
.jpg)

Return to Upper Incisor Immediate Implant, Trajectory II 1-Piece Prevent Fracture
Xin Wei, DDS, PhD, MS 1st edition 10/01/2019, last revision 06/12/2020
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
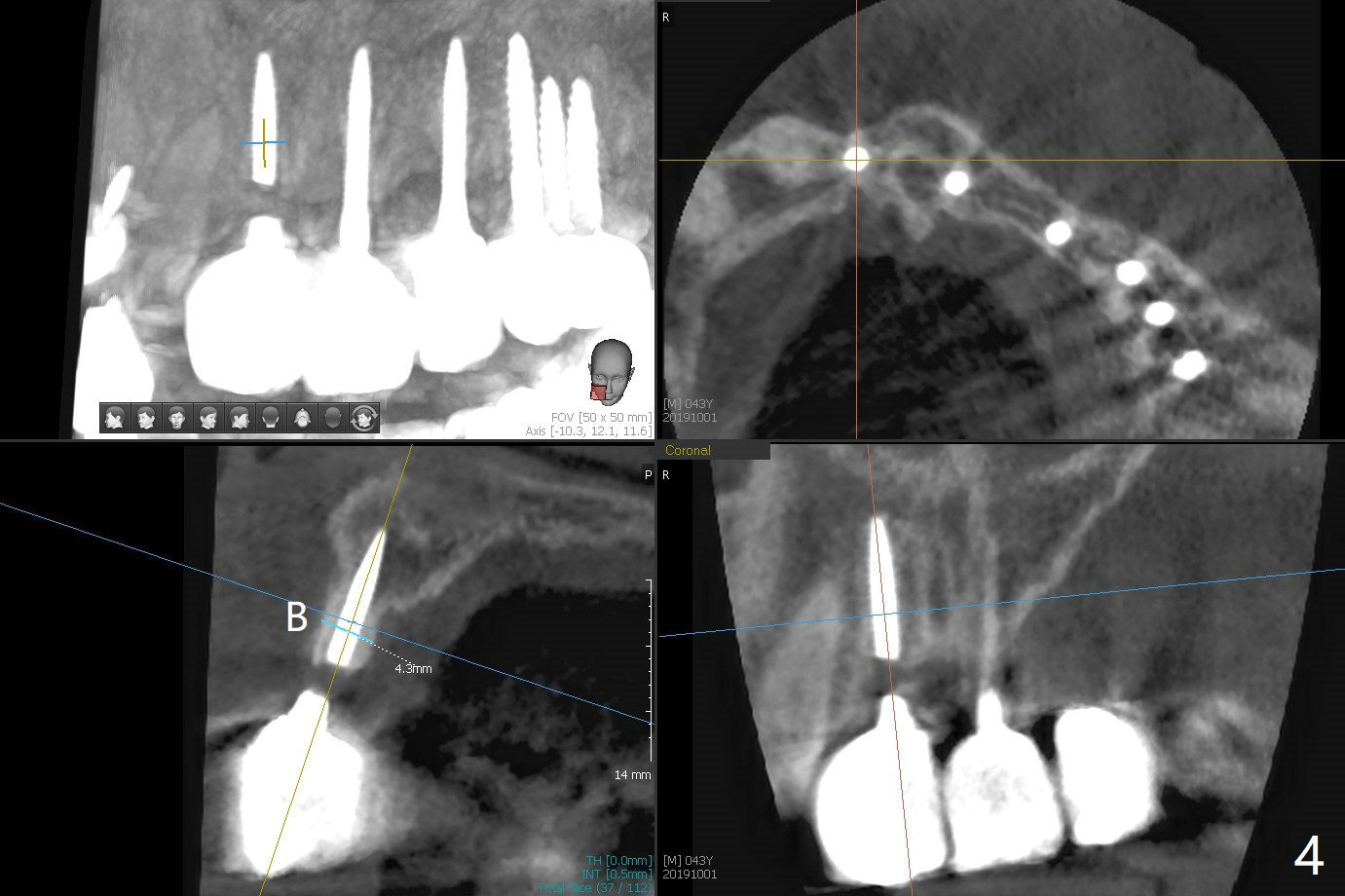
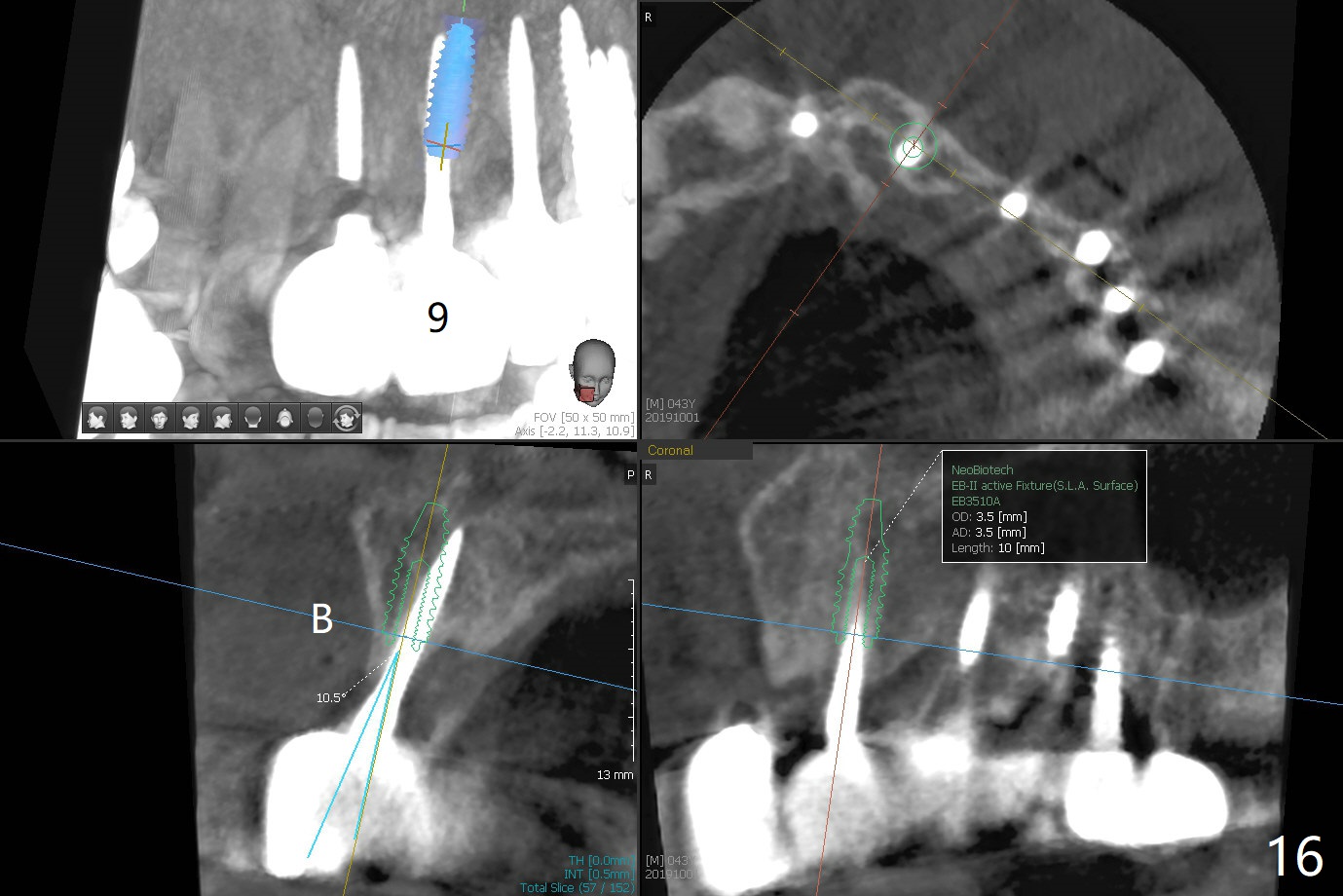
The ridge is wide enough for a 3.5x10 mm
