


,%2030%20Ncm.jpg)



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Socket Shield in Narrow Space
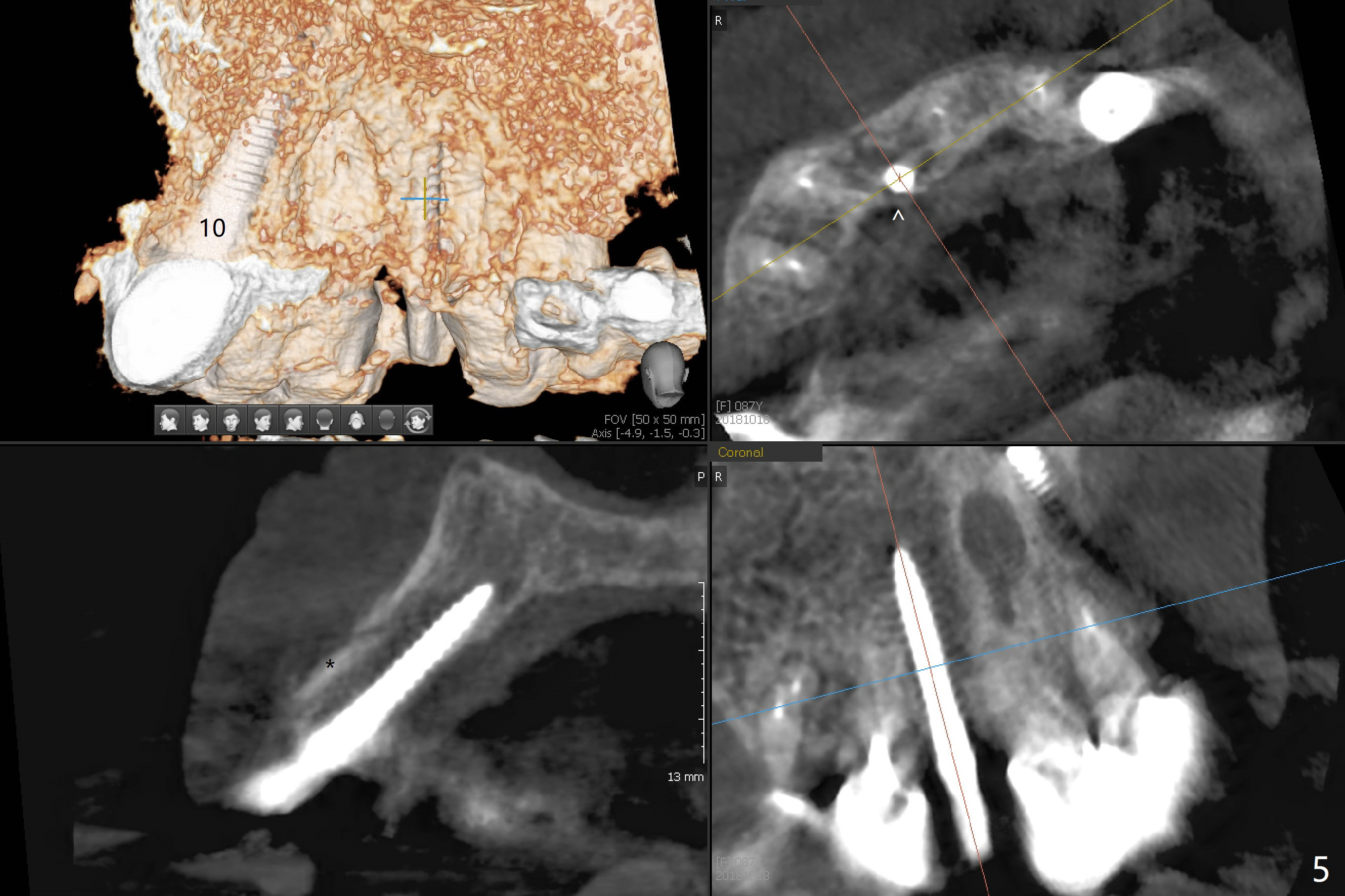
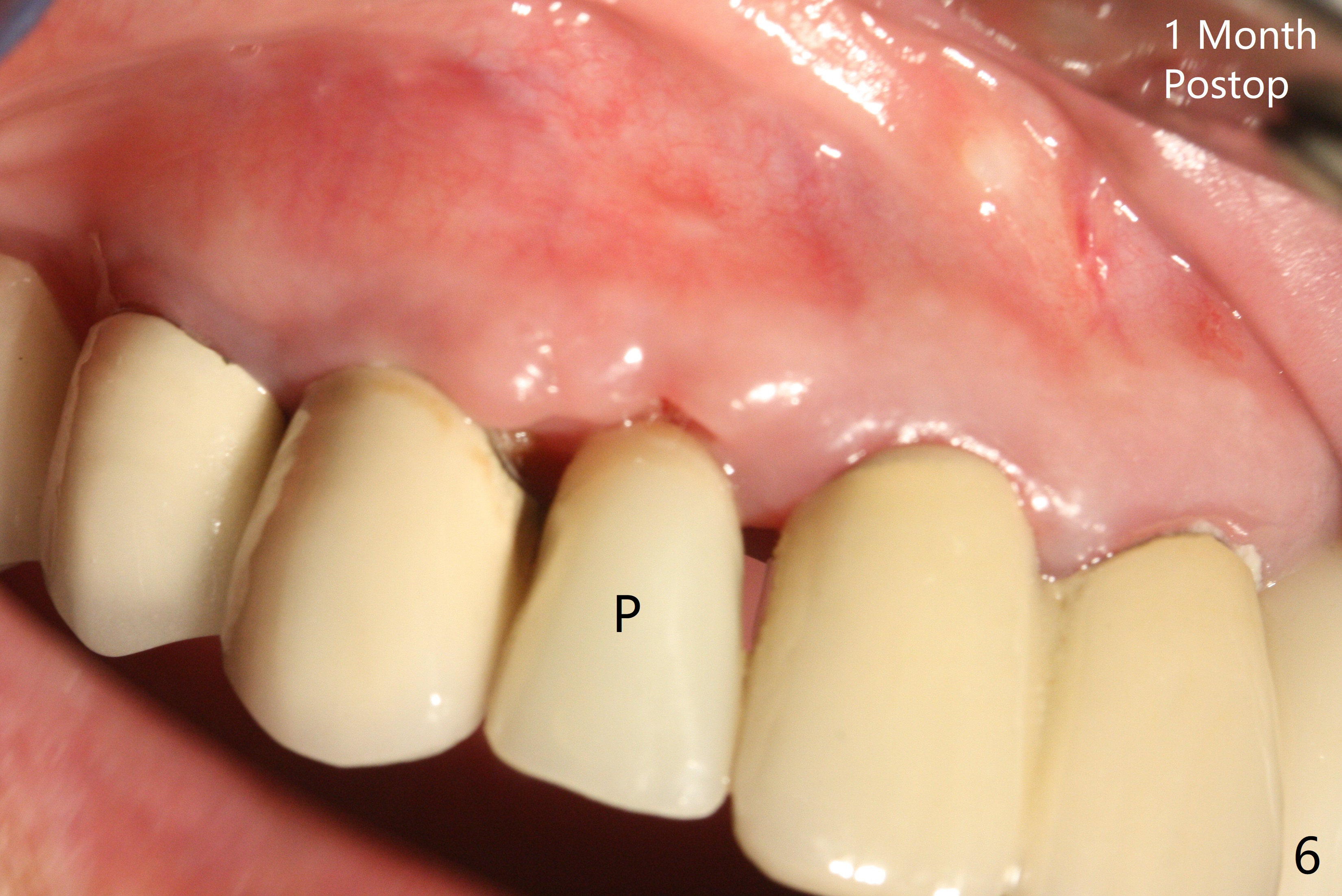
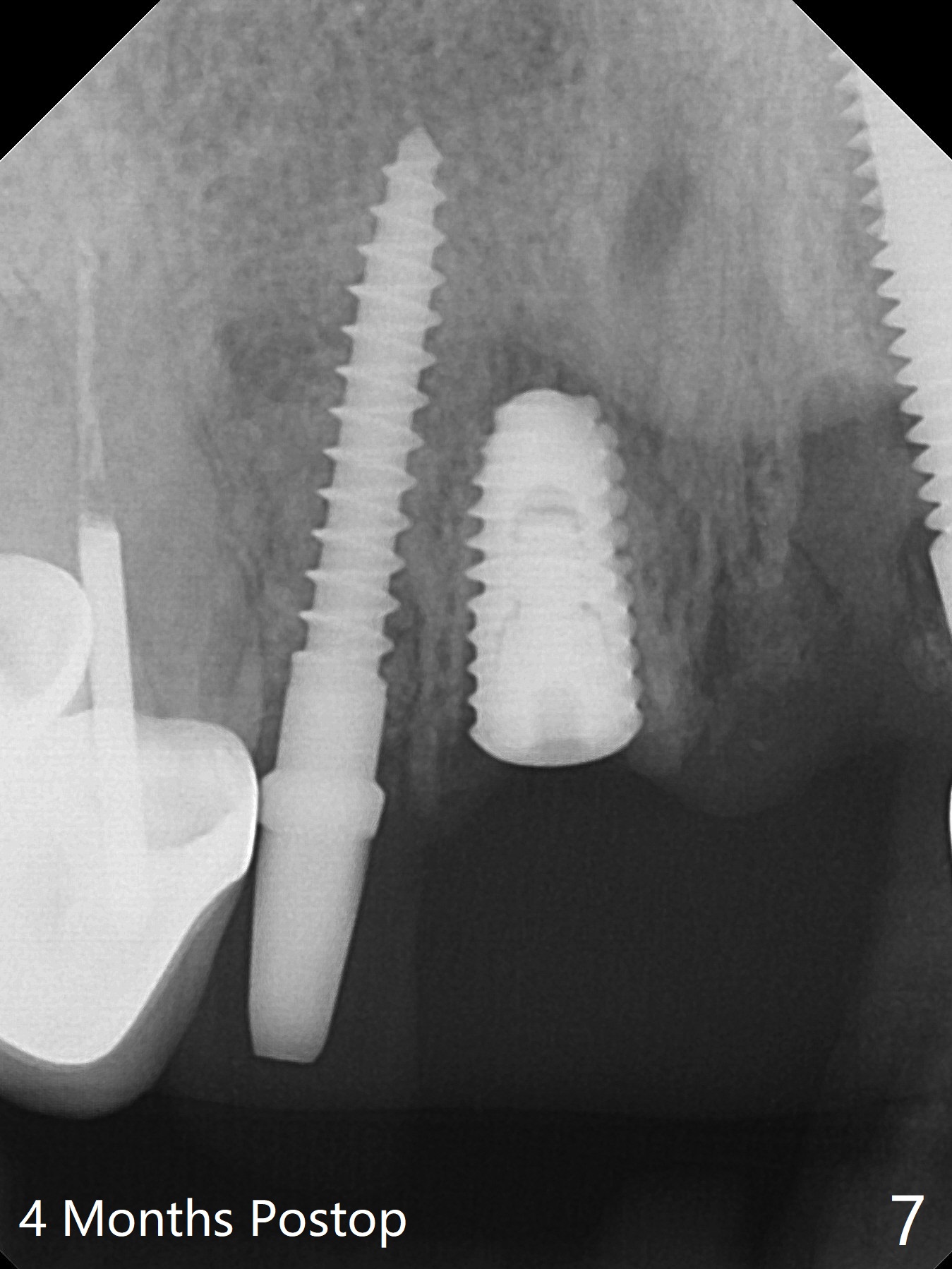
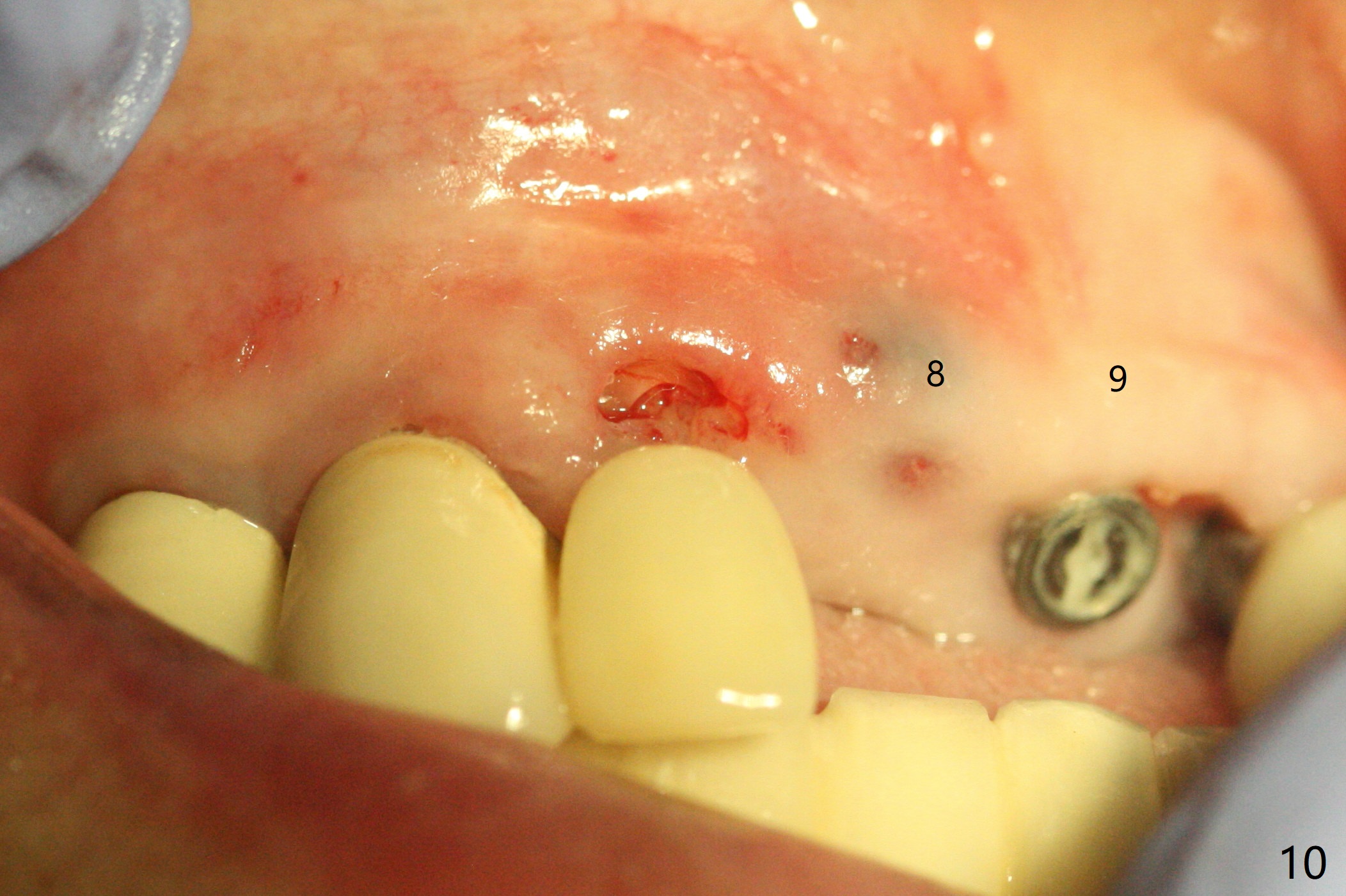
