


|
|
|
|
|
|
|
|
|
|
|
|
|
|
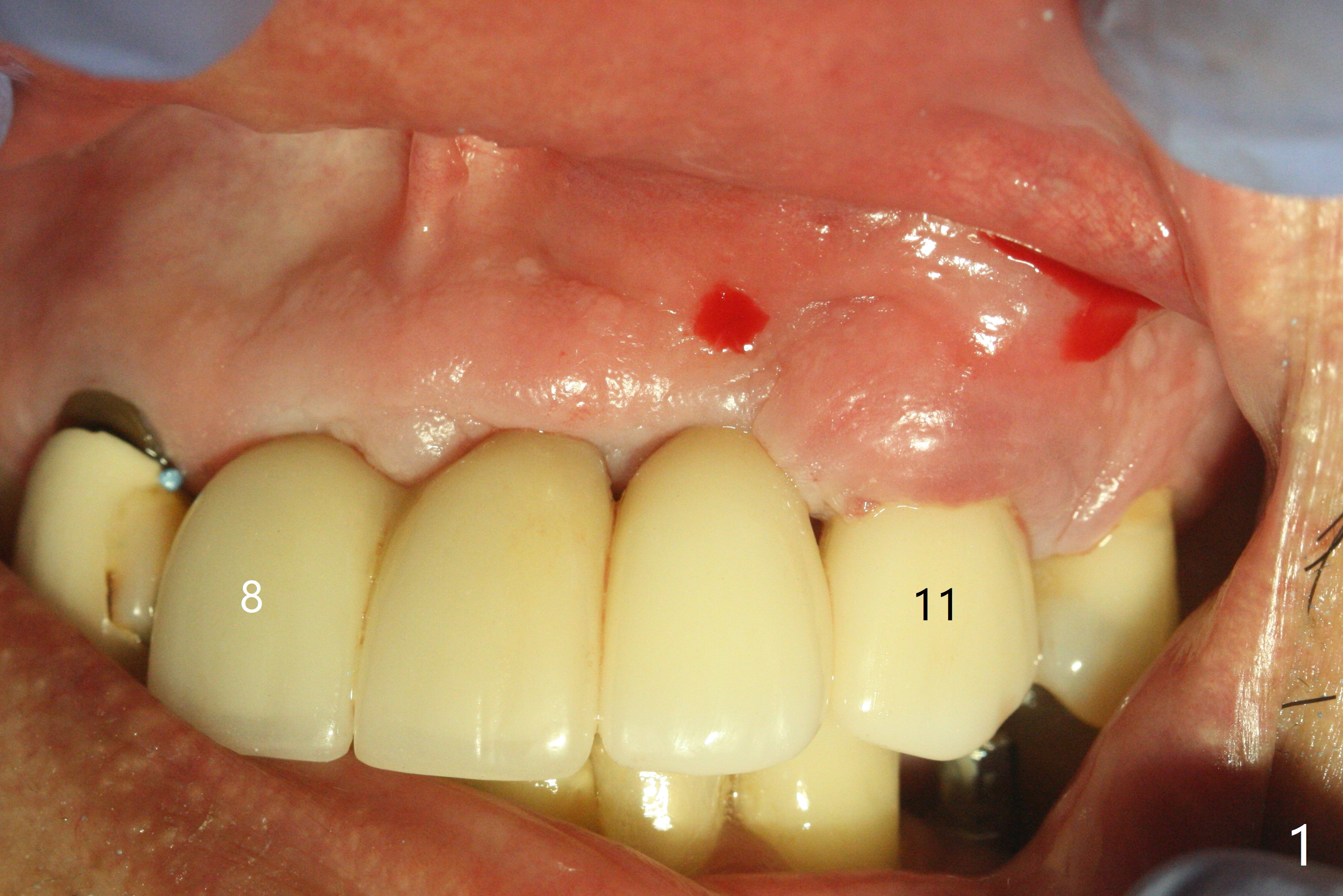
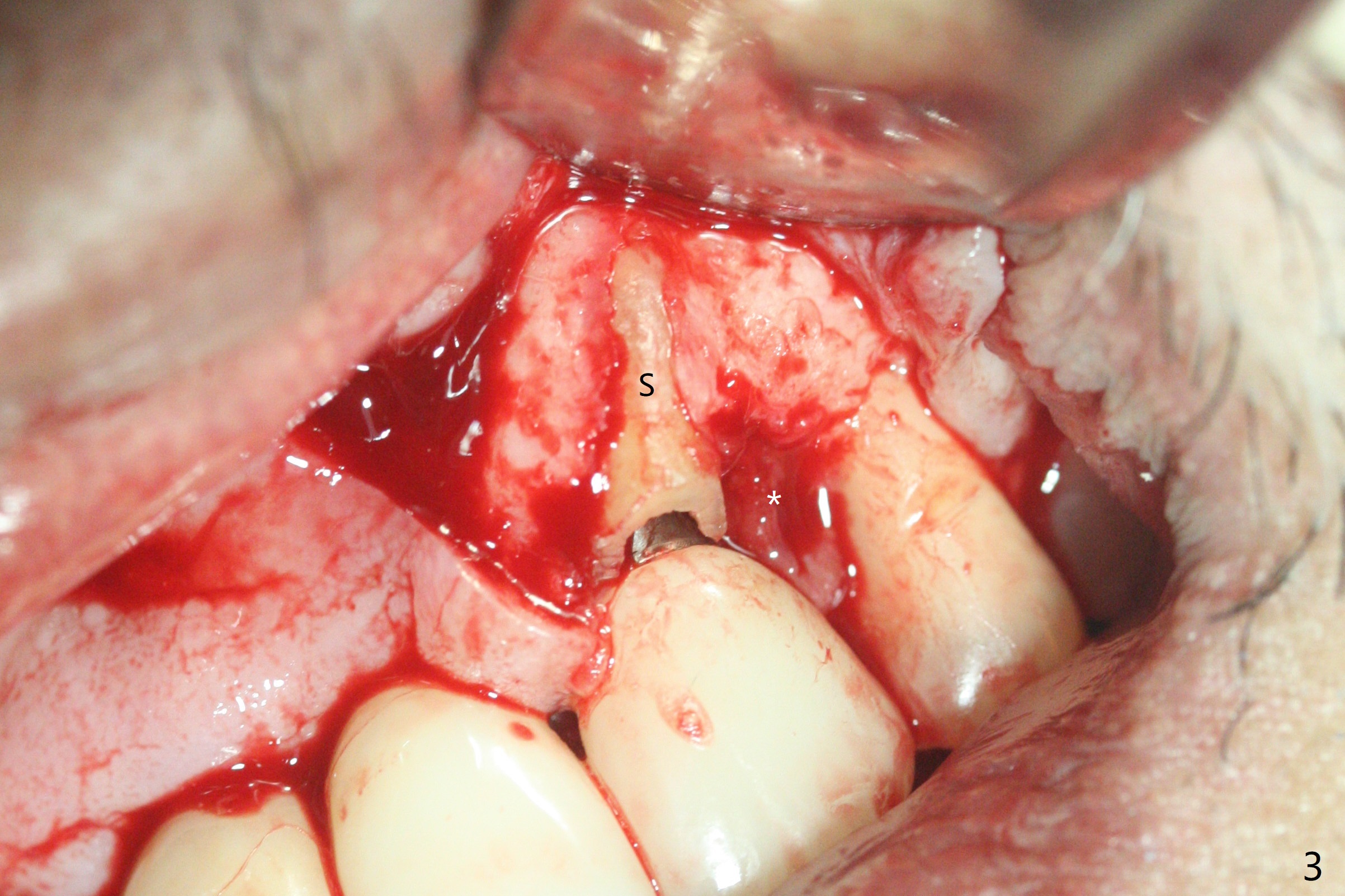
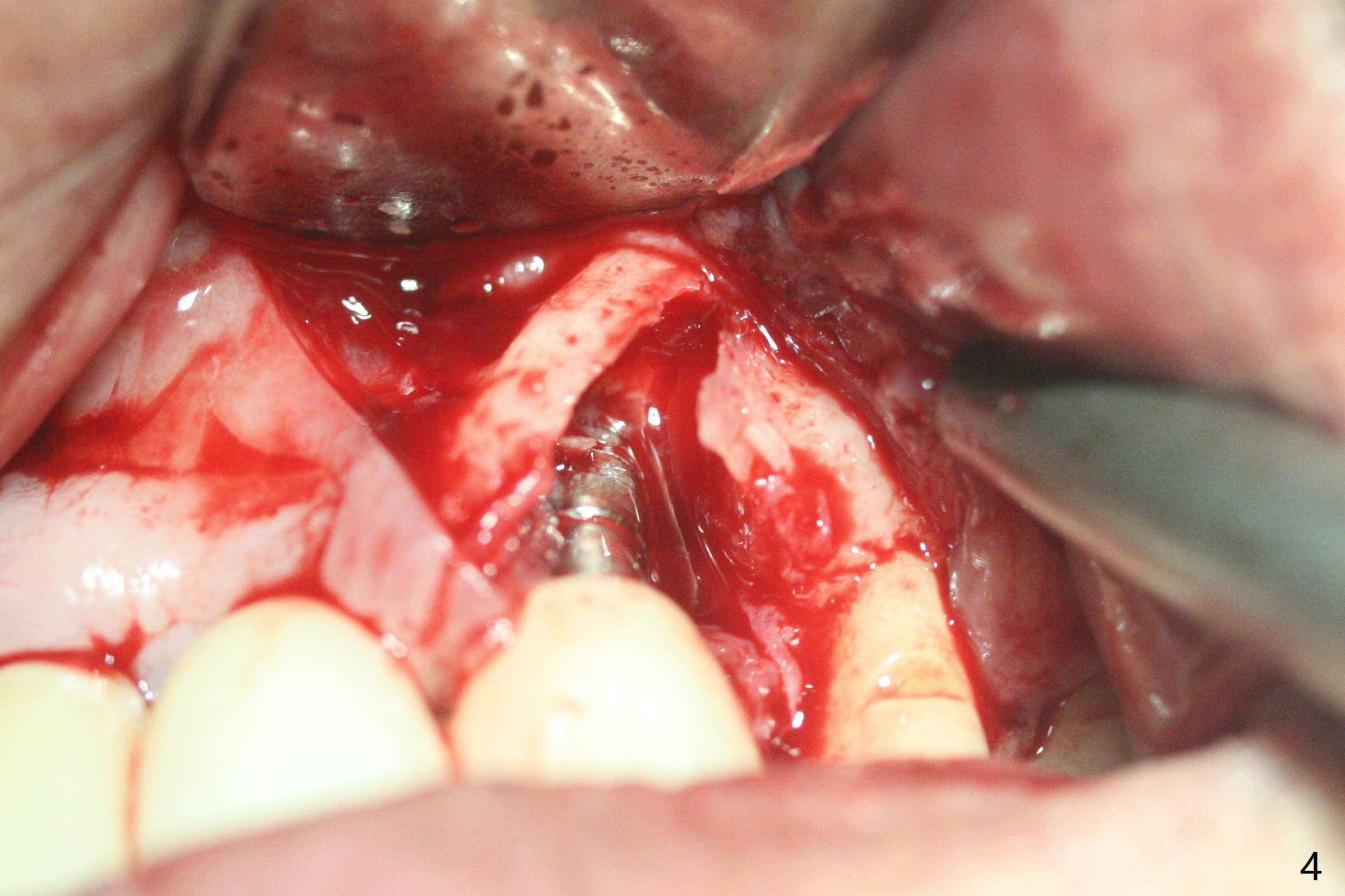
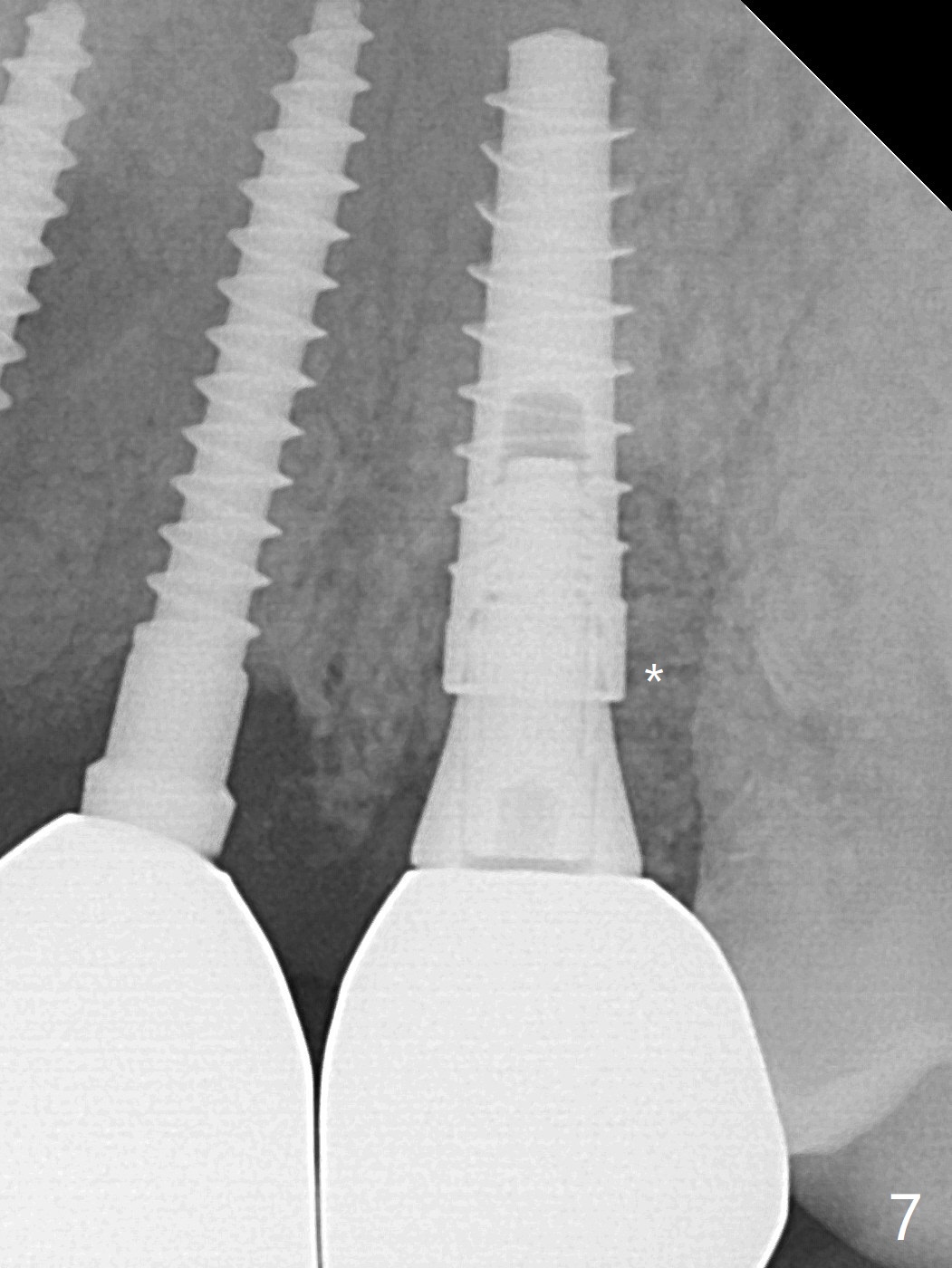
Removal of Socket Shield
