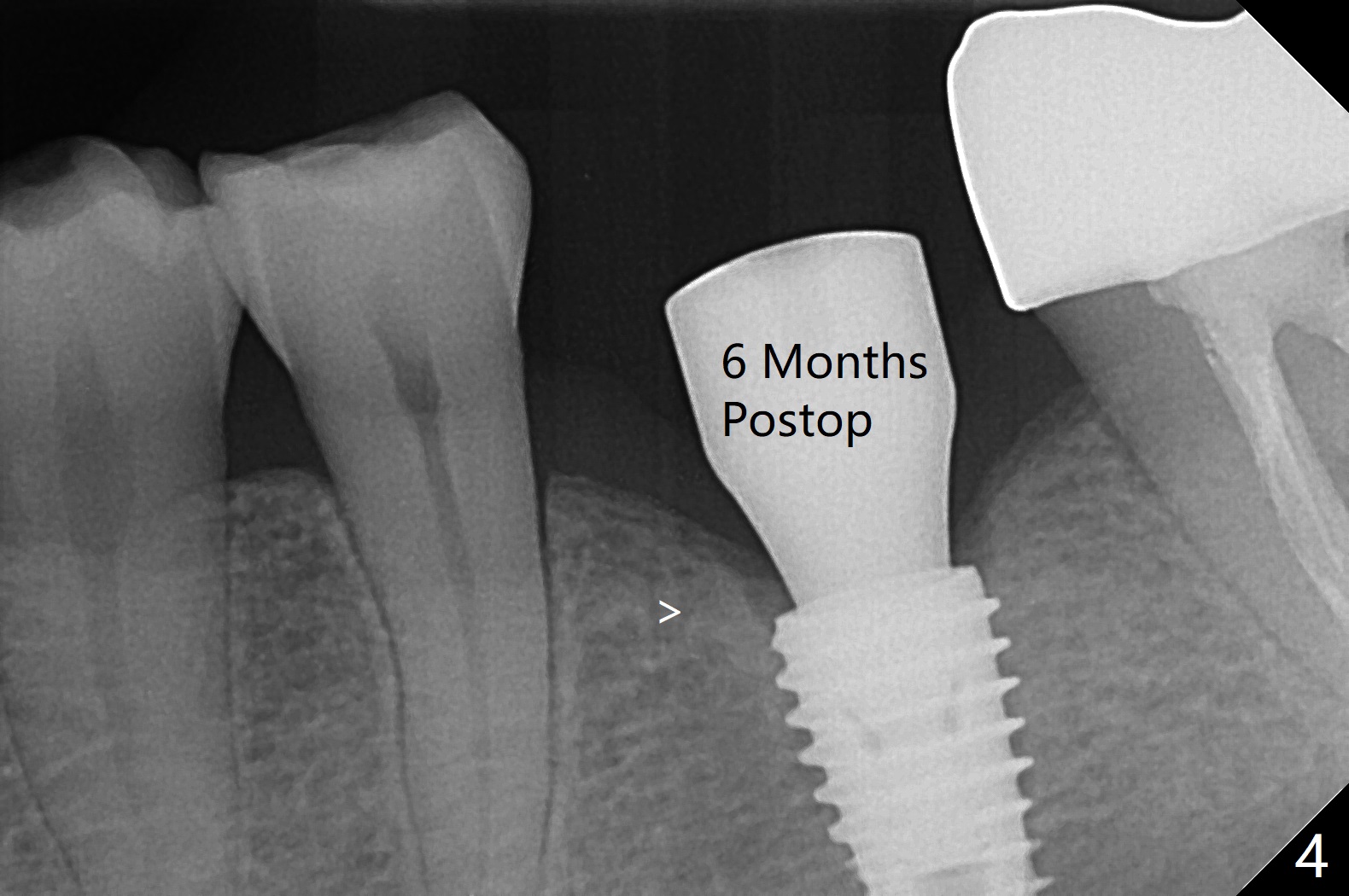
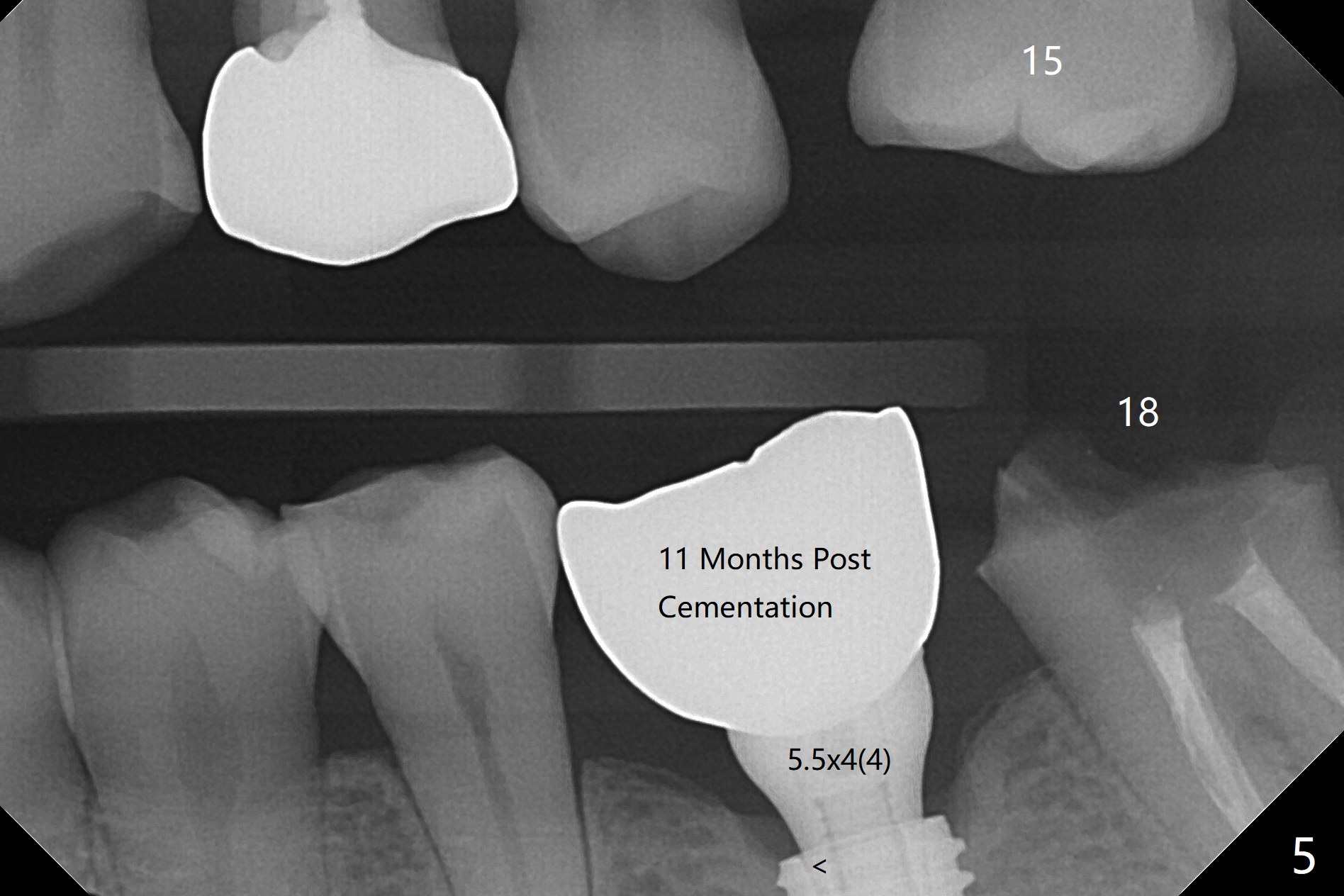
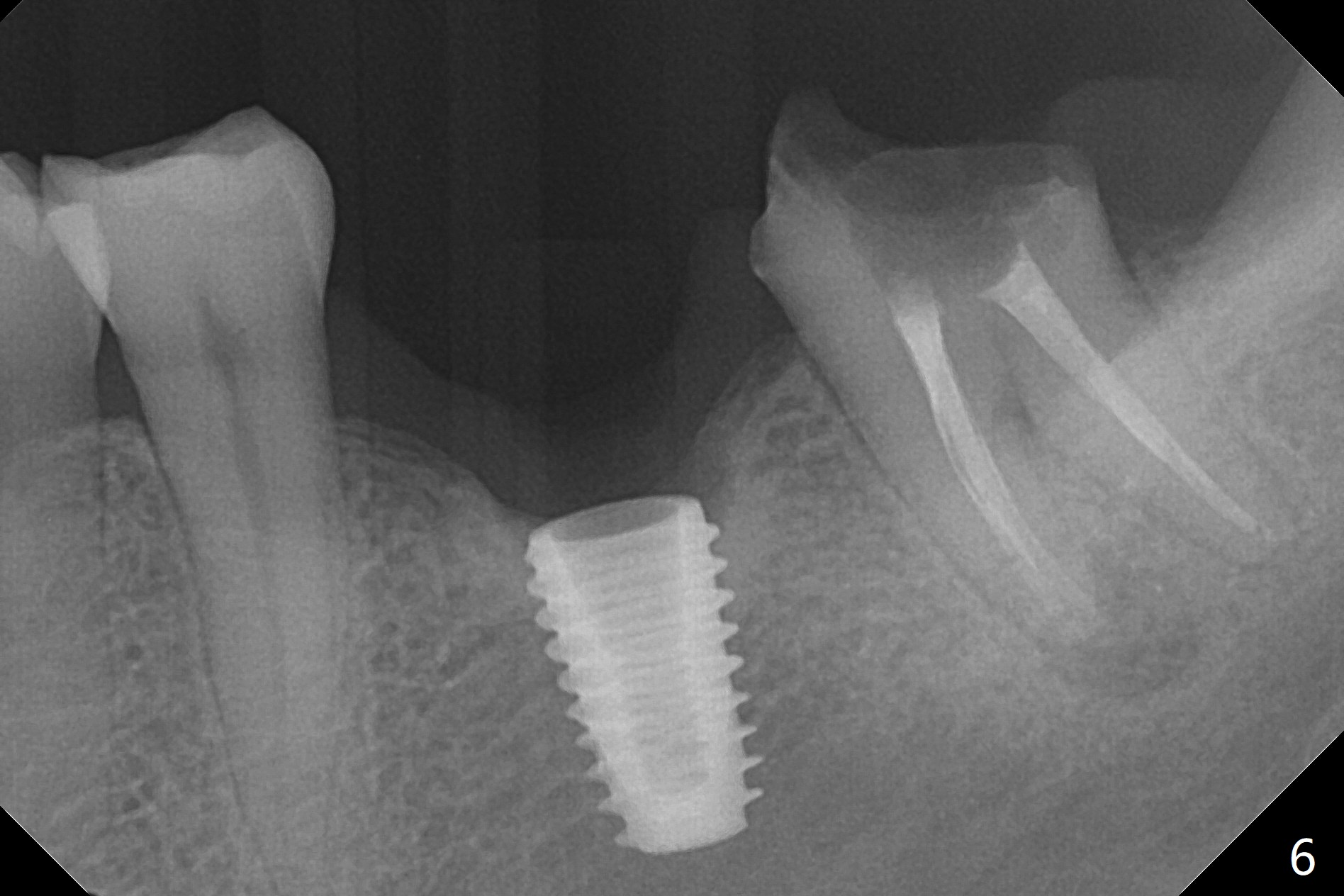
With one carpule of Xylocaine (34 mg with 17 mcg of Epinephrine), a 5x8.5 mm implant is placed at #19 in a timely and painless manner. The patient is pleased as compared to her previous implant placement at #3 and 30. Due to the thin buccal bone, the implant is placed ~.5 mm deeper than designed; a 6.5x4(2) mm healing abutment is incompletely seated (Fig.1). A smaller and skinny one (5.5x7(4) mm) is seated normally (Fig.2). Regional panoramic X-ray shows clearance from the Inferior Alveolar Canal (Fig.3 *). Although there is crestal bone resorption 6 months postop, the bone density next to the 1st thread is high (Fig.4 >). A 5.5x4(4) mm cemented abutment is placed for impression. The patient returns with #18 crown dislodgement and #19 crown loosening 11 months post cementation (Fig.5 <: gap between implant and abutment). Since the crown and abutment are unable to be torqued properly, they are removed (Fig.6). A narrower abutment is able to be seated apparently completely while a metal post (Fig.7 *) is tried in in the distal root of #18. To reduce the chance of re-fracture of #18 crown, the tooth #15 needs to be distalized orthodontically so that an implant will be placed at #14 (Fig.5).
Return to Lower Molar Immediate Implant, Trajectory Xin Wei, DDS, PhD, MS 1st edition 02/22/2019, last revision 08/05/2020