
,%20Vanilla.jpg)

|
|
|
|
|
|
|
|
Osteotomy Deviation
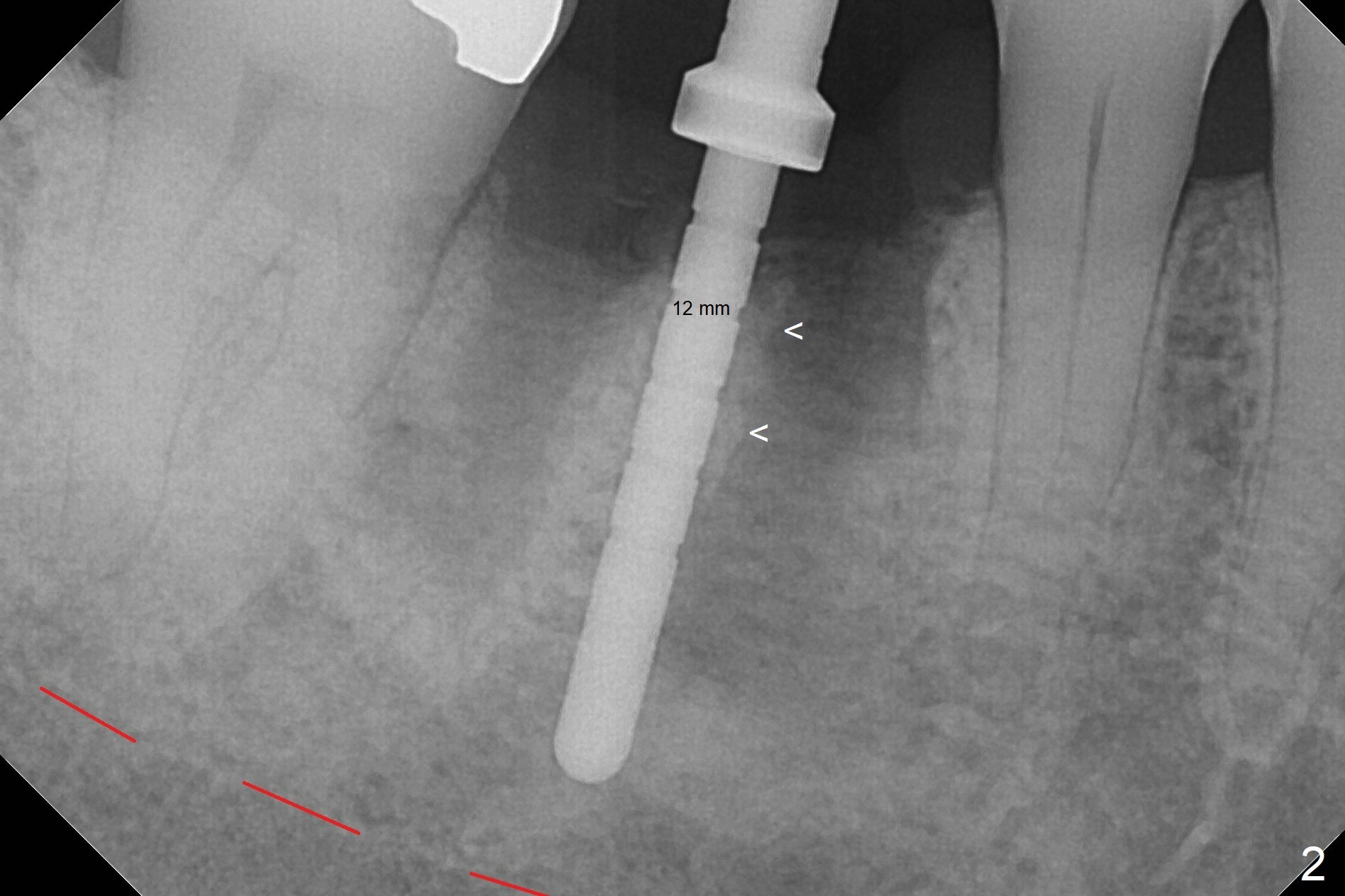
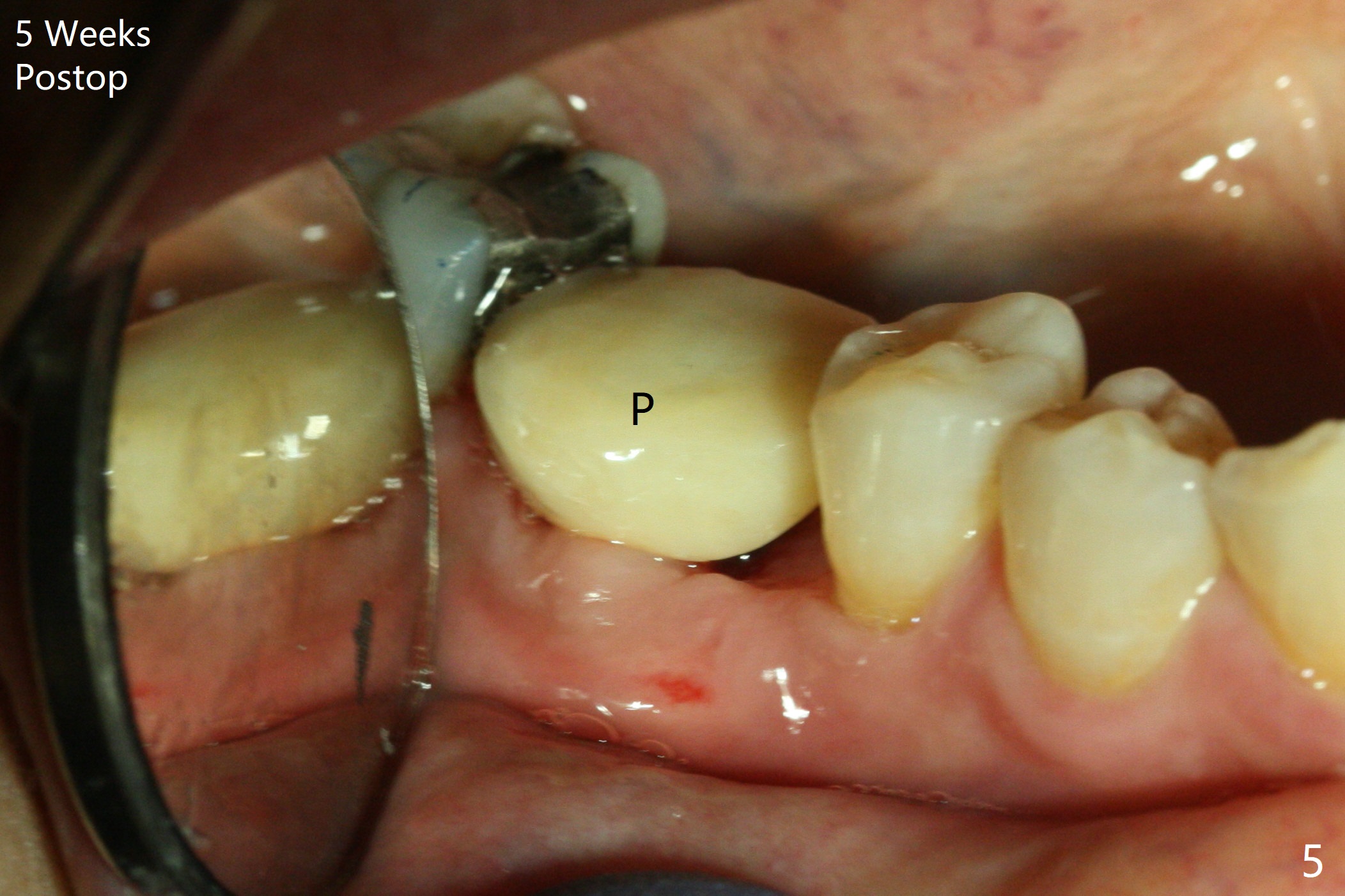
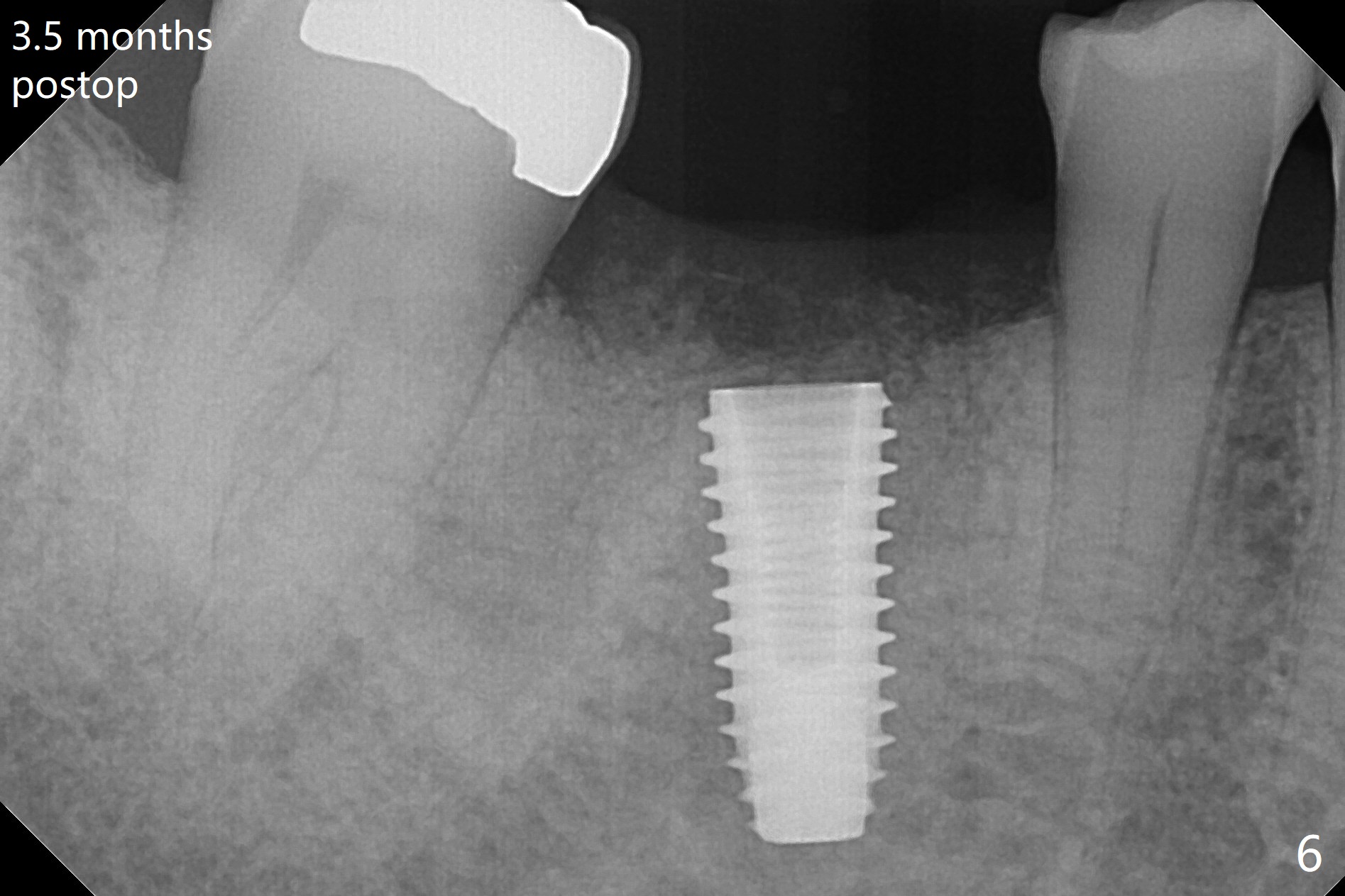
Buccal swelling is severe at #30 before extraction (Fig.1 *). Retrieval of fractured roots is extremely difficult due to hard bone. Hemorrhage seems to be inconsistent with osteonecrosis. The bone is so hard that the 2 mm drill does not reach the predetermined depth (15 mm vs. 13 mm (Fig.2)). What is ignored is the mesial deviation of the initial osteotomy (Fig.2 <). The osteotomy shifts to the mesial socket with the next drill. The severity of the deviation is not found until a 5x11.5 mm implant is placed (Fig.3). While Osteogen plug is placed in the apical socket (P), Vanilla (allograft) mixed with Osteogen in the coronal socket (*). Because of tight schedule and partial flap (to remove fractured roots), periodontal dressing is applied around the immediately placed abutment (for retention). The socket heals except mesially 3 weeks postop (Fig.4). In spite of good oral hygiene, the mesiobuccal papilla defect remains 5 weeks postop. A provisional (Fig.5 P) is fabricated for easy self cleansing. The implant seems to have osteointegrated 3.5 months postop (Fig.6, a month post abutment dislodgement). Screw loosens 4 months postop with buccal access hole and wide buccolingual width.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments Xin Wei, DDS, PhD, MS 1st edition 05/31/2018, last revision 03/06/2019