implant (Fig.16 (CT taken when #8 implant fractured)). Return to Upper Incisor Immediate Implant, Trajectory II 1-Piece Prevent Fracture Xin Wei, DDS, PhD, MS 1st edition 10/01/2019, last revision 06/12/2020 |
||||
Remove Fractured Implant M
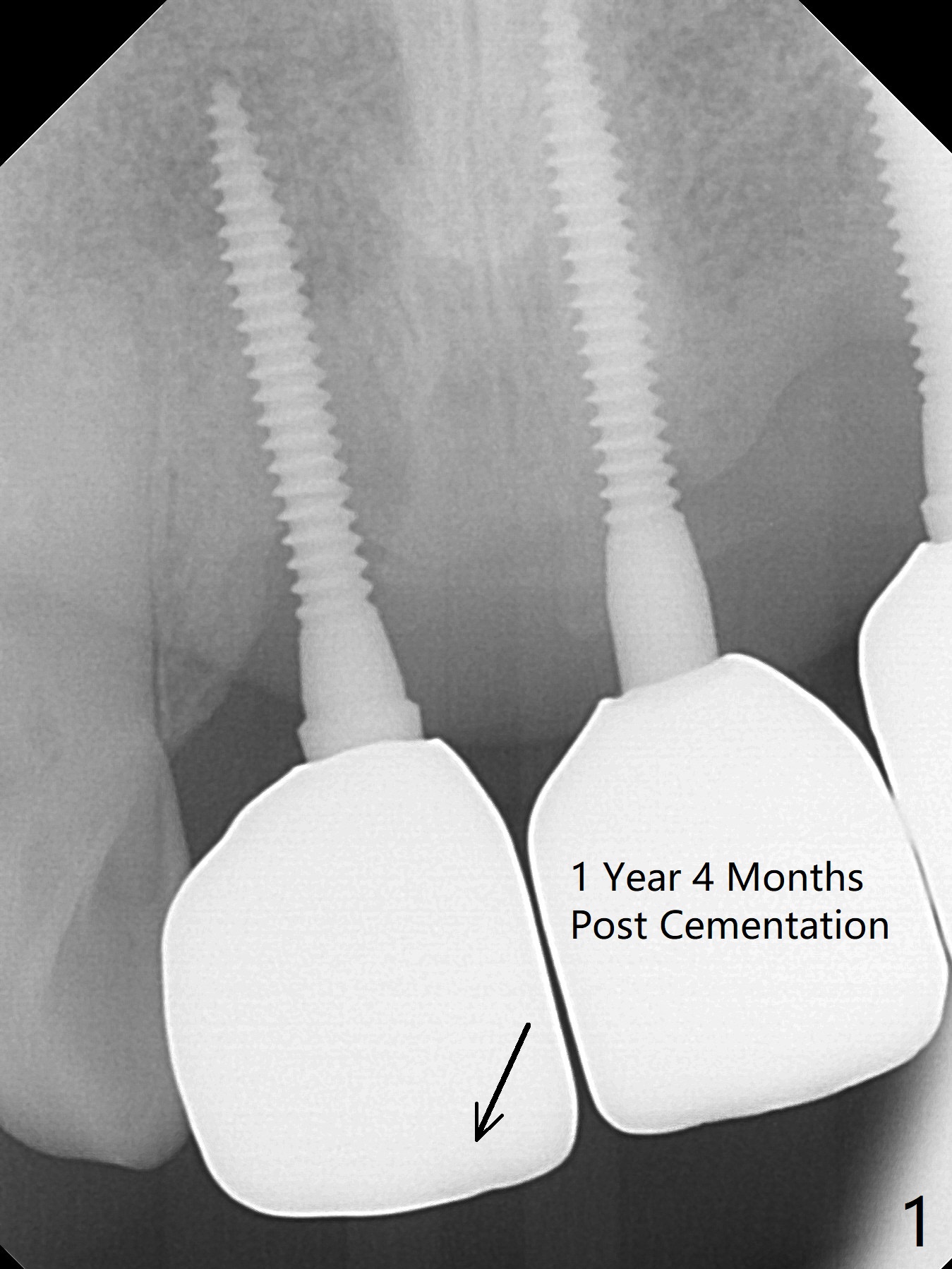
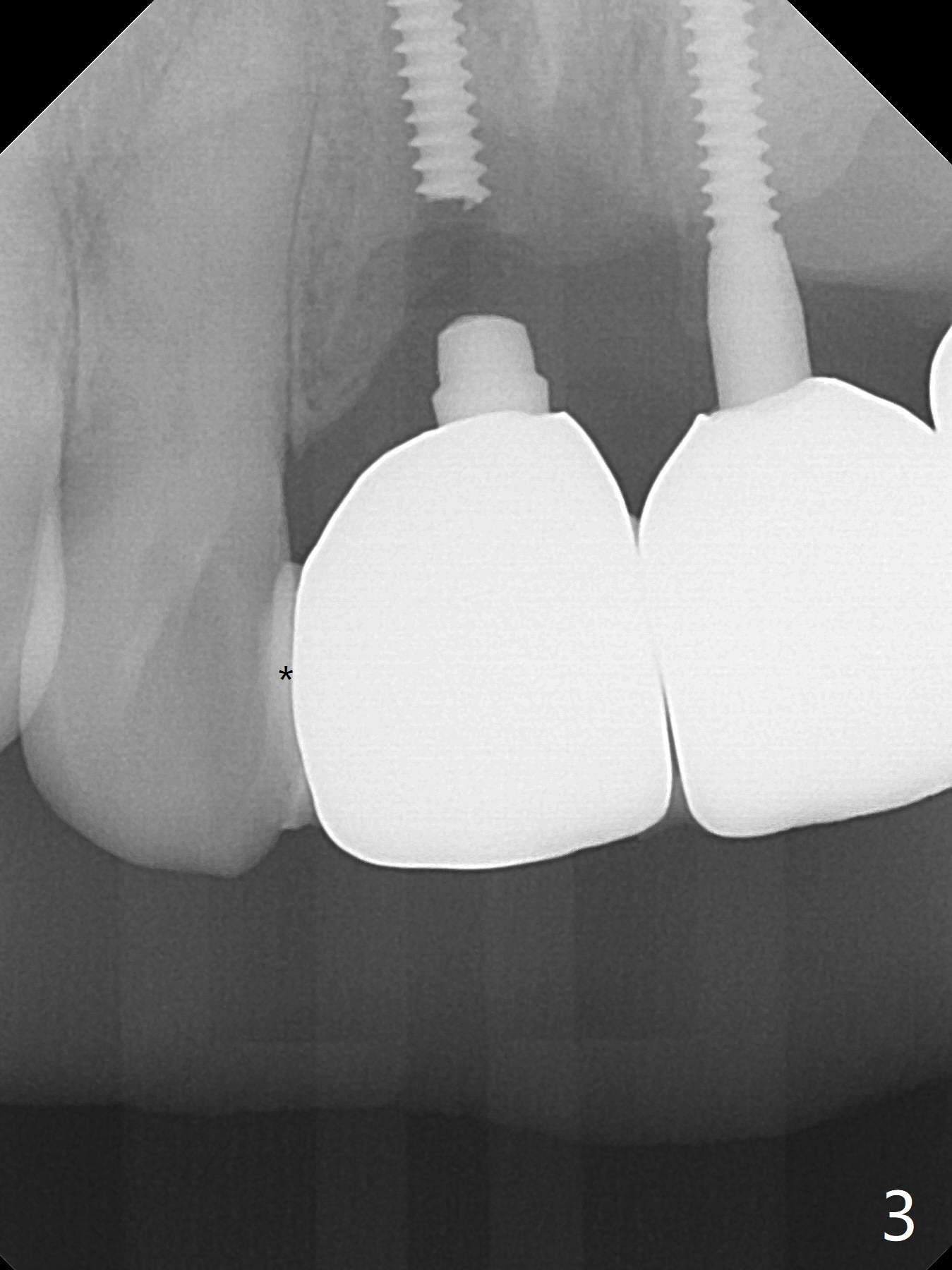
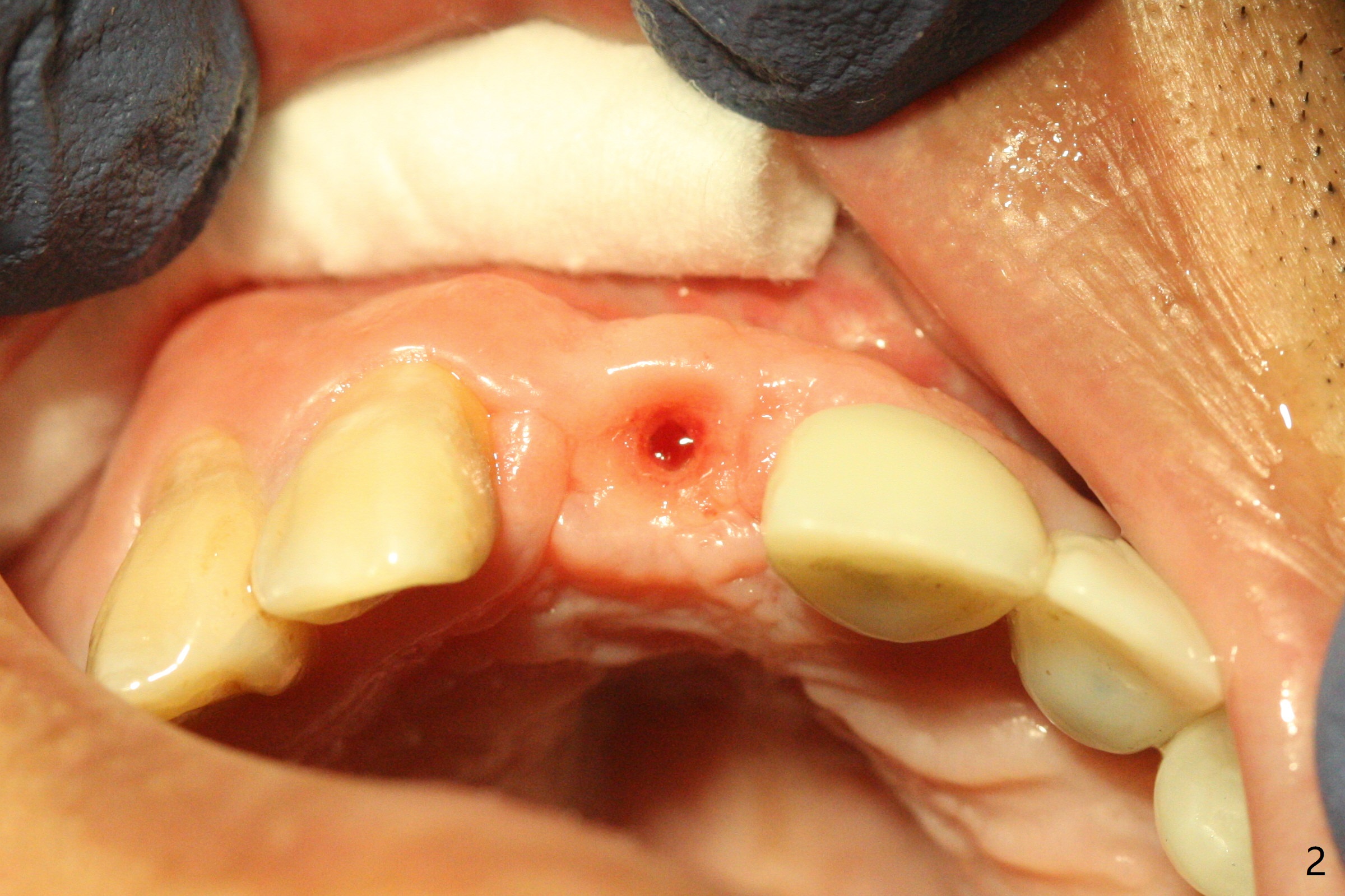
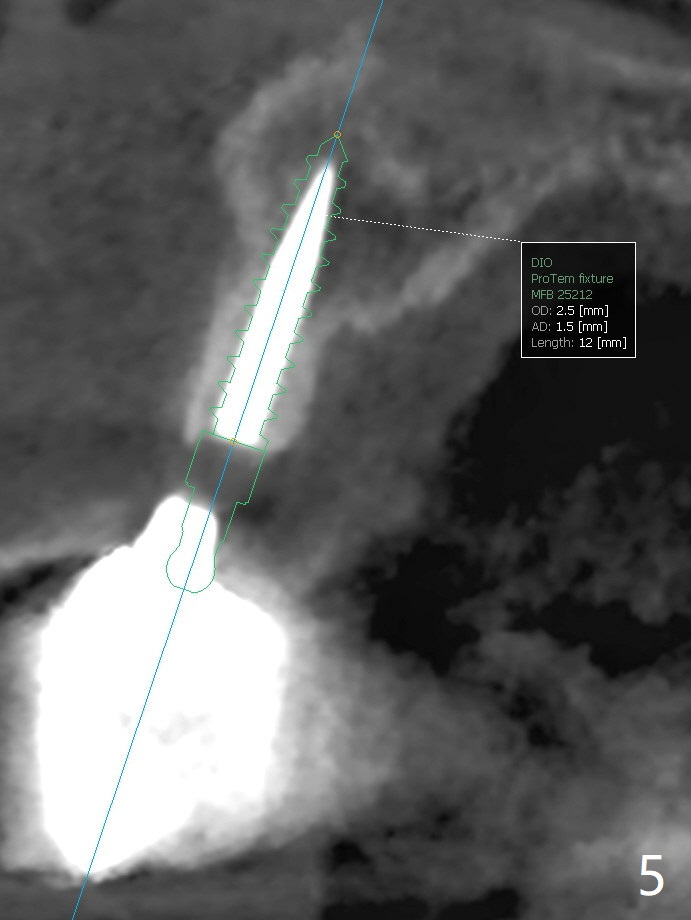
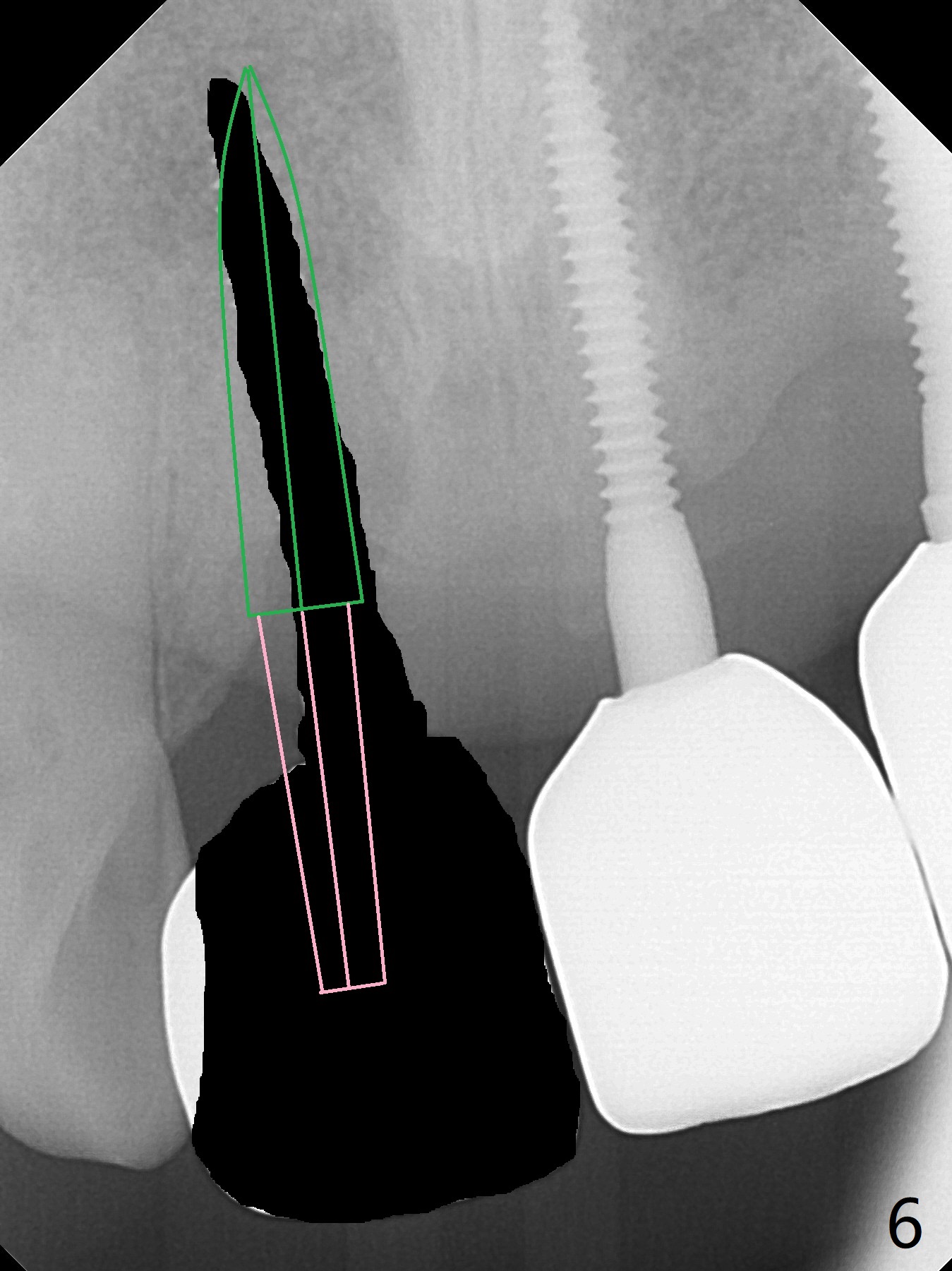
