

.jpg)


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Aborted Shield I
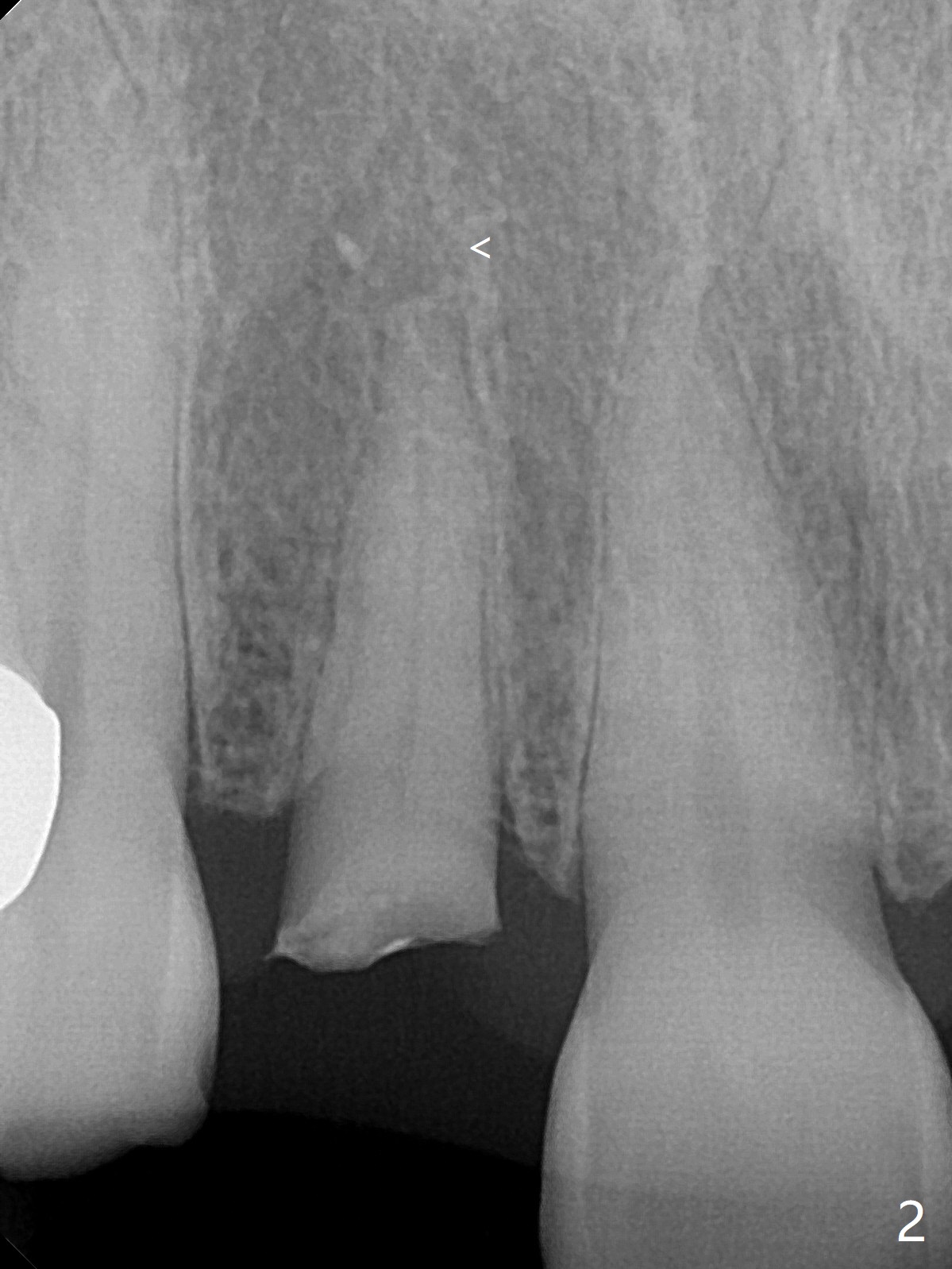
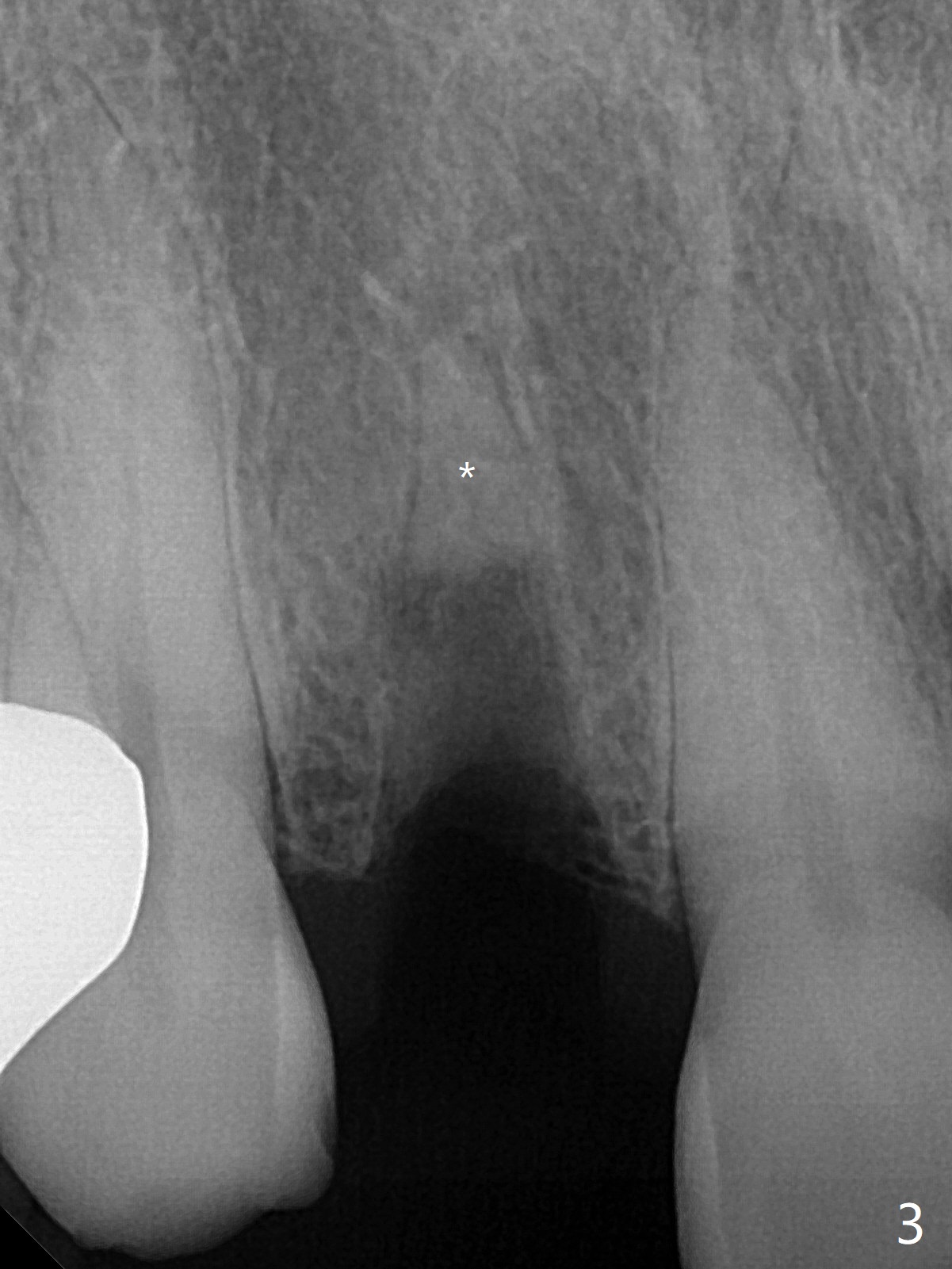
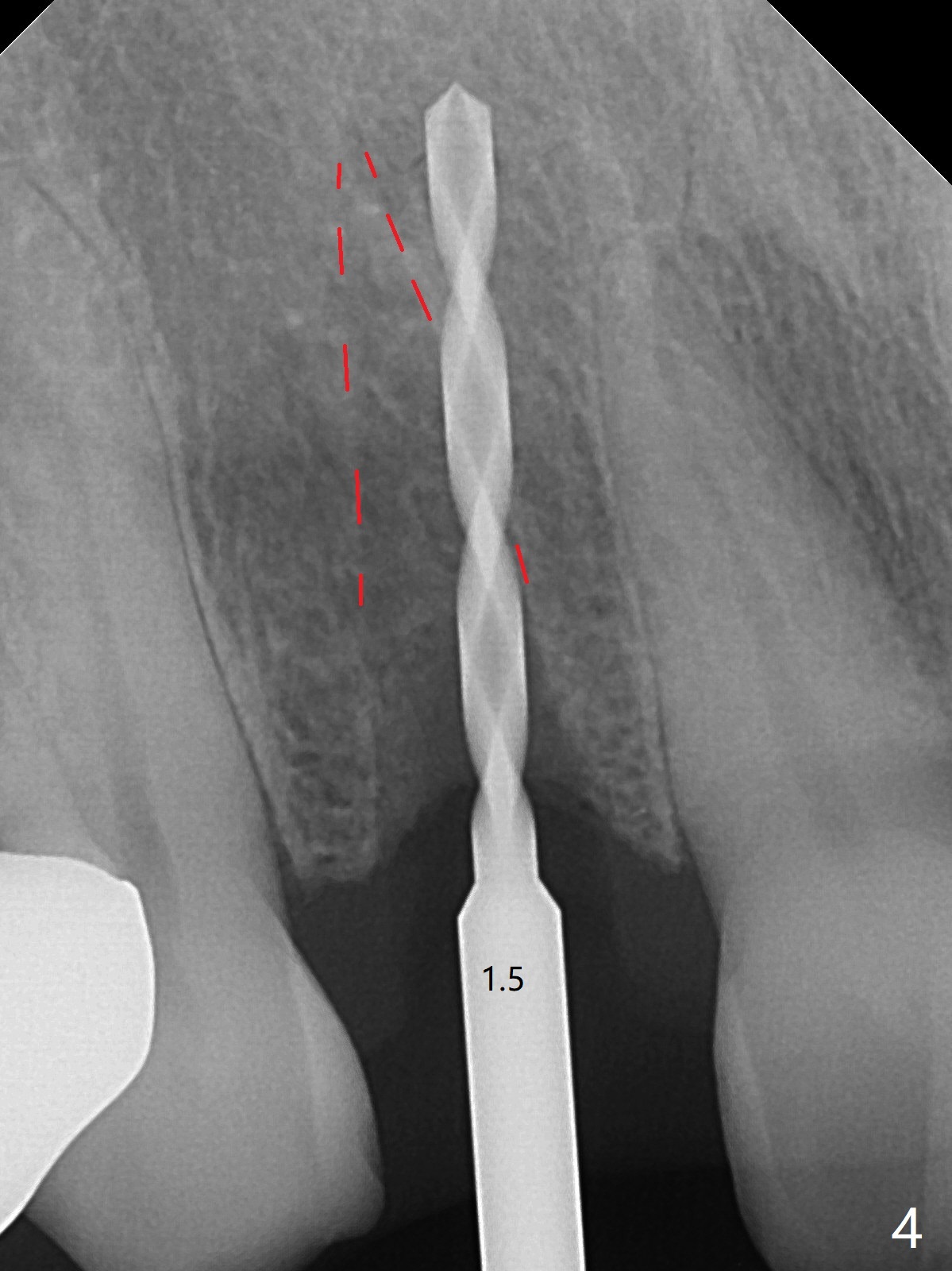
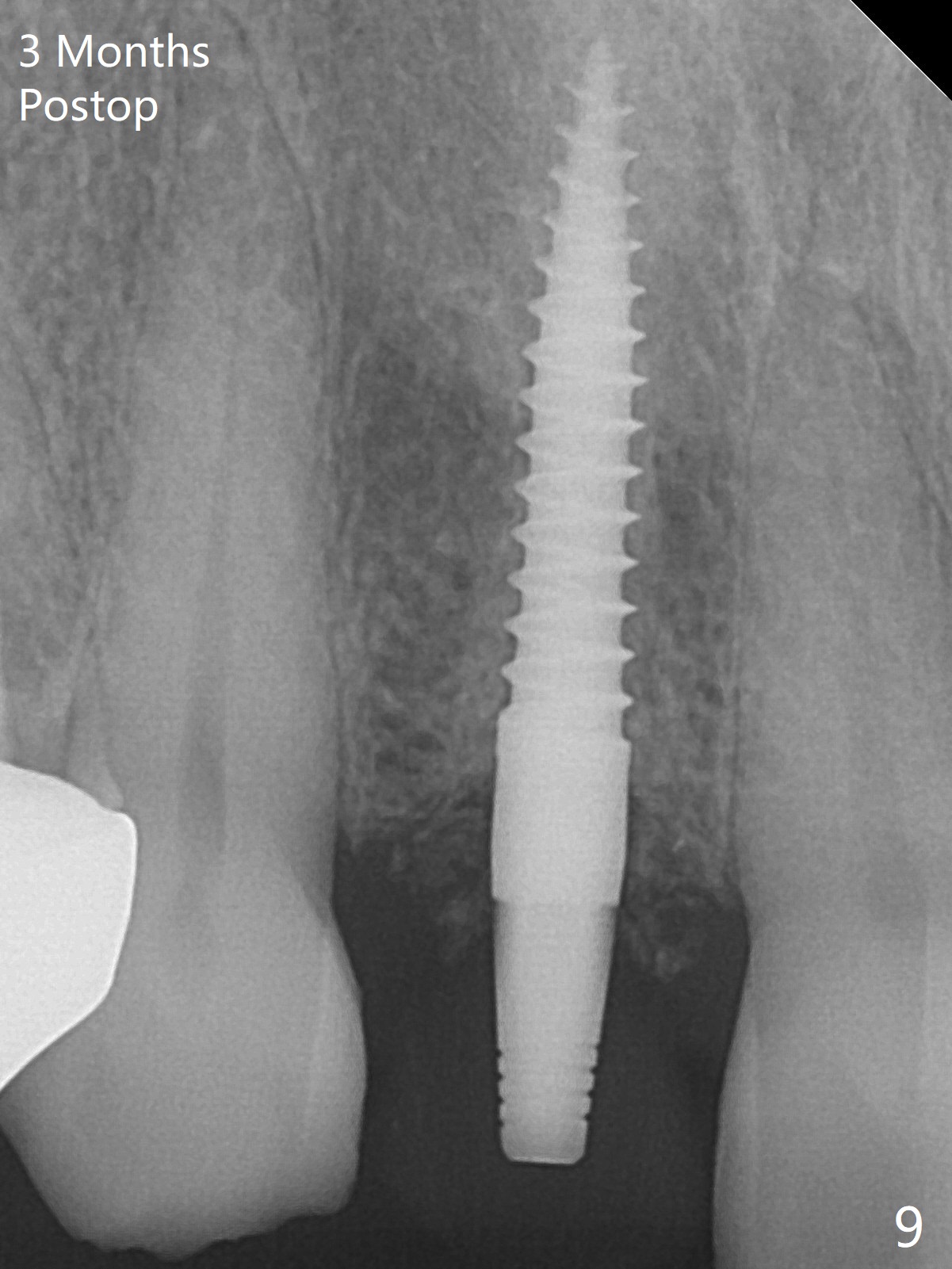
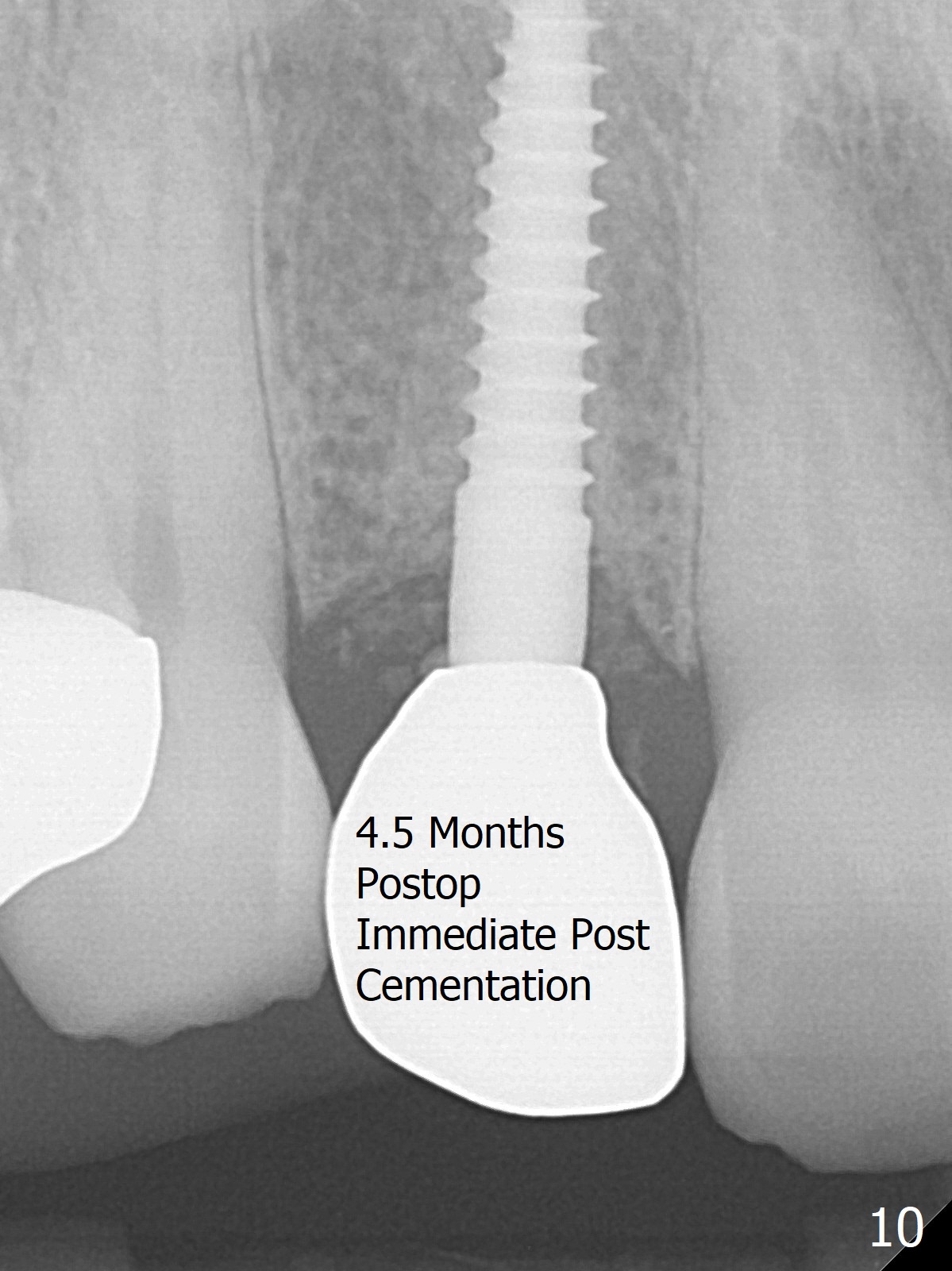
The rebonded crown at #7 debonds in a few days. There is deep anterior overbite and buccal concavity (Fig.1 *). The equi-gingival fracture (Fig.1,2) seems difficult to restore considering lack of posterior support (lower RPD in Fig.1). Buccal shield is tried in spite of the long root. It is not easy to tell whether the infected apex is removed due to the deep socket. In fact the apical buccal plate perforates because of use of surgical handpiece. Finally the buccal shied is removed. PA confirms the retained apex (Fig.3 *). The initial osteotomy with 1.5 mm drill in place is off trajectory (Fig.4). After adjustment of the trajectory of osteotomy (Fig.5), a 3x16(2) mm 1-piece implant is placed within normal limit (10-15 Ncm, Fig.6)). In fact bone graft is placed before (Fig.6,7 arrowhead; to repair apical buccal plate perforation) and after (Fig.6 *) implantation. The gingiva (including papillae) remains normal around the provisional 3 months postop (Fig.8). The bone graft becomes more organized 3 months postop (Fig.9) and continues to do so 4.5 months postop (Fig.10).
Return to Upper Incisor Immediate Implant Trajectory II Shield
Xin Wei, DDS, PhD, MS 1st edition 10/28/2019, last revision 03/14/2020