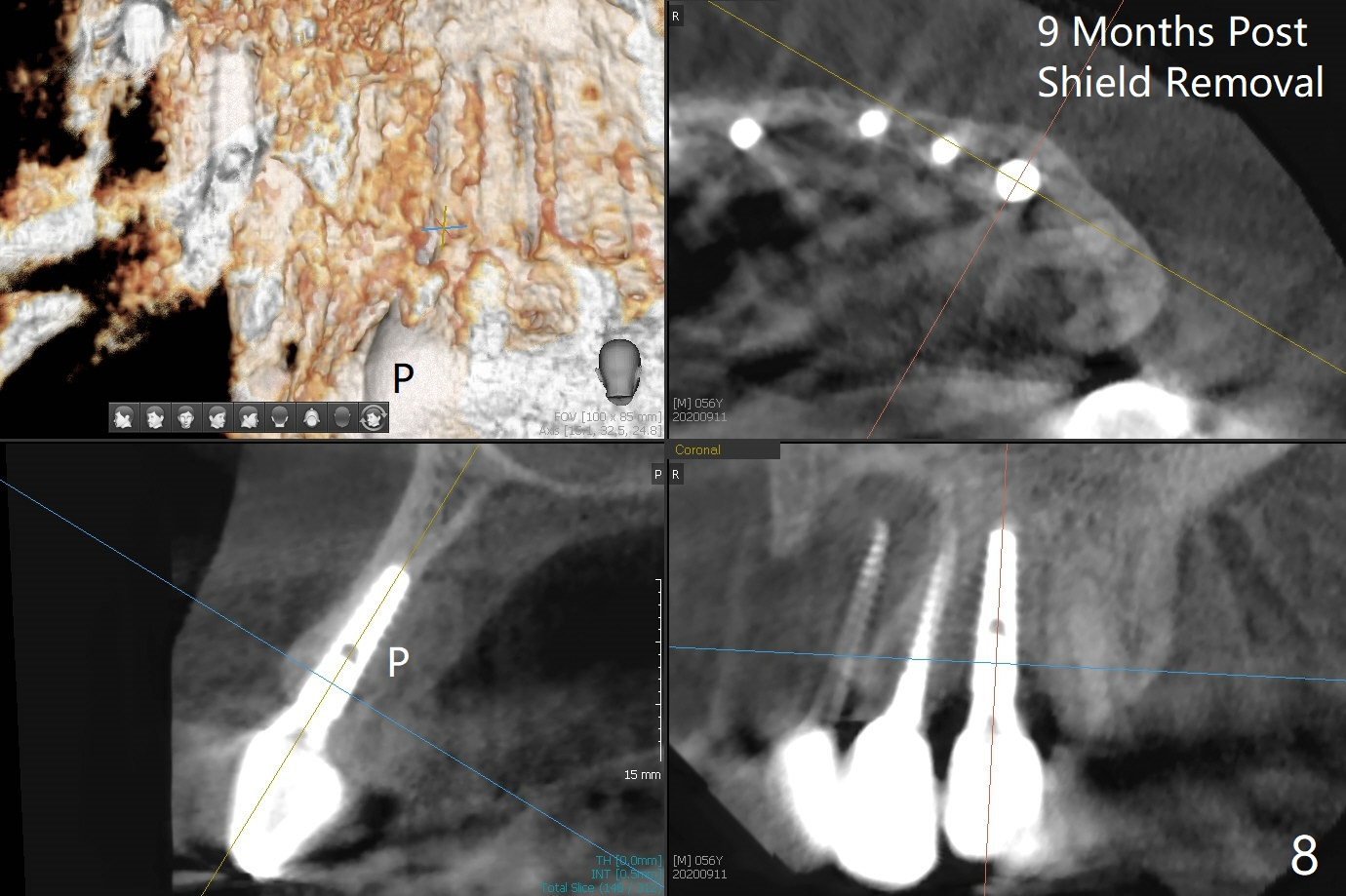
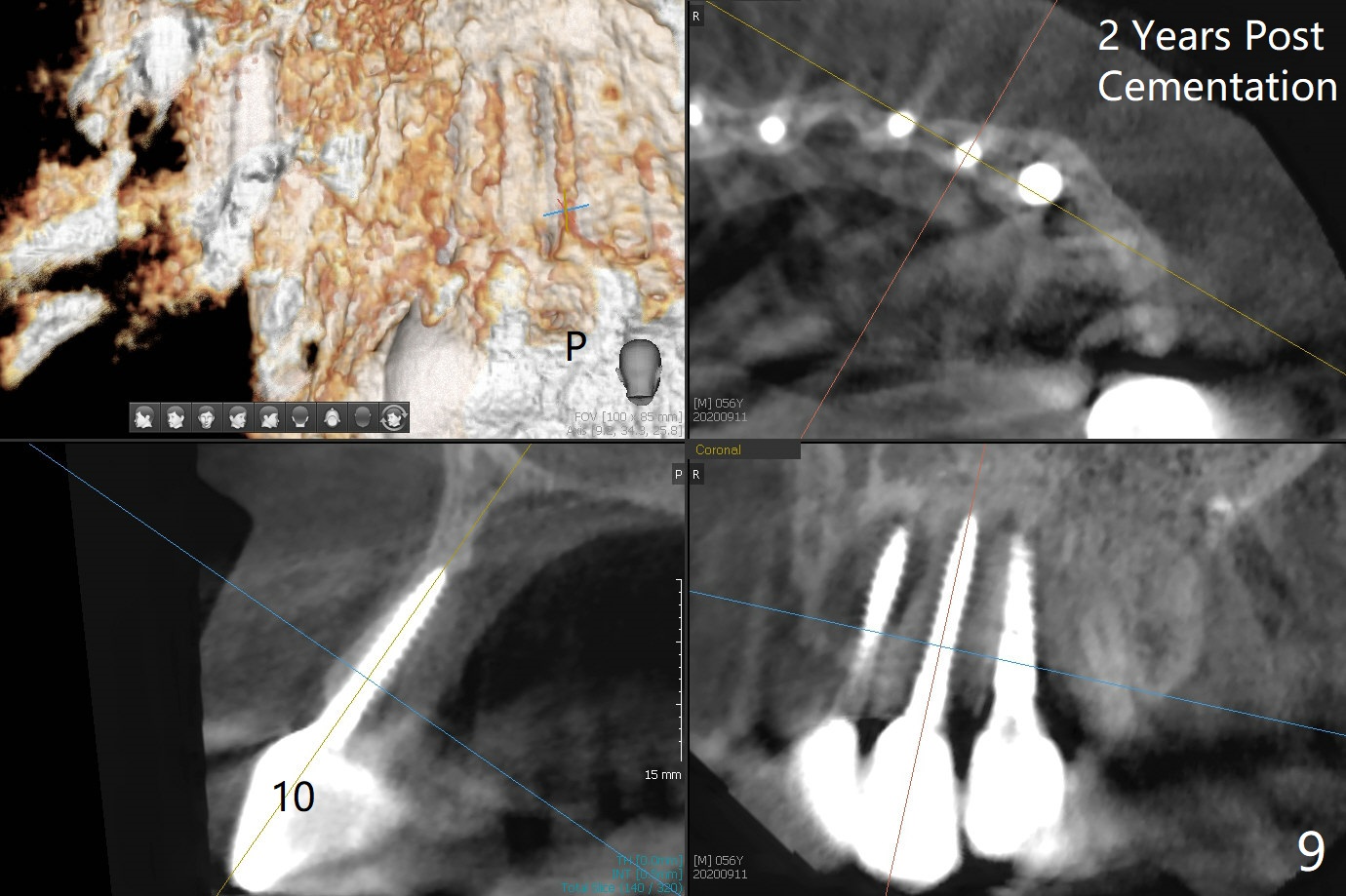
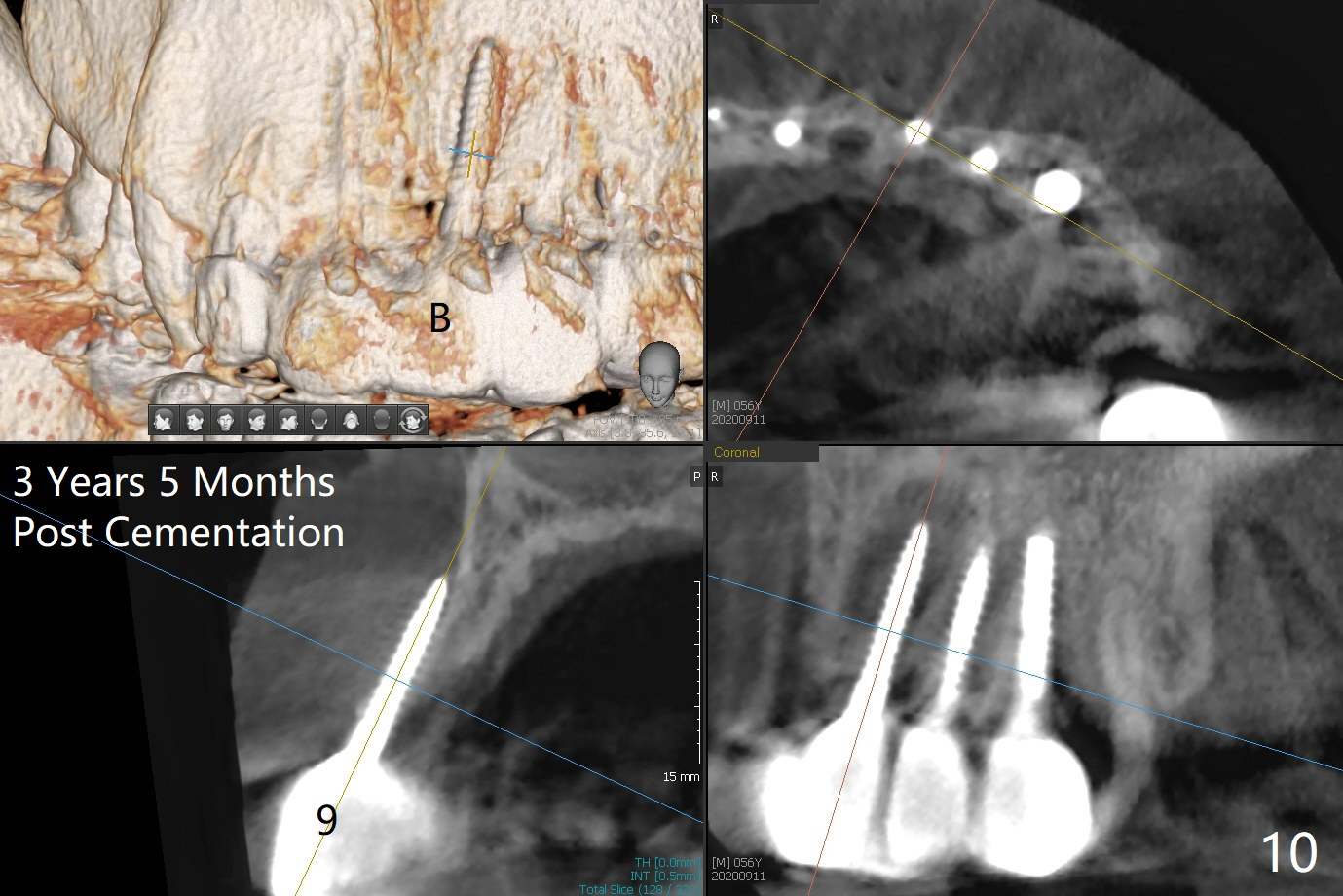
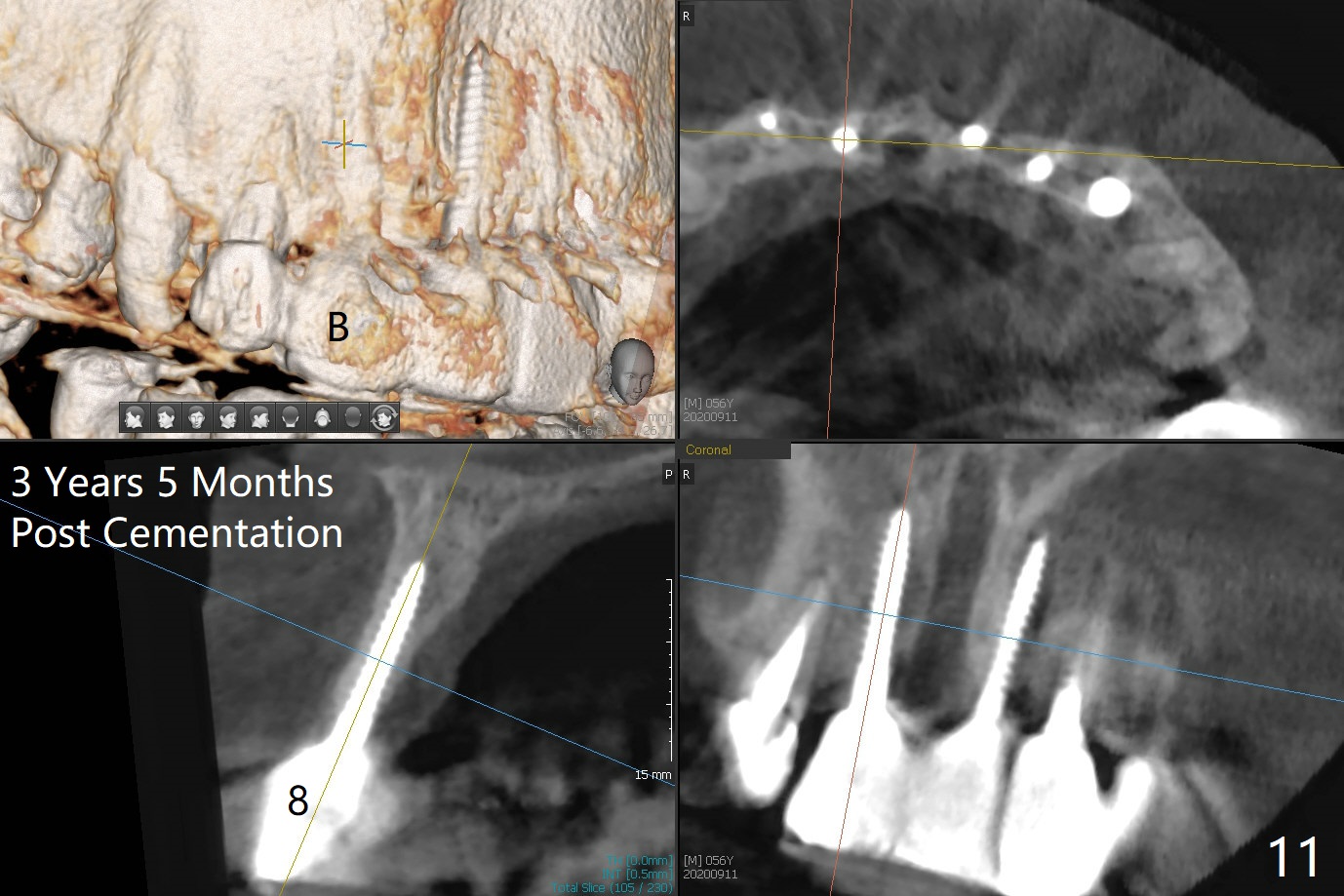
There is no obvious black triangle between the implants at #8-11 (Fig.1 post infiltration). Following