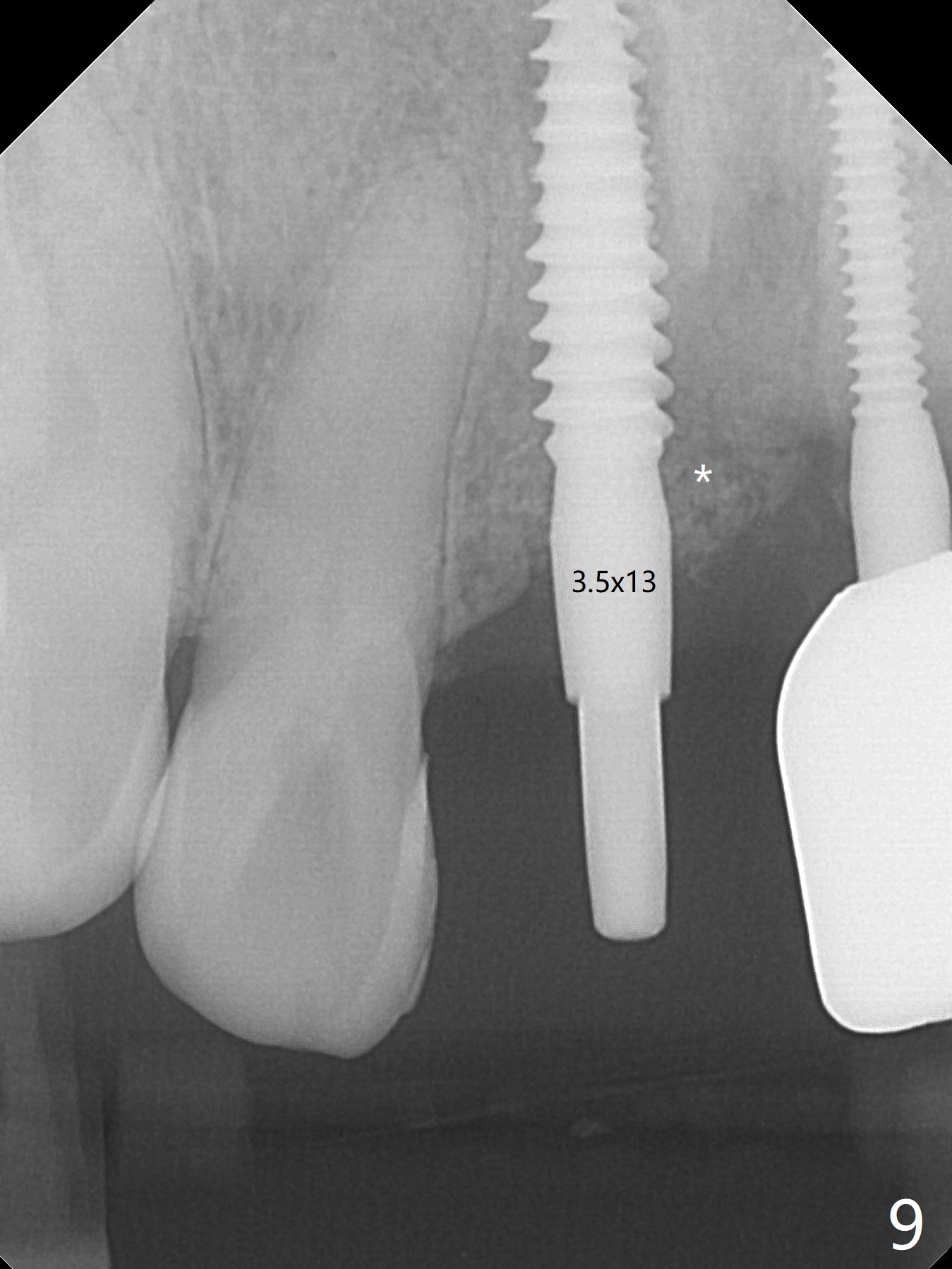
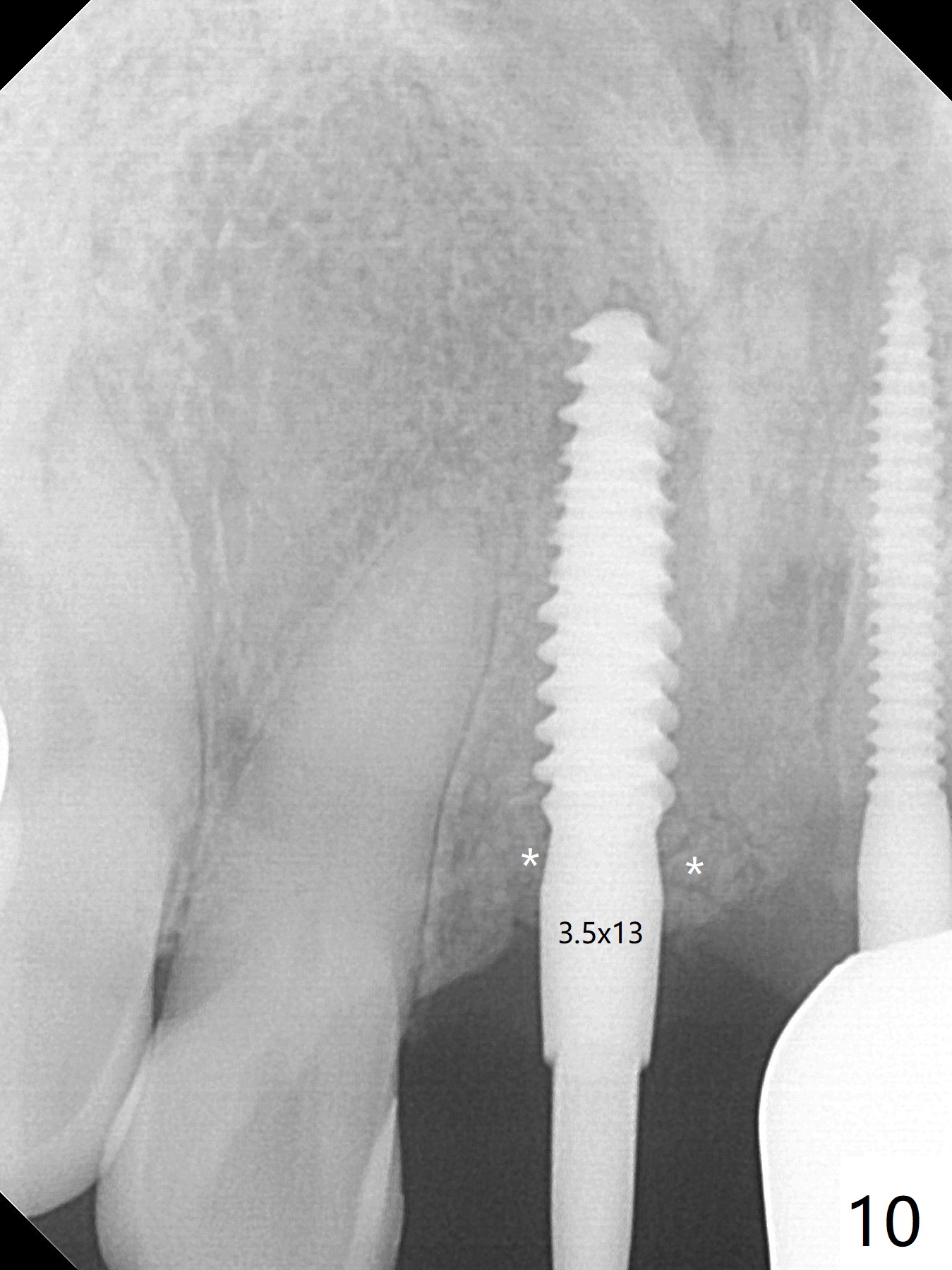
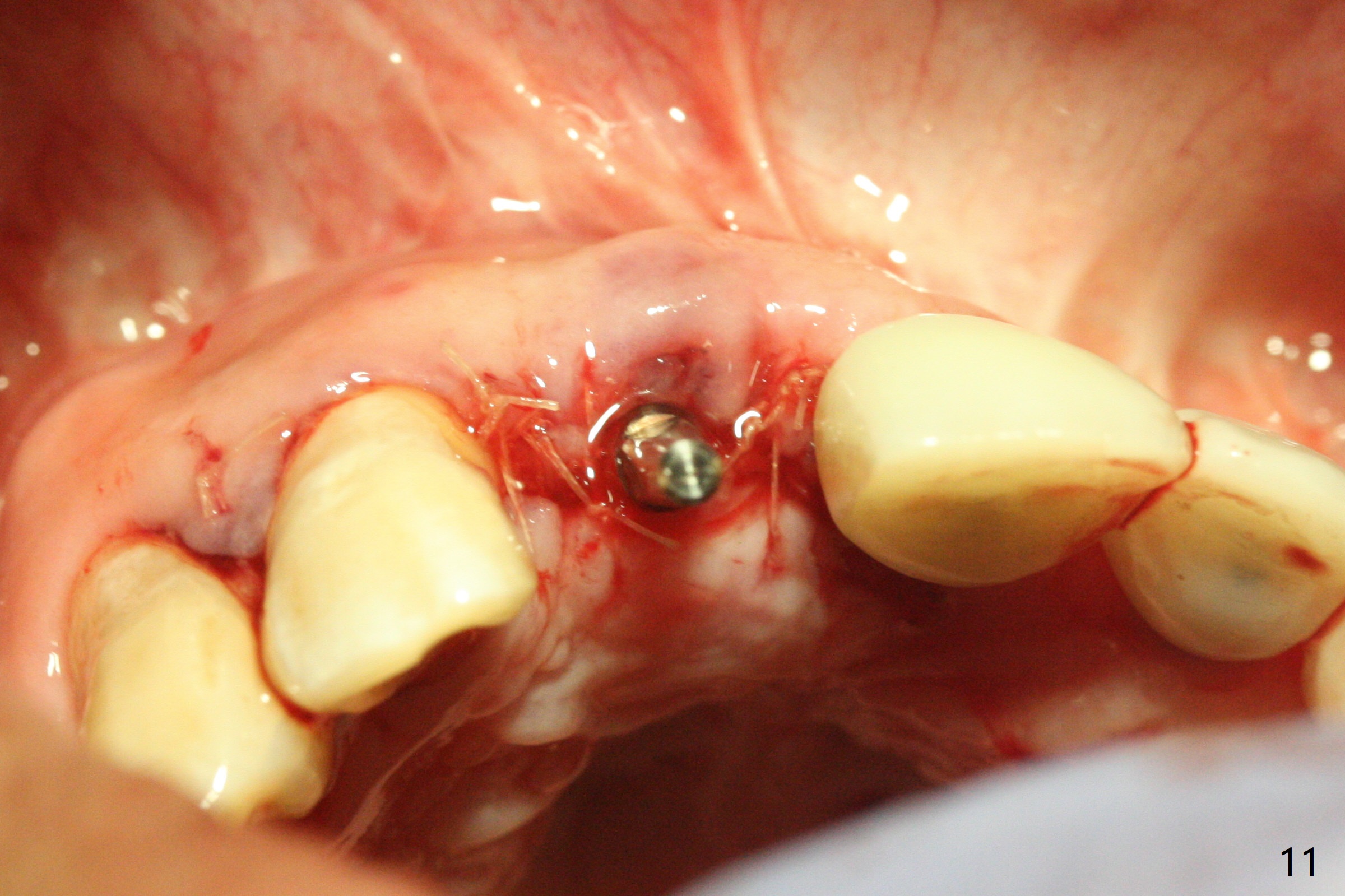
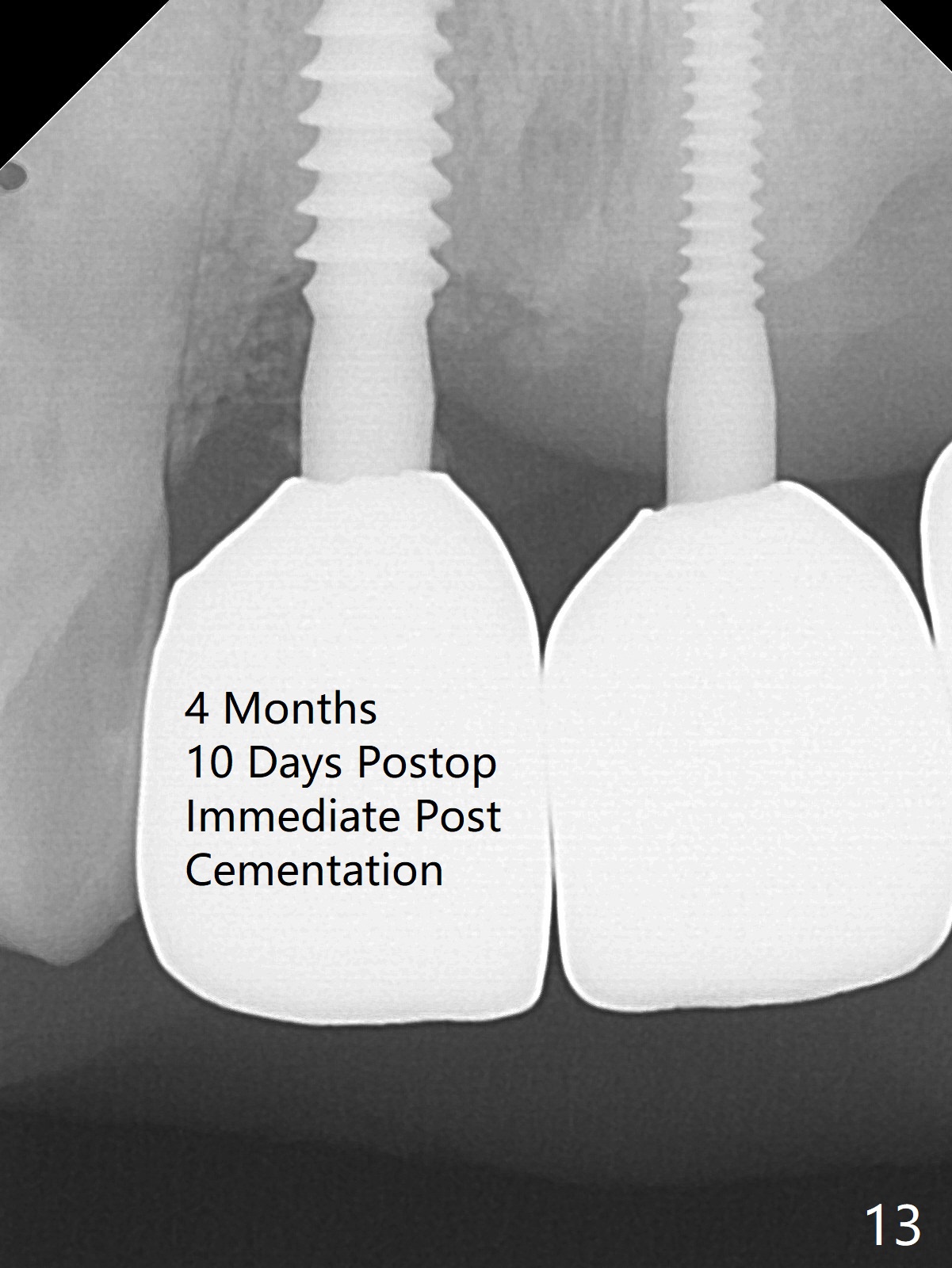
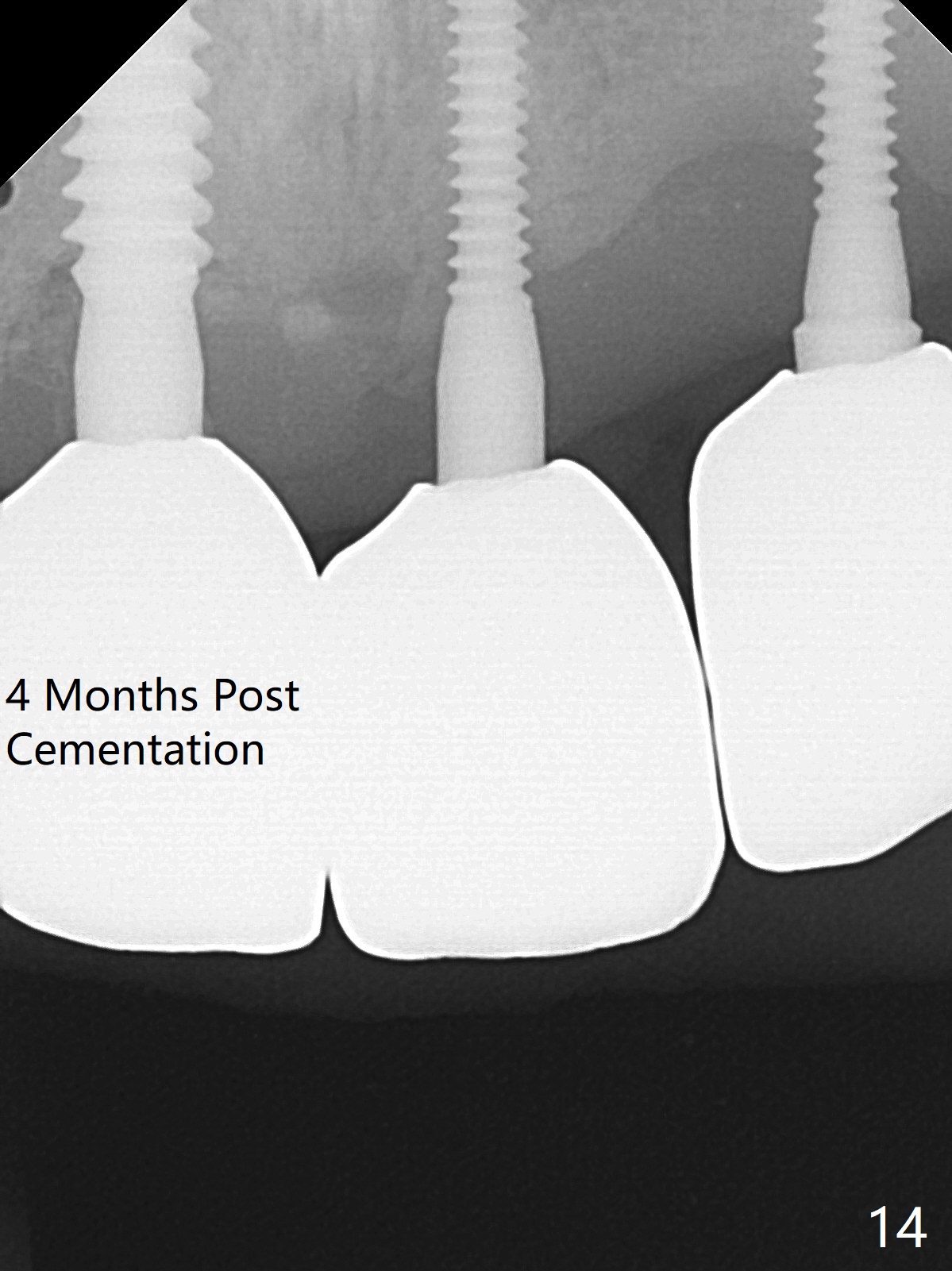
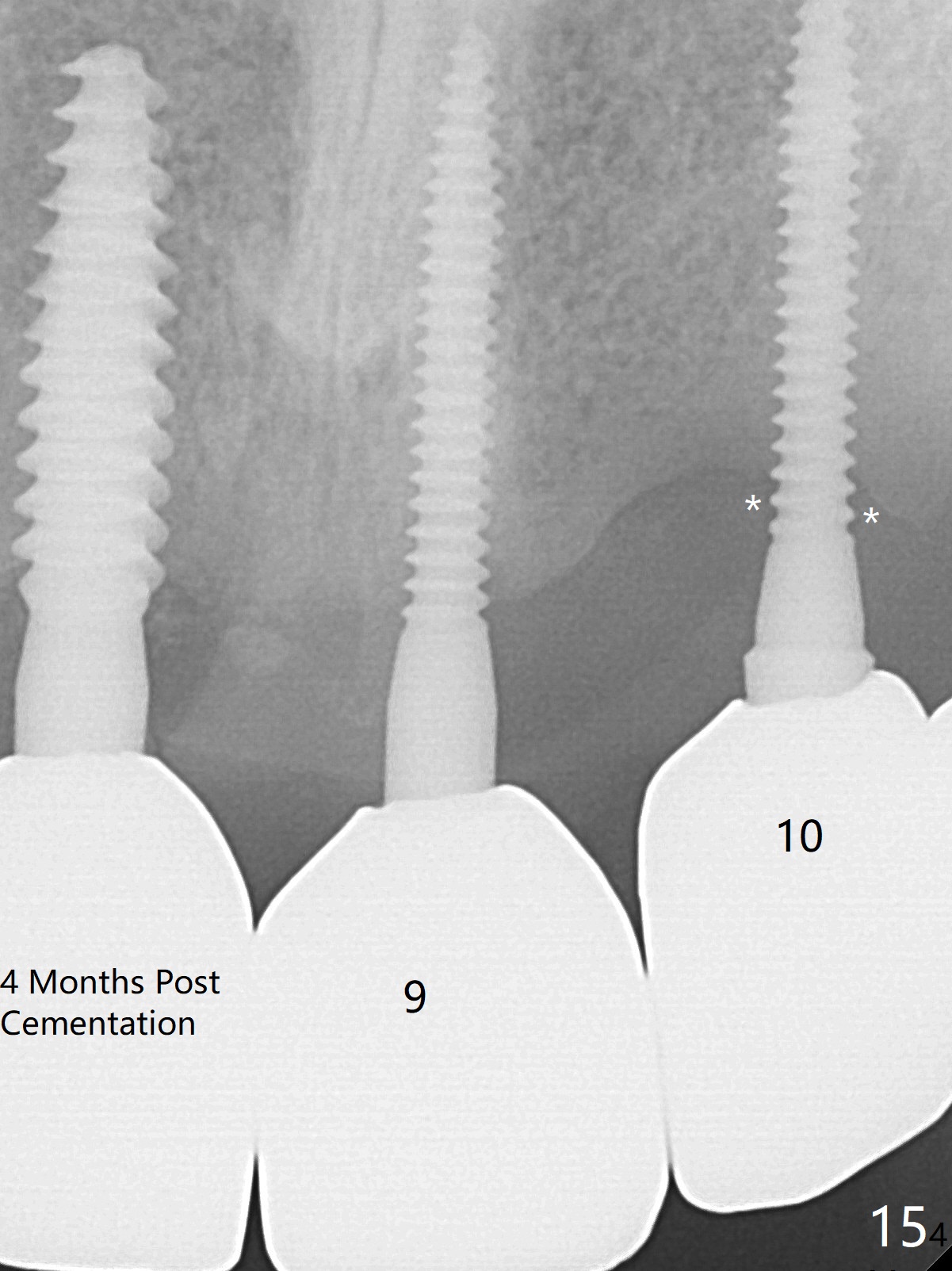
A 43-year-old man has 6 of 1-piece implants in the maxilla (#8-13). His daughter's head hits his upper anterior teeth 7 months