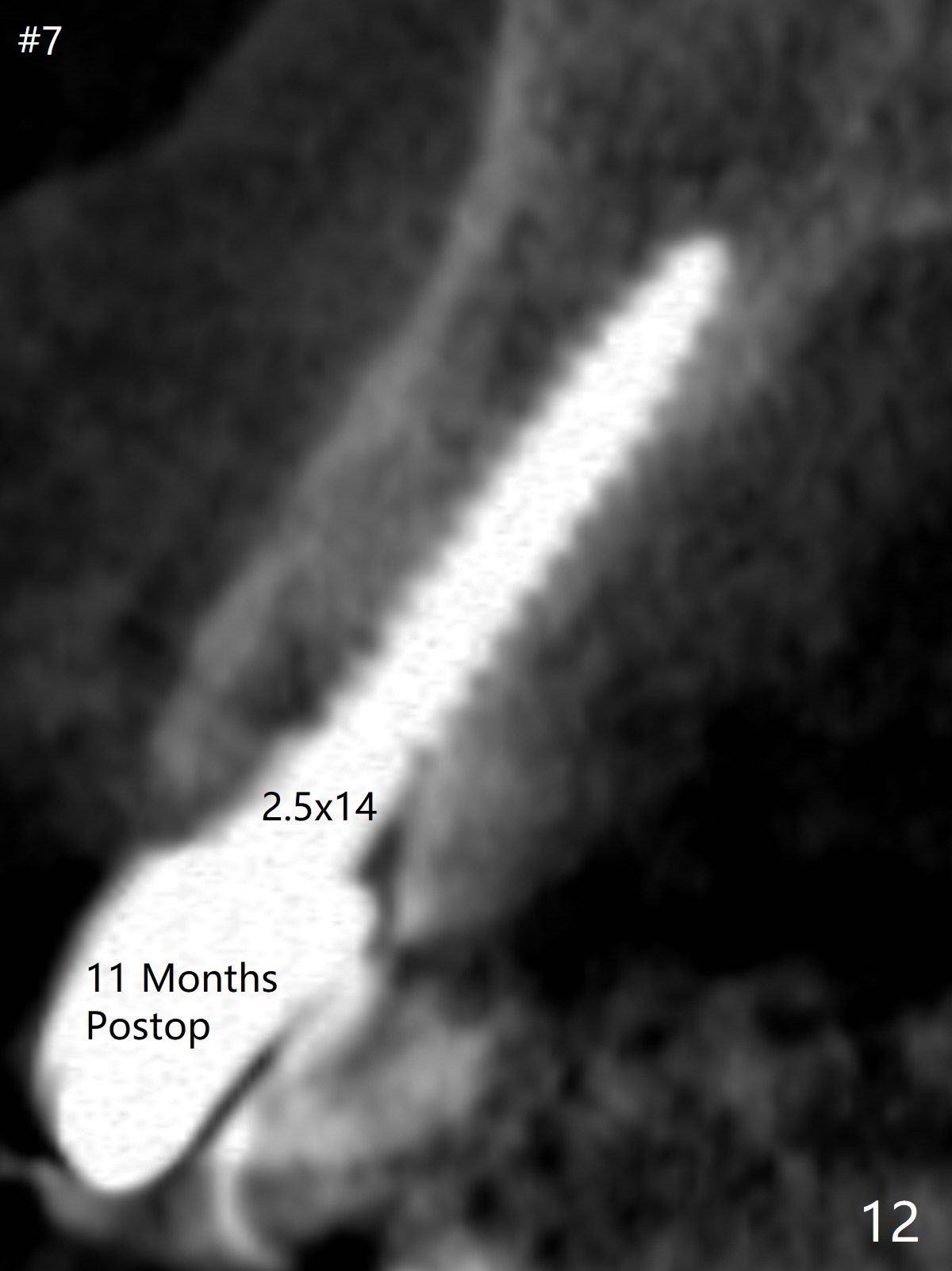
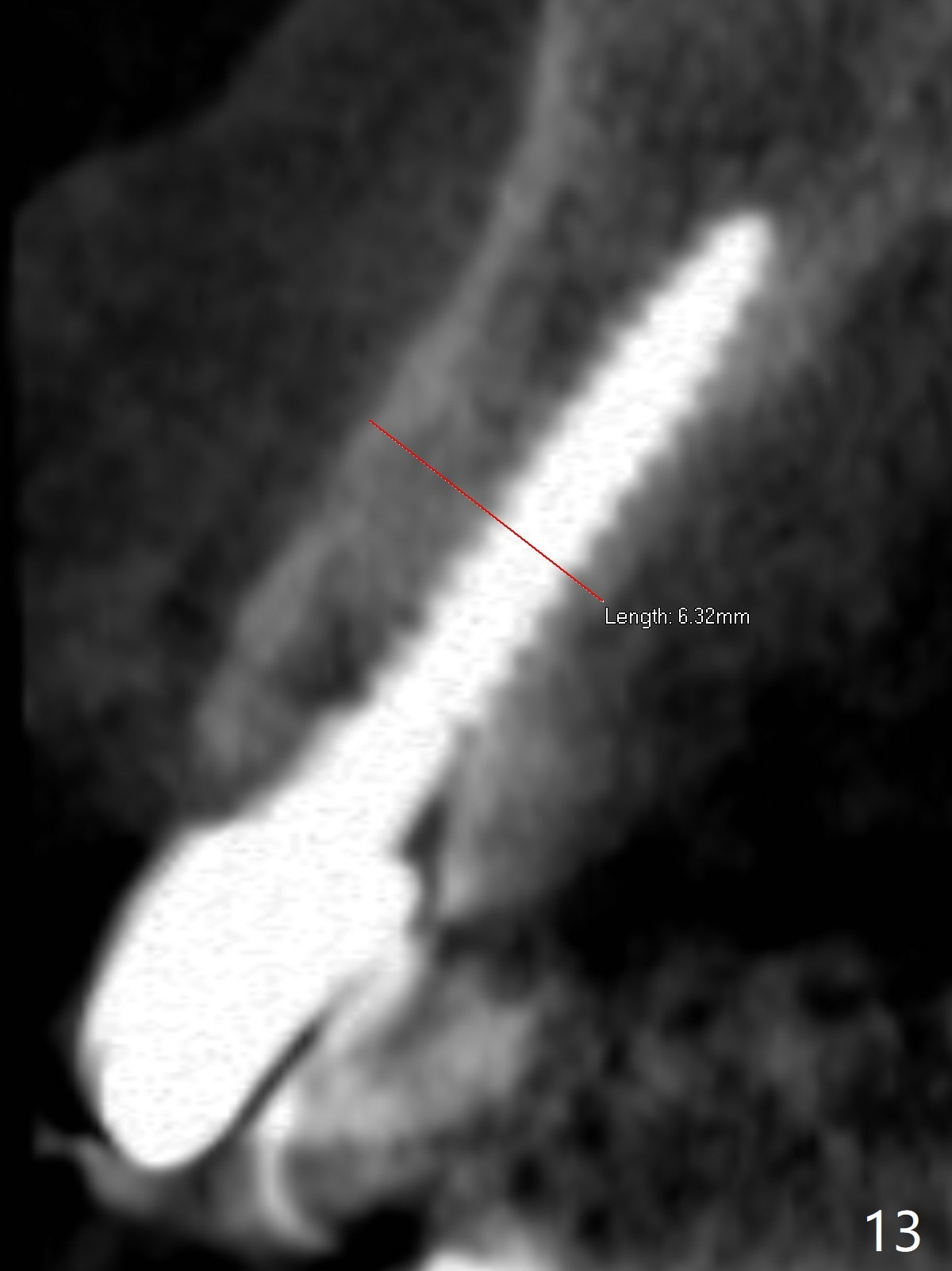
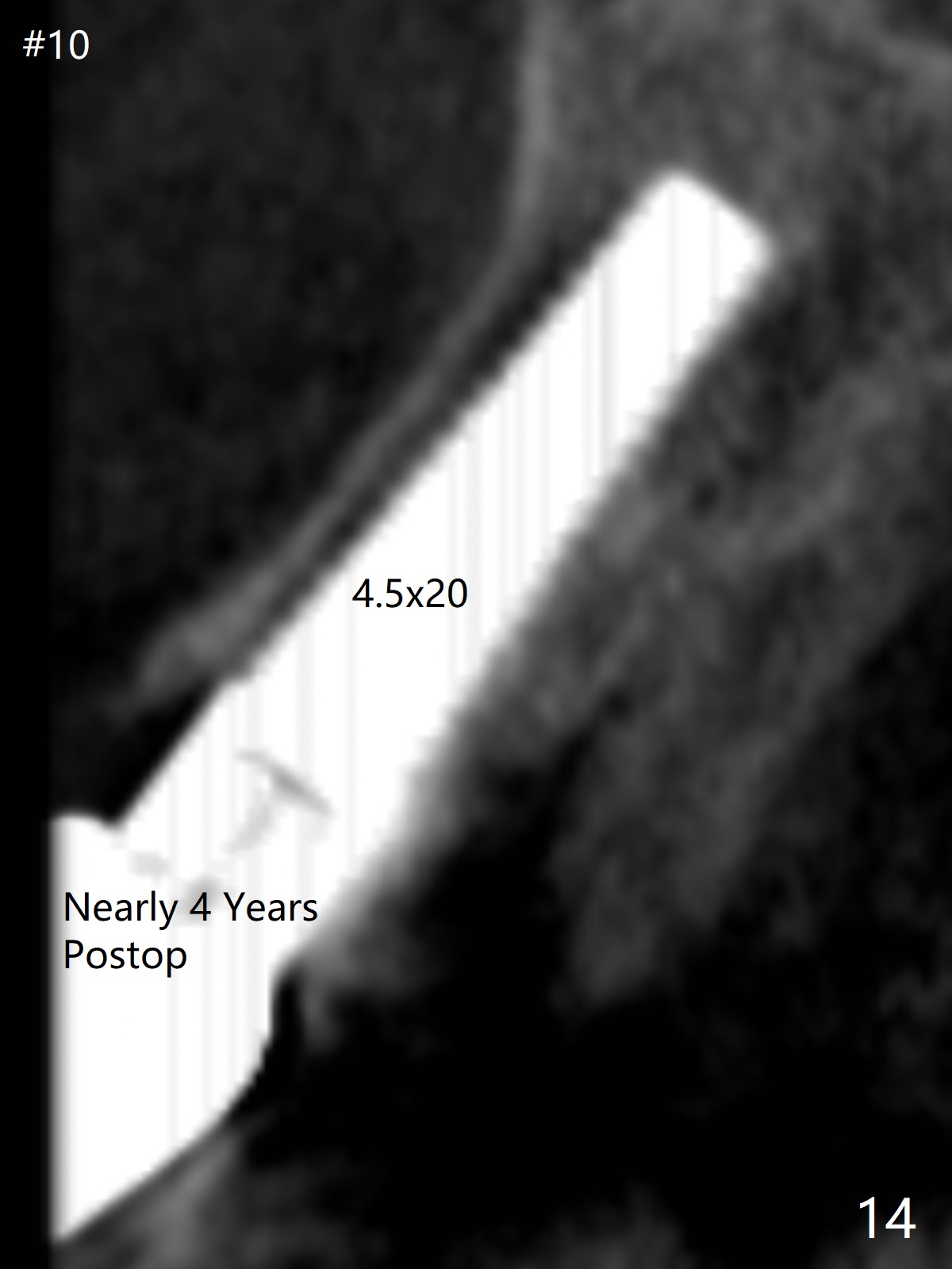
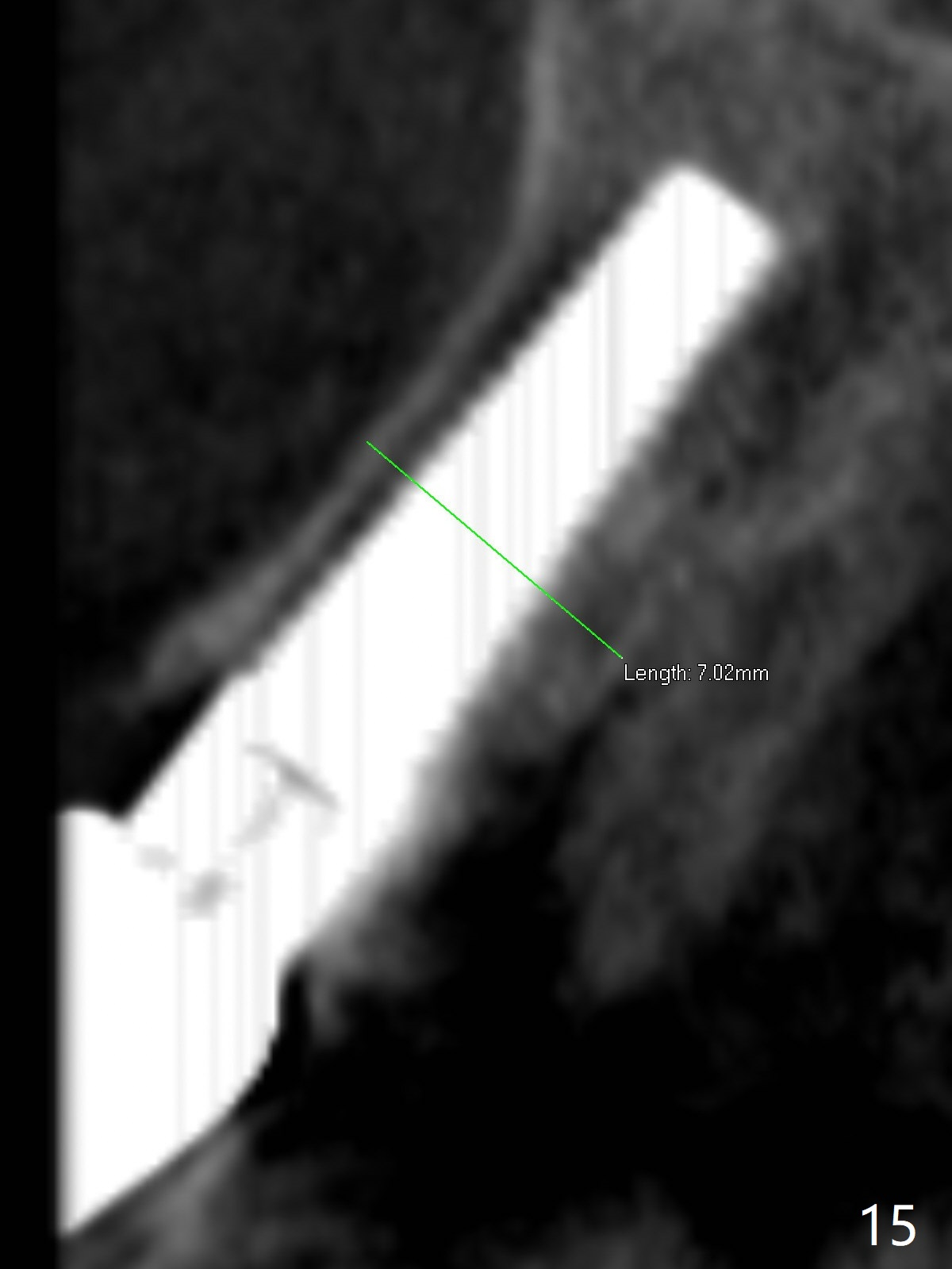
The edentulous area at #7 is narrow both buccopalatally and mesiodistally, whereas the crowns of the neighboring teeth are long (Fig.1,2). For the latter reason, it is difficult to remove the apical portion of the root, including gutta percha with surgical handpiece (Fig.3 *) for socket shield (Fig.2 *). To avoid the perspective implant touching socket shield, initial osteotomy is palatal. When a 2 mm drill is being used, the coronal end of the palatal plate starts to perforate. A 2.5x14 mm 1-piece implant is placed with 30 Ncm (Fig.4). The palatal plate is thin (Fig.5). Preop CT will help determine the position of initial osteotomy. The buccal gingiva seems to have been re-attached to the underlying alveolus and the provisional 1 month postop (Fig.6). The teeth #8 and 9 fracture (an implant is placed at #8 and bone graft at #9, while the implant at #7 is osteointegrating (Fig.7). In fact the shield is exposed without symptom. A year postop, another dental provider sends a photo of apparently hemorrhagic gingiva around #7 crown (Fig.8). A few days later with oral hygiene instruction, the gingiva around the exposed root piece is healthy (Fig.9). The root surface is reduced; with socket shield, there is no buccal plate collapse; in contrast the neighboring buccal plate (at #8 and 9) is concave (Fig.10). There is minimal exposure 11 days postop (Fig.11). The gingiva palatal to the shield is erythematous, a possible sign of periimplantitis. The socket shield at #7 appears to be fused with the buccal plate 11 months postop (Fig.12), as compared to the implant at #10 nearly 4 years postop (Fig.14). The buccopalatal widths at #7 and 10 are equivalent (Fig.13,15).
Return to Upper Incisor Immediate Implant, Trajectory, Socket Shield, 10 6 Xin Wei, DDS, PhD, MS 1st edition 10/18/2018, last revision 07/11/2021