papilla (Fig.2 *) sparing incision and elevation of the buccal flap, the fenetration of the buccal plate around the socket shield (Fig.3 S) is found at #11; there is a distal defect with granulation tissue (*). After shield and granulation tissue removal, the coronal implant is found exposed (Fig.4 until osteotomy). The relatively flat surface of IBS implant is apparently less likely to develop periimplantitis. With periosteal relief and placement of sticky bone (Fig.7 *), PRF and 6-month membrane, the wound is closed with 4-0 PTFE suture (Fig.5). Failure of socket shield is related to retention of the apex (Fig.6 <). Probe before extraction and remove apex and gutta percha. There appears no buccal or palatal (P) defect 9 months post shield removal (17 months post cementation, Fig.8), although the bone density palatally is low. Although the sagittal section (Fig.9 (lower left panel) shows the absent palatal plate at #10, the 3-D image and the coronal section do not (upper let and right panels). The 2.5 mm implant at #9 appears to have been placed buccal (Fig.10 B), although the buccal crest is present. In contrast the 2.5 mm implant at #8 appears within the bone boundary (Fig.11). The soft tissue remains healthy at #8-11. Bone graft will be done if needed.
Return to
Upper
Canine Immediate Implant,
Trajectory II
Shield
18/19
Xin Wei, DDS, PhD, MS 1st edition
12/16/2019, last revision
09/13/2020