post cementation. Exam shows that the tooth #7 has mild percussion. Nine months later the implant crown at #8 becomes displaced and loose when he bites apple (Fig.1 arrow). Forceps are used to remove the crown, leaving a concave implant site (Fig.2). After the crown is bonded to the neighboring tooth/implant crown (Fig.3 *), the patient feels pain from the neighboring tooth. The alveolus is 4.3 mm wide (Fig.4 (2.9 mm preop)), allowing 2.5 or 3.0 mm immediate implant re-placement (Fig.5). A 2.0/3.0 mm trephine bur will be used for implant removal. Try to place the new implant slightly distal to improve the trajectory (Fig.6). Particulate and/or onlay graft is an option. Prepare dummy implants. As planned, the fractured implant is removed by using a 2.0/3.0 mm trephine bur following incision (Fig.7). After use of Lindamann bur to remove the distal bone, a 3x14(4) mm dummy implant is placed with 20 Ncm (Fig.8). A longer implant could be used (3x16(2 or 4) mm), but a 3.5x13 mm 1-piece implant is placed with ~ 50 Ncm after use 3.0 mm drill (Fig.9,10). Allograft is placed around the implant (Fig.9,10 *), followed by Amnion-Chorion membrane and 5-0 PGA sutures (Fig.11). Allograft placed around the implant (Fig.9 *) appears to be able to prevent implant thread exposure 4 months postop (Fig.12). PA is taken when the crown is cemented (Fig.13). Four months postop cementation of #8 crown, the patient returns because of #9 mobility (Fig.14). In fact the implant fractures when the loose crown is removed with forceps; there is bone loss at #10. Bone graft will be placed at #10 with sticky bone (PRFx1), while the implant at #9 is redo. The ridge is wide enough for a 3.5x10 mm implant (Fig.16 (CT taken when #8 implant fractured)). Also prepare Tatum angled 1-piece implant. The 2 mm implant is too thin when occlusion contact at #10-13 is incomplete. The crowns will be redone when the implant at #9 is osteointegrated.